You might also like
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationFrom EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehNo ratings yet
- Neuro-Ophthalmological Biomarkers of Visual Outcome in Newly Diagnosed Idiopathic Intracranial HypertensionDocument8 pagesNeuro-Ophthalmological Biomarkers of Visual Outcome in Newly Diagnosed Idiopathic Intracranial HypertensionMira TamilaNo ratings yet
- Diagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaFrom EverandDiagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaNo ratings yet
- Blood Pressure and GlaucomaDocument6 pagesBlood Pressure and GlaucomaRizqy AbdullahNo ratings yet
- Robba Et Al-2024-Intensive Care MedicineDocument13 pagesRobba Et Al-2024-Intensive Care MedicineLeiniker NavarroNo ratings yet
- EJCO - Volume 6 - Issue 2 - Pages 117-123Document7 pagesEJCO - Volume 6 - Issue 2 - Pages 117-123doaa ahmadNo ratings yet
- Correlation of Visual Field Defects and Optical Coherence Tomography Finding in Migraine PatientsDocument5 pagesCorrelation of Visual Field Defects and Optical Coherence Tomography Finding in Migraine Patientsmara 11No ratings yet
- Prevalence of Glaucoma in North Costal Andhra PradeshDocument7 pagesPrevalence of Glaucoma in North Costal Andhra PradeshIJAR JOURNALNo ratings yet
- Clinical Study of Intraocular Pressure Changesfollowing Nd-Yag Laser Iridotomy in Angle Closure DiseaseDocument15 pagesClinical Study of Intraocular Pressure Changesfollowing Nd-Yag Laser Iridotomy in Angle Closure DiseaseIJAR JOURNALNo ratings yet
- Diagnosis of Idiopathic Normal Pressure Hydrocephalus Is Supported by MRI-based Scheme: A Prospective Cohort StudyDocument11 pagesDiagnosis of Idiopathic Normal Pressure Hydrocephalus Is Supported by MRI-based Scheme: A Prospective Cohort StudyDini NanamiNo ratings yet
- Parinaud Syndrome: Any Clinicoradiological Correlation?: L. Pollak - T. Zehavi-Dorin - A. Eyal - R. Milo - R. Huna-BaronDocument6 pagesParinaud Syndrome: Any Clinicoradiological Correlation?: L. Pollak - T. Zehavi-Dorin - A. Eyal - R. Milo - R. Huna-BaronJessica HerreraNo ratings yet
- Full Paper. Clinical Profile of Cyclocryotherapy Patients in Yap Eye HospitalDocument4 pagesFull Paper. Clinical Profile of Cyclocryotherapy Patients in Yap Eye HospitalSeravina Adila IzzatiNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleMarcella PolittonNo ratings yet
- Normal Tension Glaucoma: A Different Disease?: Kuldev SinghDocument3 pagesNormal Tension Glaucoma: A Different Disease?: Kuldev SinghRasha Mounir Abdel-Kader El-TanamlyNo ratings yet
- Endothelial Progenitor Cells: A New Key For Endothelial Dysfunction in MigraineDocument6 pagesEndothelial Progenitor Cells: A New Key For Endothelial Dysfunction in MigrainevividewaNo ratings yet
- Diagnosis, Management, and Outcomes of Patients With Syncope and Bundle Branch BlockDocument7 pagesDiagnosis, Management, and Outcomes of Patients With Syncope and Bundle Branch BlockPaul CalbureanNo ratings yet
- Evaluation of The Relationship Between Binocular Anomaly and Headache Prospective Cross Sectional StudyDocument7 pagesEvaluation of The Relationship Between Binocular Anomaly and Headache Prospective Cross Sectional StudyEstefania GuerreroNo ratings yet
