You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Geopathic StressDocument17 pagesGeopathic Stressitounos100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- AnticoagulantsDocument19 pagesAnticoagulantsOsama ZbedaNo ratings yet
- CDAC DocumentDocument15 pagesCDAC DocumentShruthi DyavegowdaNo ratings yet
- Grabovoi Numbers 2 PDF FreeDocument21 pagesGrabovoi Numbers 2 PDF FreeLina AmorNo ratings yet
- UHS Pre-Enrolment Physical (Medical) Examination Form PDFDocument2 pagesUHS Pre-Enrolment Physical (Medical) Examination Form PDFReaStephanieCidNo ratings yet
- Jadwal Operasi, Selasa 26 Juli 2022Document1 pageJadwal Operasi, Selasa 26 Juli 2022Angger SatriaNo ratings yet
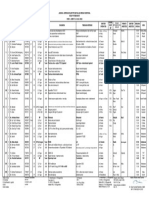
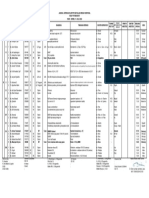
- Jadwal Operasi, Selasa 16 Agustus 2022 PDFDocument1 pageJadwal Operasi, Selasa 16 Agustus 2022 PDFAngger SatriaNo ratings yet
- Swab PCR Bayu GemilangDocument1 pageSwab PCR Bayu GemilangAngger SatriaNo ratings yet
- Assessment TN MasrukhiDocument3 pagesAssessment TN MasrukhiAngger SatriaNo ratings yet
- Pembahasan Semester 4-5 Maret 2022Document21 pagesPembahasan Semester 4-5 Maret 2022Angger SatriaNo ratings yet
- Role of Pre Operative Ureteral Stent On Outcomes of Retrograde Intra Renal Surgery (RIRS) Systematic Review and Meta Analysis of 3831 Patients and Comparison of Asian and Non Asian CohortsDocument13 pagesRole of Pre Operative Ureteral Stent On Outcomes of Retrograde Intra Renal Surgery (RIRS) Systematic Review and Meta Analysis of 3831 Patients and Comparison of Asian and Non Asian CohortsAngger SatriaNo ratings yet
- Pediatric Living Donor Liver Transplantation WithDocument21 pagesPediatric Living Donor Liver Transplantation WithAngger SatriaNo ratings yet
- Jadwal Operasi, Senin 25 Juli 2022 PDFDocument1 pageJadwal Operasi, Senin 25 Juli 2022 PDFAngger SatriaNo ratings yet
- Jadwal Operasi, Rabu 10 Agustus 2022 PDFDocument1 pageJadwal Operasi, Rabu 10 Agustus 2022 PDFAngger SatriaNo ratings yet
- Jadwal Operasi, Senin 8 Agustus 2022Document1 pageJadwal Operasi, Senin 8 Agustus 2022Angger SatriaNo ratings yet
- Jadwal Operasi, Senin 18 Juli 2022Document1 pageJadwal Operasi, Senin 18 Juli 2022Angger SatriaNo ratings yet
- Jadwal Operasi, Jum'at 22 Juli 2022Document1 pageJadwal Operasi, Jum'at 22 Juli 2022Angger SatriaNo ratings yet
- Jadwal Operasi, Kamis 28 Juli 2022Document1 pageJadwal Operasi, Kamis 28 Juli 2022Angger SatriaNo ratings yet
- Jadwal Operasi, Jum'at 29 Juli 2022Document1 pageJadwal Operasi, Jum'at 29 Juli 2022Angger SatriaNo ratings yet
- Jadwal Operasi, Senin 11 Juli 2022 PDFDocument1 pageJadwal Operasi, Senin 11 Juli 2022 PDFAngger SatriaNo ratings yet
- Jadwal Operasi, Kamis 4 Agustus 2022Document1 pageJadwal Operasi, Kamis 4 Agustus 2022Angger SatriaNo ratings yet
- Jadwal Operasi, Selasa 9 Agustus 2022Document1 pageJadwal Operasi, Selasa 9 Agustus 2022Angger SatriaNo ratings yet
- Jadwal Operasi, Jum'at 19 Agustus 2022 PDFDocument1 pageJadwal Operasi, Jum'at 19 Agustus 2022 PDFAngger SatriaNo ratings yet
- Jadwal Operasi, Kamis 21 Juli 2022Document1 pageJadwal Operasi, Kamis 21 Juli 2022Angger SatriaNo ratings yet
- Jadwal Operasi, Jum'at 5 Agustus 2022Document1 pageJadwal Operasi, Jum'at 5 Agustus 2022Angger SatriaNo ratings yet
- Ju 0000000000001548Document11 pagesJu 0000000000001548Angger SatriaNo ratings yet
- Jadwal Operasi, Selasa 19 Juli 2022Document1 pageJadwal Operasi, Selasa 19 Juli 2022Angger SatriaNo ratings yet
- Jadwal Operasi, Kamis 7 Juli 2022 PDFDocument1 pageJadwal Operasi, Kamis 7 Juli 2022 PDFAngger SatriaNo ratings yet
- Jadwal Operasi, Rabu 13 Juli 2022 PDFDocument1 pageJadwal Operasi, Rabu 13 Juli 2022 PDFAngger SatriaNo ratings yet
