You might also like
- Covid19 y CardioDocument4 pagesCovid19 y CardioNestor Alonso Lopez RubioNo ratings yet
- Stroke 2Document30 pagesStroke 2somyahNo ratings yet
- Clinical Characteristics and Risk Factors of Cardiac Involvement in COVID-19Document11 pagesClinical Characteristics and Risk Factors of Cardiac Involvement in COVID-19Yerlis OspinoNo ratings yet
- InternacionalDocument9 pagesInternacionalbryan ronaldNo ratings yet
- Artikel Covid-19Document9 pagesArtikel Covid-19nhshivani532000No ratings yet
- Myocarditis CovidDocument7 pagesMyocarditis CovidbagholderNo ratings yet
- Pathophysiology of Cardiovascular Complications in COVID-19Document11 pagesPathophysiology of Cardiovascular Complications in COVID-19Salsabila AstianiNo ratings yet
- Journal Reading Muhamad Fakhri PPDS JantungDocument24 pagesJournal Reading Muhamad Fakhri PPDS JantungLycka AkaishaNo ratings yet
- Adults 6Document7 pagesAdults 6Bshara SleemNo ratings yet
- Arythmie CovidDocument7 pagesArythmie CovidrakotonirinaNo ratings yet
- Stroke As A Neurological Complication of COVID-19: A Systematic Review and Meta-Analysis of Incidence, Outcomes and PredictorsDocument13 pagesStroke As A Neurological Complication of COVID-19: A Systematic Review and Meta-Analysis of Incidence, Outcomes and PredictorsChintya Anugrah SuhendraNo ratings yet
- J Jacbts 2021 10 011Document15 pagesJ Jacbts 2021 10 011Martha CeciliaNo ratings yet
- Jurnal Chen Et AlDocument31 pagesJurnal Chen Et AlUtami MNo ratings yet
- Articulo de Fisiopatología Tombosis en Tiempos de Covid Una Mini RevisiónDocument12 pagesArticulo de Fisiopatología Tombosis en Tiempos de Covid Una Mini RevisiónMayker Armando Carbo BazurtoNo ratings yet
- Cerebrovascular Complications of COVID-19: Brief ReportDocument5 pagesCerebrovascular Complications of COVID-19: Brief ReportAmandaNo ratings yet
- DunnoDocument8 pagesDunnoprastiaNo ratings yet
- Miocarditis y Covid-19Document8 pagesMiocarditis y Covid-19Jesús Evangelista GomerNo ratings yet
- 1.clinical Characteristics of 28 PatientsDocument7 pages1.clinical Characteristics of 28 PatientsTeguh WibowoNo ratings yet
- Journal Pre-Proof: Nutrition, Metabolism and Cardiovascular DiseasesDocument28 pagesJournal Pre-Proof: Nutrition, Metabolism and Cardiovascular Diseasessameer sahaanNo ratings yet
- 5 Huang2020Document10 pages5 Huang2020ANGEL DANIEL REYES FALCONNo ratings yet
- Jamaneurology Merkler 2020 Oi 200057 1604530429.19867Document7 pagesJamaneurology Merkler 2020 Oi 200057 1604530429.19867Satyaalfa PanggabeanNo ratings yet
- Jamacardiology Puntmann 2020 Oi 200057 1605207404.62135Document9 pagesJamacardiology Puntmann 2020 Oi 200057 1605207404.62135Faizal MusthofaNo ratings yet
- TAC COVID 19. LEC-S3-SEM1pdfDocument9 pagesTAC COVID 19. LEC-S3-SEM1pdfJimena Obregon GarciaNo ratings yet
- LONG COVID IssaDocument2 pagesLONG COVID IssaIchlasul MadriddistaNo ratings yet
- Estudo DiabetesDocument9 pagesEstudo DiabetesFulano de TalNo ratings yet
- Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, ChinaDocument7 pagesDysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, Chinacika daraNo ratings yet
- Jamacardiology Puntmann 2020 Oi 200057Document9 pagesJamacardiology Puntmann 2020 Oi 200057Henry DanielNo ratings yet
- Dong J - Prediction For Progression Risk in Patients With COVID - 19 Pneumonia The CALL ScoreDocument7 pagesDong J - Prediction For Progression Risk in Patients With COVID - 19 Pneumonia The CALL ScoreMercedes Ah CardenasNo ratings yet