- Convulsive Status Epilepticus Management in Adults and Children: of The Working Group of The Polish Society of EpileptologyDocument8 pagesConvulsive Status Epilepticus Management in Adults and Children: of The Working Group of The Polish Society of Epileptologymoy9616No ratings yet
- Chronic Glaucoma Treatment / SEEOS / Tirane / 18-06-2010 / Prof - Dr.ilhami Goranci, DR - Ardiana Goranci, DR - Dafina Goranci, DR - Halil Ajvazi, DR - Dardan Goranci.Document33 pagesChronic Glaucoma Treatment / SEEOS / Tirane / 18-06-2010 / Prof - Dr.ilhami Goranci, DR - Ardiana Goranci, DR - Dafina Goranci, DR - Halil Ajvazi, DR - Dardan Goranci.Dardan GoranciNo ratings yet
- Fneur 08 00507Document8 pagesFneur 08 00507bozasnachoNo ratings yet
- Sleep and Psychiatric Abnormalities in Gullian Barré SyndromeDocument7 pagesSleep and Psychiatric Abnormalities in Gullian Barré SyndromeShri RamNo ratings yet
- Glaukoma Case ReportDocument9 pagesGlaukoma Case ReportHIstoryNo ratings yet
- ETM 2021-03-Association of Obstructive Sleep Apnea-Hypopnea Syndrome With Glaucomatous Optic Neuropathy and Ocular Blood FlowDocument7 pagesETM 2021-03-Association of Obstructive Sleep Apnea-Hypopnea Syndrome With Glaucomatous Optic Neuropathy and Ocular Blood FlowMarcos FerrazNo ratings yet
- Imp Landmark Glauc StudiesDocument100 pagesImp Landmark Glauc StudiesASHOK KUMAR SINGHNo ratings yet
- Brainhypoxiaisassociatedwithshort Termoutcomeafterseveretraumaticbraininjuryindependentlyofi 2Document9 pagesBrainhypoxiaisassociatedwithshort Termoutcomeafterseveretraumaticbraininjuryindependentlyofi 2indahNo ratings yet
- Seizure: Kristina Malmgren, Anna EdelvikDocument8 pagesSeizure: Kristina Malmgren, Anna EdelvikRidho ArendoNo ratings yet
- Content ServerDocument8 pagesContent ServerG. Araya MoraNo ratings yet
- Critical Care Medicine: Background: Methods: ResultsDocument9 pagesCritical Care Medicine: Background: Methods: ResultsMedicina InternaNo ratings yet
- BR J Ophthalmol-2014-Chan-79-81 PDFDocument4 pagesBR J Ophthalmol-2014-Chan-79-81 PDFRomi Mauliza FauziNo ratings yet
- Syncope and Epilepsy Coexist in Possible' and Drug-Resistant' Epilepsy (Overlap Between Epilepsy and Syncope Study - Oesys)Document9 pagesSyncope and Epilepsy Coexist in Possible' and Drug-Resistant' Epilepsy (Overlap Between Epilepsy and Syncope Study - Oesys)Monica Aleja FernándezNo ratings yet
- Emanuel 2017Document4 pagesEmanuel 2017Kimberly Ann SumbillaNo ratings yet
- Long Term Outcomes of Status Epilepticus: A Critical AssessmentDocument15 pagesLong Term Outcomes of Status Epilepticus: A Critical AssessmentnafamaulidinaNo ratings yet
- Efikasi TX Gukoma 2016Document37 pagesEfikasi TX Gukoma 2016Al-Harits OctaNo ratings yet
- 617 08 16 ArticleDocument8 pages617 08 16 Articlewilliam lozaNo ratings yet
- Casos Clinicos NEJM 2018Document287 pagesCasos Clinicos NEJM 2018Eduarda RosasNo ratings yet
- Hypoglycemic Encephalopathy A Case Series and Literature Review On Outcome DeterminationDocument7 pagesHypoglycemic Encephalopathy A Case Series and Literature Review On Outcome Determinationc5qdk8jnNo ratings yet
- Prevalence of Depression and Anxiety Among ParticiDocument10 pagesPrevalence of Depression and Anxiety Among ParticiAishah FarihaNo ratings yet
