You might also like
- PADIS Guidelines Teaching Slides DeliriumDocument30 pagesPADIS Guidelines Teaching Slides DeliriumMohamat MutajirNo ratings yet
- PADIS Guidelines Teaching Slides PainDocument43 pagesPADIS Guidelines Teaching Slides Pain陳政吉No ratings yet
- PADIS Guidelines Teaching Slides SedationDocument27 pagesPADIS Guidelines Teaching Slides SedationMohamat MutajirNo ratings yet
- PADIS Guidelines Teaching Slides ImmobilityDocument25 pagesPADIS Guidelines Teaching Slides ImmobilityDaniel Lago BorgesNo ratings yet
- OS-1a GRADE Intro - Detty Revised - 20160519Document31 pagesOS-1a GRADE Intro - Detty Revised - 20160519Febbty KuswantiNo ratings yet
- GRADE Practice GuidelinesDocument49 pagesGRADE Practice GuidelinesSuli M ENo ratings yet
- Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) by DR Linda Long (Pen-TAG)Document21 pagesGrading of Recommendations, Assessment, Development, and Evaluations (GRADE) by DR Linda Long (Pen-TAG)AkshayNo ratings yet
- How To Read A Paper - Critical AppraisalDocument48 pagesHow To Read A Paper - Critical AppraisalMark KerrNo ratings yet
- TherappraisalclrDocument5 pagesTherappraisalclrMike CabotageNo ratings yet
- 14.00-14.30 Systematic Review 2023 - อ.ภัทรวัณย์ วรธนารัตน์Document58 pages14.00-14.30 Systematic Review 2023 - อ.ภัทรวัณย์ วรธนารัตน์reservemos1No ratings yet
- Ebm Topic DiscussionDocument3 pagesEbm Topic Discussionapi-457374333No ratings yet
- DGNR S3 Guideline English TranslationDocument5 pagesDGNR S3 Guideline English Translationv.bokatueva71No ratings yet
- AEPCC Revista04 EN-CONDYLOMADocument40 pagesAEPCC Revista04 EN-CONDYLOMAneneNo ratings yet
- Cohort StudiesDocument30 pagesCohort StudiesAbinandhan AbiNo ratings yet
- Interpreting Diagnostic Tests: Ian Mcdowell Department of Epidemiology & Community Medicine January 2010Document30 pagesInterpreting Diagnostic Tests: Ian Mcdowell Department of Epidemiology & Community Medicine January 2010AntenehNo ratings yet
- Risk Assessment & ManagementDocument51 pagesRisk Assessment & ManagementBelkacem AchourNo ratings yet
- DiabeticRetinopathy 2015PPPDocument4 pagesDiabeticRetinopathy 2015PPPCaleb Llacctarimay SanchezNo ratings yet
- 2022 Guideline For The Management of Patients With Spontaneous ICH Clinical Update SlidesDocument38 pages2022 Guideline For The Management of Patients With Spontaneous ICH Clinical Update SlidesshaishaiNo ratings yet
- Root Cause AnalysisDocument42 pagesRoot Cause AnalysisAzhar Saleem100% (1)
- OutlineDocument20 pagesOutlineDrx ahmed MaherNo ratings yet
- All About Clinical TrialsDocument29 pagesAll About Clinical TrialsJay BingoNo ratings yet
- Modulo III InvestigacionDocument59 pagesModulo III InvestigacionLorena TorresNo ratings yet
- What Is Basic Difference Between HAZOP and HAZIDDocument34 pagesWhat Is Basic Difference Between HAZOP and HAZIDNirnay Patil100% (4)
- NCE Assessment and Testing PDFDocument7 pagesNCE Assessment and Testing PDFAmy D.100% (1)
- Worksheets For Preparing A Summary of Findings Using GradeDocument17 pagesWorksheets For Preparing A Summary of Findings Using Gradeyassin gaming g.No ratings yet
- Cornea/External Disease Summary Benchmarks For Preferred Practice Pattern® GuidelinesDocument12 pagesCornea/External Disease Summary Benchmarks For Preferred Practice Pattern® GuidelinesfifahcantikNo ratings yet
- Quality Assessment, Data Synthesis, - Presenting The Results - CRPDocument39 pagesQuality Assessment, Data Synthesis, - Presenting The Results - CRPMuhammad Zukri MalikNo ratings yet
- Evidence-Based Case Report: Kartiwa Hadi NuryantoDocument20 pagesEvidence-Based Case Report: Kartiwa Hadi NuryantohfathiardiNo ratings yet
- Primary Open-Angle Glaucoma SummaryDocument9 pagesPrimary Open-Angle Glaucoma SummaryTony AndersonNo ratings yet