- PIIS0735675720303569Document3 pagesPIIS0735675720303569Dewianggreini DandaNo ratings yet
- Clinical Characteristics of 116 Hospitalized Patients With COVID-19 in Wuhan, China: A Single-Centered, Retrospective, Observational StudyDocument11 pagesClinical Characteristics of 116 Hospitalized Patients With COVID-19 in Wuhan, China: A Single-Centered, Retrospective, Observational Studykristina dewiNo ratings yet
- D-Dimer As A Prognostic Indicator in Critically Ill Patients Hospitalized With COVID-19 in Leishenshan Hospital, Wuhan, ChinaDocument9 pagesD-Dimer As A Prognostic Indicator in Critically Ill Patients Hospitalized With COVID-19 in Leishenshan Hospital, Wuhan, ChinadariusNo ratings yet
- Association of Procalcitonin Levels With The Progression and Prognosis of Hospitalized Patients With COVID-19Document9 pagesAssociation of Procalcitonin Levels With The Progression and Prognosis of Hospitalized Patients With COVID-19Dian Putri NingsihNo ratings yet
- Computed Tomography Features of Cerebrovascular ComplicationsDocument6 pagesComputed Tomography Features of Cerebrovascular ComplicationsBiomédica Fabiane IngrideNo ratings yet
- The Clinical and Chest CT Features Associated With Severe and Critical COVID-19 PneumoniaDocument5 pagesThe Clinical and Chest CT Features Associated With Severe and Critical COVID-19 PneumoniaNadanNadhifahNo ratings yet
- COVID 19 and Ischemic Stroke: Mechanisms of Hypercoagulability (Review)Document13 pagesCOVID 19 and Ischemic Stroke: Mechanisms of Hypercoagulability (Review)Martha OktaviaNo ratings yet
- Ijmm 47 3 4854 PDFDocument13 pagesIjmm 47 3 4854 PDFarif 2006No ratings yet
- Myocarditis and Pericarditis Following The SARS-CoV-2 Infection and COVID-19 VaccinationDocument18 pagesMyocarditis and Pericarditis Following The SARS-CoV-2 Infection and COVID-19 VaccinationStephen DonovanNo ratings yet
- 1 s2.0 S0272638620306120 ManinDocument10 pages1 s2.0 S0272638620306120 ManinrezaNo ratings yet
- COVID-19 Associated Ischemic Stroke and Hemorrhagic Stroke - Incidence, Potential Pathological Mechanism, and ManagementDocument8 pagesCOVID-19 Associated Ischemic Stroke and Hemorrhagic Stroke - Incidence, Potential Pathological Mechanism, and ManagementWilliam MilesNo ratings yet
- 2845-Article Text-24370-1-10-20210427Document10 pages2845-Article Text-24370-1-10-20210427DamNo ratings yet
- Clinical Characteristics of COVID-19 Complicated With Pleural EffusionDocument10 pagesClinical Characteristics of COVID-19 Complicated With Pleural EffusionInternal MedicineNo ratings yet
- 1 s2.0 S1930043320306208 MainDocument3 pages1 s2.0 S1930043320306208 MainRivaldy BobihuNo ratings yet
- Incidence of Deep Venous Thrombosis in Hospitalized COVID-19 Patients in Isolated de Martini Hospital Mogadishu SomaliaDocument8 pagesIncidence of Deep Venous Thrombosis in Hospitalized COVID-19 Patients in Isolated de Martini Hospital Mogadishu SomaliaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Piis0300957220301428 PDFDocument5 pagesPiis0300957220301428 PDFDabeet MoncayoNo ratings yet
- Long Covid 1Document5 pagesLong Covid 1lakshminivas PingaliNo ratings yet
- Ischemic Stroke Associated With Novel Coronavirus 2019 A Report of Three CasesDocument6 pagesIschemic Stroke Associated With Novel Coronavirus 2019 A Report of Three CasesDewianggreini DandaNo ratings yet
- Resuscitation: Effects of COVID-19 Pandemic On Out-Of-Hospital Cardiac Arrests: A Systematic ReviewDocument7 pagesResuscitation: Effects of COVID-19 Pandemic On Out-Of-Hospital Cardiac Arrests: A Systematic ReviewAchmad RyandaNo ratings yet