- Epilepsy, Headache, and Abdominal Pain After Shunt Surgery For Idiopathic Normal Pressure Hydrocephalus - The INPH-CRasH StudyDocument10 pagesEpilepsy, Headache, and Abdominal Pain After Shunt Surgery For Idiopathic Normal Pressure Hydrocephalus - The INPH-CRasH StudyFernandoNo ratings yet
- Kabat Rehabilitation For Facial Nerve Paralysis: Perspective On Neurokinetic Recovery and Review of Clinical Evaluation ToolsDocument9 pagesKabat Rehabilitation For Facial Nerve Paralysis: Perspective On Neurokinetic Recovery and Review of Clinical Evaluation ToolsInternational Journal of Academic Scientific ResearchNo ratings yet
- Highlights in Neuro OphthalmologyDocument2 pagesHighlights in Neuro OphthalmologyShruthi VMNo ratings yet
- Ventriculo-Peritoneal Shunting Is A Safe and Effective Treatment For Idiopathic Intracranial HypertensionDocument10 pagesVentriculo-Peritoneal Shunting Is A Safe and Effective Treatment For Idiopathic Intracranial HypertensionTELHNo ratings yet
- JAMDIG StudyDocument9 pagesJAMDIG StudyTushar BatraNo ratings yet
- GLAUKOMA2Document12 pagesGLAUKOMA2NorytaWahyuniawatiAsfianaNo ratings yet
- BormannDocument9 pagesBormannMereeshaNo ratings yet
- Extubation Success Prediction in A Multicentric Cohort of Patients With Severe Brain InjuryDocument9 pagesExtubation Success Prediction in A Multicentric Cohort of Patients With Severe Brain InjuryEdison LucioNo ratings yet
- SINPHONIDocument11 pagesSINPHONIvistamaniacNo ratings yet
- Risk Factors For Primary Open Angle Glaucoma in Japanese Sub 101911Document7 pagesRisk Factors For Primary Open Angle Glaucoma in Japanese Sub 101911marwicuteNo ratings yet
- Presuregry EvaluationDocument8 pagesPresuregry Evaluationbhadresh neuro mangukiyaNo ratings yet
- The Glymphatic System and New Etiopathogenic Hypotheses Concerning Glaucoma Based On Pilot Study On Glaucoma Patients Who Underwent Osteopathic Manipulative Treatment (OMT)Document7 pagesThe Glymphatic System and New Etiopathogenic Hypotheses Concerning Glaucoma Based On Pilot Study On Glaucoma Patients Who Underwent Osteopathic Manipulative Treatment (OMT)BOHR International Journal of Current Research in Optometry and Ophthalmology (BIJCROO)No ratings yet
- Obling Et Al-2023-Intensive Care MedicineDocument12 pagesObling Et Al-2023-Intensive Care Medicinefatmaahmed3241No ratings yet
- Aos0091 0406Document7 pagesAos0091 0406maandre123No ratings yet
- Statin and GalucomaDocument6 pagesStatin and Galucomawimakrifah istiqomahNo ratings yet
- Chest 147 1 132Document8 pagesChest 147 1 132Timothy Eduard A. SupitNo ratings yet
- Axial Myopia Is Associated With Visual Field Prognosis of Primary Open-Angle GlaucomaDocument10 pagesAxial Myopia Is Associated With Visual Field Prognosis of Primary Open-Angle GlaucomaRezha IndrawanNo ratings yet
- Uzma FasihDocument7 pagesUzma FasihFriskadoreendaputriNo ratings yet
- What We Have Learned From The Ocular Hypertension TreatmentDocument8 pagesWhat We Have Learned From The Ocular Hypertension TreatmentASHOK KUMAR SINGHNo ratings yet
- Glaucoma Case ReportDocument9 pagesGlaucoma Case Reportsuci caraswatiNo ratings yet
- IcuDocument56 pagesIcurulli_pranandaNo ratings yet