- Jadwal Operasi, Jumat 8 Juli 2022 PDFDocument1 pageJadwal Operasi, Jumat 8 Juli 2022 PDFAngger SatriaNo ratings yet
- Jadwal Operasi, Kamis 14 Juli 2022 PDFDocument1 pageJadwal Operasi, Kamis 14 Juli 2022 PDFAngger SatriaNo ratings yet
- Jadwal Operasi, Jum'at 15 Juli 2022 PDFDocument1 pageJadwal Operasi, Jum'at 15 Juli 2022 PDFAngger SatriaNo ratings yet
- Journal Pone 0253236Document10 pagesJournal Pone 0253236Angger SatriaNo ratings yet
- Checklist StudyDocument3 pagesChecklist StudyAngger SatriaNo ratings yet
- J Jpedsurg 2020 03 023Document4 pagesJ Jpedsurg 2020 03 023Angger SatriaNo ratings yet
- Median Rhomboid Glossitis in A Patient Undergoing Orthodontic TreatmentDocument4 pagesMedian Rhomboid Glossitis in A Patient Undergoing Orthodontic Treatmentandreia ichimNo ratings yet
- 0bf403db-e794-4967-b46c-737b3dc23d71Document7 pages0bf403db-e794-4967-b46c-737b3dc23d71utkarsh kushwahaNo ratings yet
- Jpn. J. Clin. Oncol.-2014-Xue-926-31 PDFDocument6 pagesJpn. J. Clin. Oncol.-2014-Xue-926-31 PDFKarina Mega WNo ratings yet
- Disorders of Esophagus and StomachDocument29 pagesDisorders of Esophagus and StomachSamuel kuriaNo ratings yet
- Surgery of The SkinDocument66 pagesSurgery of The SkinJess PeltraNo ratings yet
- Guideline AnesthesiaDocument31 pagesGuideline AnesthesiaMuhammad Izzatul Naim ZainuddinNo ratings yet
- Abdomen Pediatrics1Document12 pagesAbdomen Pediatrics1cmalloupas91No ratings yet
- Radiation TherapyDocument22 pagesRadiation TherapyErl D. Melitante100% (1)
- Venous Thromboembolism (VTE) - McMaster Pathophysiology ReviewDocument9 pagesVenous Thromboembolism (VTE) - McMaster Pathophysiology ReviewFadiyah UlfahNo ratings yet
- A Framework For Standardized Management of IntrapartumDocument11 pagesA Framework For Standardized Management of IntrapartumRaul A UrbinaNo ratings yet
- RIMS Thesis TopicsDocument3 pagesRIMS Thesis TopicsroshansanasamNo ratings yet
- 10 1056@NEJMoa1905380Document11 pages10 1056@NEJMoa1905380anisaNo ratings yet
- HemoptoeDocument42 pagesHemoptoeBhisma D. SyaputraNo ratings yet
- GTW ApaanDocument3 pagesGTW ApaanOshbbyNo ratings yet
- CBD - DR - Muh Saugi Abduh, SP - PD, KKV, FINASIM - LUPITA MAHARANI - HCCDocument77 pagesCBD - DR - Muh Saugi Abduh, SP - PD, KKV, FINASIM - LUPITA MAHARANI - HCCMustika RanyNo ratings yet
- 47 Case ReportDocument4 pages47 Case Reportsusanti bulanNo ratings yet
- William Osler El Hombre y Sus DescripcionesDocument10 pagesWilliam Osler El Hombre y Sus Descripcionescristian vallejoNo ratings yet
- ILAE Classification of Epilepsy - Update: Chris Rittey SheffieldDocument34 pagesILAE Classification of Epilepsy - Update: Chris Rittey Sheffieldzefri suhendarNo ratings yet
- Abdominal PainDocument38 pagesAbdominal PainPro fatherNo ratings yet
- Histological and Gene Expression Analysis of The Effects of Menopause Status and Hormone Therapy On The Vaginal Introitus and Labia MajoraDocument34 pagesHistological and Gene Expression Analysis of The Effects of Menopause Status and Hormone Therapy On The Vaginal Introitus and Labia MajoraDomenico FeleppaNo ratings yet
- Krishnan2019 Article NeuroimagingInPediatricHydroceDocument9 pagesKrishnan2019 Article NeuroimagingInPediatricHydroceBrenoNo ratings yet
- Zinc, Copper and Selenium in ReproductionDocument15 pagesZinc, Copper and Selenium in ReproductionNéstor MirelesNo ratings yet
- Training Strategy For ASHA Facilitators and ANMDocument3 pagesTraining Strategy For ASHA Facilitators and ANMakashniranjaneNo ratings yet
- Ultrasound Diagnostics of Thyroid DiseasesDocument245 pagesUltrasound Diagnostics of Thyroid Diseasesivan.danovNo ratings yet