- Acute Cerebrovascular Disease Following COVID-19: A Single Center, Retrospective, Observational StudyDocument6 pagesAcute Cerebrovascular Disease Following COVID-19: A Single Center, Retrospective, Observational StudysomyahNo ratings yet
- Jocs 14596Document8 pagesJocs 14596Jorge Eduardo Sánchez MoralesNo ratings yet
- Coagulation Disorders in Coronavirus Infected PatientsDocument6 pagesCoagulation Disorders in Coronavirus Infected PatientsQuang TrầnNo ratings yet
- Resuscitation: In-Hospital Cardiac Arrest Outcomes Among Patients With COVID-19 Pneumonia in Wuhan, ChinaDocument6 pagesResuscitation: In-Hospital Cardiac Arrest Outcomes Among Patients With COVID-19 Pneumonia in Wuhan, ChinaOthoniel RamirezNo ratings yet
- Higher Level of Neutrophil-to-Lymphocyte Is Associated With Severe COVID-19Document12 pagesHigher Level of Neutrophil-to-Lymphocyte Is Associated With Severe COVID-19Emier HidayatNo ratings yet
- Epidemiological and Clinical Characteristics of 671 COVID-19 Patients in Henan Province, ChinaDocument11 pagesEpidemiological and Clinical Characteristics of 671 COVID-19 Patients in Henan Province, ChinaOrlando JúniorNo ratings yet
- Oksigen Andcardiac InjuryDocument9 pagesOksigen Andcardiac InjuryZakky HazamiNo ratings yet
- Jamacardiology Shi 2020 Oi 200024Document8 pagesJamacardiology Shi 2020 Oi 200024Hengki Permana PutraNo ratings yet
- Current Perspectives On Coronavirus Disease 2019 and Cardiovascular Disease: A White Paper by The JAHA EditorsDocument23 pagesCurrent Perspectives On Coronavirus Disease 2019 and Cardiovascular Disease: A White Paper by The JAHA EditorsCorina NedelcuNo ratings yet
- Automatic COVID 19 Severity Assessment From HRVDocument10 pagesAutomatic COVID 19 Severity Assessment From HRVCarlos Eduardo NorteNo ratings yet
- Explore: Shuo-Wen Hung, Yuan-Ching Liao, I-Chang Chi, Ting-Yen Lin, Yu-Chuan Lin, Hung-Jen Lin, Sheng-Teng HuangDocument6 pagesExplore: Shuo-Wen Hung, Yuan-Ching Liao, I-Chang Chi, Ting-Yen Lin, Yu-Chuan Lin, Hung-Jen Lin, Sheng-Teng HuangJOHNNo ratings yet
- Falling Stroke Rates During COVID-19 Pandemic at A Comprehensive Stroke Center: Cover Title: Falling Stroke Rates During COVID-19Document8 pagesFalling Stroke Rates During COVID-19 Pandemic at A Comprehensive Stroke Center: Cover Title: Falling Stroke Rates During COVID-19khairaniNo ratings yet
- Adults 7Document14 pagesAdults 7Bshara SleemNo ratings yet
- Adults 6Document7 pagesAdults 6Bshara SleemNo ratings yet
- Adults 1Document20 pagesAdults 1Bshara SleemNo ratings yet
- Adults 5Document5 pagesAdults 5Bshara SleemNo ratings yet
- Adults 2Document5 pagesAdults 2Bshara SleemNo ratings yet
- Microstrip Antennas: How Do They Work?Document2 pagesMicrostrip Antennas: How Do They Work?Tebogo SekgwamaNo ratings yet
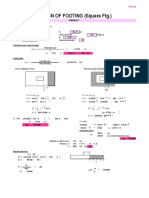
- Design of Footing (Square FTG.) : M Say, L 3.75Document2 pagesDesign of Footing (Square FTG.) : M Say, L 3.75victoriaNo ratings yet
- A Job InterviewDocument8 pagesA Job Interviewa.rodriguezmarcoNo ratings yet
- Big Data Hadoop Certification Training CourseDocument12 pagesBig Data Hadoop Certification Training Courseprema vNo ratings yet
- Uncertainty-Based Production Scheduling in Open Pit Mining: R. Dimitrakopoulos and S. RamazanDocument7 pagesUncertainty-Based Production Scheduling in Open Pit Mining: R. Dimitrakopoulos and S. RamazanClaudio AballayNo ratings yet