- LSPfor Risk AssessmentDocument7 pagesLSPfor Risk AssessmentadhavanannathuraiNo ratings yet
- Understanding Phase 2B Clinical TrialsDocument24 pagesUnderstanding Phase 2B Clinical Trialssabuz pataNo ratings yet
- How To Appraise Harm JournalDocument26 pagesHow To Appraise Harm Journalmirfanjee89No ratings yet
- Diagnostic Test DesignDocument30 pagesDiagnostic Test DesignDika Gita PratamaNo ratings yet
- Bab 2 Persepsi Tentang Risiko PDFDocument53 pagesBab 2 Persepsi Tentang Risiko PDFDaffa JNo ratings yet
- Guideline For Assessment of Cardiovascular Risk in Asymptomatic AdultsDocument31 pagesGuideline For Assessment of Cardiovascular Risk in Asymptomatic AdultsAlexa Lorenzo CiprianoNo ratings yet
- RCT Report - ChuaDocument36 pagesRCT Report - Chuanv5yy5ryd5No ratings yet
- Risk: Definition: Effect of Uncertainties On Objectives (ISO 31000:2018)Document40 pagesRisk: Definition: Effect of Uncertainties On Objectives (ISO 31000:2018)sskiitbNo ratings yet
- Section 7 Slides 2022Document70 pagesSection 7 Slides 2022Sathappan KasiNo ratings yet
- Risk Assessments: School of PhysicsDocument51 pagesRisk Assessments: School of Physicsvava nillaaaNo ratings yet
- Risk Assessments: School of PhysicsDocument51 pagesRisk Assessments: School of PhysicsUmmama KhanNo ratings yet
- Evidence-Based Medicine and Critical AppraisalDocument49 pagesEvidence-Based Medicine and Critical AppraisalRamón Rosal SequeaNo ratings yet
- Risk Management For Human ErrorDocument81 pagesRisk Management For Human Errorbasit.000No ratings yet
- Analytical Validation and Points For Discussion: Julia Tait Lathrop, PHDDocument46 pagesAnalytical Validation and Points For Discussion: Julia Tait Lathrop, PHDAlicia GarcíaNo ratings yet
- 6.4 Accident Investigation 6 Edit BDocument100 pages6.4 Accident Investigation 6 Edit BHilmyZulkifliNo ratings yet
- Pemilihan Disain Studi ObservasionalDocument44 pagesPemilihan Disain Studi Observasionalsum4nd4nNo ratings yet
- EBM, Design Study, Quantifying RiskDocument71 pagesEBM, Design Study, Quantifying Riskseptian kristyanaNo ratings yet
- Critical Appraisal of A JournalDocument29 pagesCritical Appraisal of A Journalmonique marwick100% (2)
- BC-2208 PPPSummaryBenchmarks.17.CataractDocument4 pagesBC-2208 PPPSummaryBenchmarks.17.CataractKittithep SukkhongNo ratings yet
- Arun Bhatt Consultant Clinical Research and Development PDFDocument38 pagesArun Bhatt Consultant Clinical Research and Development PDFAnant KhotNo ratings yet
- Systematic Review and Meta-Analysis Topic DiscussionDocument3 pagesSystematic Review and Meta-Analysis Topic Discussionapi-589696674No ratings yet
- EBCR Refreshing For ResidentsDocument47 pagesEBCR Refreshing For ResidentsJohn Patria Maruli SinagaNo ratings yet
- Lecture 3 - Practical Guide - Overview EBM - Dr. Jarir at Thobari, PhD.,D.Pharm (2020)Document13 pagesLecture 3 - Practical Guide - Overview EBM - Dr. Jarir at Thobari, PhD.,D.Pharm (2020)Lily LiestiowatiNo ratings yet
- Hazard Identification & Risk Assessment (HIRA)Document25 pagesHazard Identification & Risk Assessment (HIRA)Suraj PantNo ratings yet
- 1121054Document186 pages1121054optisearchNo ratings yet
- How To Appraise Harm: Nia Kurniati Child Health Department/CE-EBM Faculty of Medicine Universitas of IndonesiaDocument46 pagesHow To Appraise Harm: Nia Kurniati Child Health Department/CE-EBM Faculty of Medicine Universitas of IndonesiageraldinekenyoNo ratings yet
- Risk Assesment in Microbiology: Presented by K. Santosh KumarDocument23 pagesRisk Assesment in Microbiology: Presented by K. Santosh KumarsanthoshkurvaNo ratings yet
- BC-2208 PPPSummaryBenchmarks.17.PediatricDocument5 pagesBC-2208 PPPSummaryBenchmarks.17.PediatricKittithep SukkhongNo ratings yet
- 06 Overview of Ra1Document71 pages06 Overview of Ra1adryankusNo ratings yet