- 02-15 QCS 2014Document17 pages02-15 QCS 2014Raja Ahmed HassanNo ratings yet
- Technical Report: Determination of The Resistance To DelaminationDocument4 pagesTechnical Report: Determination of The Resistance To DelaminationStefan NaricNo ratings yet
- VMC Ballscrew 32mm Horizontal Plane ReplacementDocument11 pagesVMC Ballscrew 32mm Horizontal Plane ReplacementMarlon GeronimoNo ratings yet
- NATIONAL DEVELOPMENT COMPANY v. CADocument11 pagesNATIONAL DEVELOPMENT COMPANY v. CAAndrei Anne PalomarNo ratings yet
- Delegation-of-Power CasesDocument35 pagesDelegation-of-Power CasesKazzy GNo ratings yet
- Instructions For Comprehensive Exams NovemberDocument2 pagesInstructions For Comprehensive Exams Novembermanoj reddyNo ratings yet
- 1849 1862 Statutes at Large 601-779Document200 pages1849 1862 Statutes at Large 601-779ncwazzyNo ratings yet
- 9MFY18 MylanDocument94 pages9MFY18 MylanRahul GautamNo ratings yet
- Affidavit To Use The Surname of The FatherDocument2 pagesAffidavit To Use The Surname of The FatherGlenn Lapitan Carpena100% (1)
- Why Is Inventory Turnover Important?: ... It Measures How Hard Your Inventory Investment Is WorkingDocument6 pagesWhy Is Inventory Turnover Important?: ... It Measures How Hard Your Inventory Investment Is WorkingabhiNo ratings yet
- Marc-André Ter Stegen PES 2021 StatsDocument1 pageMarc-André Ter Stegen PES 2021 StatsSom VasnaNo ratings yet
- The 8051 Microcontroller & Embedded Systems: Muhammad Ali Mazidi, Janice Mazidi & Rolin MckinlayDocument15 pagesThe 8051 Microcontroller & Embedded Systems: Muhammad Ali Mazidi, Janice Mazidi & Rolin MckinlayAkshwin KisoreNo ratings yet
- ISC 2008 Computer Science Paper 1 TheoryDocument8 pagesISC 2008 Computer Science Paper 1 TheoryShadowerNo ratings yet
- Asme 1417 WordDocument12 pagesAsme 1417 WordERIKA RUBIONo ratings yet
- Study On Color Fastness To Rubbing by Crock MeterDocument4 pagesStudy On Color Fastness To Rubbing by Crock Metertushar100% (5)
- Move It 3. Test U3Document2 pagesMove It 3. Test U3Fabian AmayaNo ratings yet
- SS 531 2006 Code of Practice For Lighting of Work Places Part 1 PDFDocument13 pagesSS 531 2006 Code of Practice For Lighting of Work Places Part 1 PDFEdmund YoongNo ratings yet
- Trigger: Business Process Procedure OverviewDocument11 pagesTrigger: Business Process Procedure Overviewcalalitbajaj100% (1)
- Gamesa Wind Turbine Element UpgradesDocument1 pageGamesa Wind Turbine Element Upgradesstanislav uzunchevNo ratings yet
- A Survey Report On The Preferred RestaurDocument22 pagesA Survey Report On The Preferred RestaurEIGHA & ASHLEIGH EnriquezNo ratings yet
- Types of Foundation and Their Uses in Building ConstructionDocument4 pagesTypes of Foundation and Their Uses in Building ConstructionCraig MNo ratings yet
- Smart Meter Are HarmfulDocument165 pagesSmart Meter Are HarmfulknownpersonNo ratings yet
- 10.isca RJCS 2015 106Document5 pages10.isca RJCS 2015 106Touhid IslamNo ratings yet
- 2017 Directory WO Member PagesDocument112 pages2017 Directory WO Member PagessberkowitzNo ratings yet
- University of MauritiusDocument4 pagesUniversity of MauritiusAtish KissoonNo ratings yet
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (82)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4.5 out of 5 stars4.5/5 (6)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (254)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (60)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)