- Clinical Practice Guidelines - 2017 PDFDocument820 pagesClinical Practice Guidelines - 2017 PDFvijay kumarNo ratings yet
- This Study Resource Was: Case: The Medicines CompanyDocument4 pagesThis Study Resource Was: Case: The Medicines CompanyFelipe AcuñaNo ratings yet
- Chand-Essential Interventional Radiology - 2022 Opt SigfridoDocument929 pagesChand-Essential Interventional Radiology - 2022 Opt SigfridoOscar SalasNo ratings yet
- Critical Care Medication Infusion ChartDocument2 pagesCritical Care Medication Infusion ChartEgi Munandar100% (1)
- Myocardial Infarction Medication: Aspirin (Ascriptin, Bayer Aspirin, Aspirtab, Ecotrin, Durlaza)Document11 pagesMyocardial Infarction Medication: Aspirin (Ascriptin, Bayer Aspirin, Aspirtab, Ecotrin, Durlaza)Ashutosh SinghNo ratings yet
- ACS Management and ESC GuidelinesDocument56 pagesACS Management and ESC GuidelinesAnonymous NeRC5JYiSNo ratings yet
- ACS Management in JKN EraDocument36 pagesACS Management in JKN EraErwin Freddy HutabaratNo ratings yet
- CCD 25132Document3 pagesCCD 25132bharattaneja017023No ratings yet
- Direct Oral Anticoagulants and Parenteral Direct Thrombin Inhibitors - Dosing and Adverse Effects - UpToDateDocument60 pagesDirect Oral Anticoagulants and Parenteral Direct Thrombin Inhibitors - Dosing and Adverse Effects - UpToDateVERONICA BARRERANo ratings yet
- Acute Coronary Syndrome - 2022Document91 pagesAcute Coronary Syndrome - 2022Rana Khaled AwwadNo ratings yet
- ICU IV Infusion GuidelinesDocument2 pagesICU IV Infusion Guidelinessgod34No ratings yet
- Anticoagulation PharmacologyDocument36 pagesAnticoagulation PharmacologyaymenNo ratings yet
- Acute Coronary SyndromesDocument8 pagesAcute Coronary Syndromesadek07No ratings yet
- Braunwald - UA and NSTEMIDocument49 pagesBraunwald - UA and NSTEMIusfcards100% (2)
- Bcps - AcsDocument63 pagesBcps - Acsapi-506607906No ratings yet
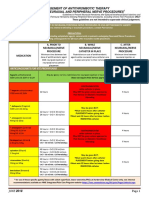
- Management of Antithrombotic Therapy For Neuraxial and Peripheral Nerve ProceduresDocument3 pagesManagement of Antithrombotic Therapy For Neuraxial and Peripheral Nerve Proceduresjojobod100% (1)
- General Indications: AnticoagulantsDocument15 pagesGeneral Indications: AnticoagulantswahidNo ratings yet
- HKPJ Vol252 - 40pp - Lo-ResDocument40 pagesHKPJ Vol252 - 40pp - Lo-ReswslNo ratings yet
- Deep Vein Thrombosis in Pediatric PatientsDocument9 pagesDeep Vein Thrombosis in Pediatric Patientsemilce beltran100% (1)
- Heparin Induced Thrombocytopenia: By: Hadeel Abueid, Medical Student, Alquds University 3 March 2021Document36 pagesHeparin Induced Thrombocytopenia: By: Hadeel Abueid, Medical Student, Alquds University 3 March 2021Hadeel Abu EidNo ratings yet
- Post PCI CareDocument17 pagesPost PCI CareaefawfAWNo ratings yet
- Anticoagulation Options For Intermittent HDDocument10 pagesAnticoagulation Options For Intermittent HDNarinder SharmaNo ratings yet
- Bleeding in ACS SlideCASTDocument83 pagesBleeding in ACS SlideCASTCarlos Del Carpio EnriquezNo ratings yet
- Overview of HemostasisDocument21 pagesOverview of Hemostasis黄資元100% (1)
- NSTMIDocument16 pagesNSTMIrio kharismaNo ratings yet
- Heparin Induced Thrombocytopenia 2009Document49 pagesHeparin Induced Thrombocytopenia 2009pannumdNo ratings yet
- Stop Anticoagulation Neuraxial AnesthesiaDocument3 pagesStop Anticoagulation Neuraxial AnesthesiaGihan NakhlehNo ratings yet
- Anticoagulants 161120143945Document29 pagesAnticoagulants 161120143945Roshan SahuNo ratings yet
- Medication Instructions Prior To SurgeryDocument11 pagesMedication Instructions Prior To Surgeryhohj100% (1)
- The Medicines Company Presentation Final OriginalDocument24 pagesThe Medicines Company Presentation Final OriginalVishwajeet KarmwarNo ratings yet