- The Relationship Between Neurogenic Dysphagia, Stroke-Associated Pneumonia and Functional Outcome in A Cohort of Ischemic Stroke Patients Treated With Mechanical ThrombectomyDocument8 pagesThe Relationship Between Neurogenic Dysphagia, Stroke-Associated Pneumonia and Functional Outcome in A Cohort of Ischemic Stroke Patients Treated With Mechanical Thrombectomypalmaputri pinantiNo ratings yet
- Update On Idiopathic Intracranial Hypertension: Sivashakthi Kanagalingam, MD Prem S. Subramanian, MD, PHDDocument13 pagesUpdate On Idiopathic Intracranial Hypertension: Sivashakthi Kanagalingam, MD Prem S. Subramanian, MD, PHDMomeneo NeoNo ratings yet
- Rosenberg 1979Document6 pagesRosenberg 1979Aliénor VienneNo ratings yet
- Roh 1998Document8 pagesRoh 1998Aliénor VienneNo ratings yet
- Ahn 2013Document2 pagesAhn 2013Aliénor VienneNo ratings yet
- Ahn 2016Document7 pagesAhn 2016Aliénor VienneNo ratings yet
- Young 2014Document8 pagesYoung 2014Aliénor VienneNo ratings yet
- SAIC N 2023 PreQualTestApplicator&AppProcCastRefract EL Rev2Document3 pagesSAIC N 2023 PreQualTestApplicator&AppProcCastRefract EL Rev2Anonymous S9qBDVkyNo ratings yet
- S.No. Components Makes: 1 Grab Cranes - Gantry TypeDocument4 pagesS.No. Components Makes: 1 Grab Cranes - Gantry TypeHarish KumarNo ratings yet
- ATF - List of Explosive MaterialsDocument8 pagesATF - List of Explosive MaterialsxiaotaoscribdNo ratings yet
- Ao+ WDM12 R40DDocument8 pagesAo+ WDM12 R40DPedro Igor Oliveira CarvalhoNo ratings yet
- Specifications: Louie Jean Mabanag Ar - 3BDocument8 pagesSpecifications: Louie Jean Mabanag Ar - 3BLouie Jean100% (1)
- Traina 250Wp PDFDocument2 pagesTraina 250Wp PDFSherifImamNo ratings yet
- Renault Gearbox and Final Drive OilsDocument10 pagesRenault Gearbox and Final Drive OilsPhat0% (1)
- Turnitin Originality ReportDocument20 pagesTurnitin Originality ReportNaomi Deirdre ReyesNo ratings yet
- Commissioning Valve Product BrochureDocument14 pagesCommissioning Valve Product BrochureblindjaxxNo ratings yet
- DuranDuran OrdinaryWorldDocument1 pageDuranDuran OrdinaryWorldEduardo LuzNo ratings yet
- JNTU Old Question Papers 2007Document8 pagesJNTU Old Question Papers 2007Srinivasa Rao GNo ratings yet
- Comic Book Paramhansa YoganandaDocument36 pagesComic Book Paramhansa Yoganandaarjuna198986% (7)
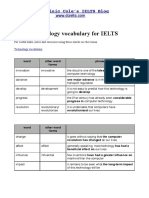
- Technology VocabularyDocument3 pagesTechnology VocabularyChixo GalaxyNo ratings yet
- Product Analysis Certificate: Propanol-2 (Iso-Propanol) A.RDocument1 pageProduct Analysis Certificate: Propanol-2 (Iso-Propanol) A.RAMMARNo ratings yet
- Doxiadis, Constantinos (1968) EkisticsDocument556 pagesDoxiadis, Constantinos (1968) EkisticsCelje1234No ratings yet
- Auto Repair and Car Wash Business PlanDocument31 pagesAuto Repair and Car Wash Business PlanKiraYagamiNo ratings yet
- Spining Mill in IndiaDocument74 pagesSpining Mill in IndiaMahendra Shah100% (4)
- Shravana CharacterDocument5 pagesShravana CharacterSuresh SharmaNo ratings yet
- Tadabbur I Qur'ānDocument43 pagesTadabbur I Qur'ānamjad_emailNo ratings yet
- 2020 Sustainabilty Report - ENDocument29 pages2020 Sustainabilty Report - ENGeraldNo ratings yet
- The Determinants of Service Quality and Customer Satisfaction in Malaysian e Hailing ServicesDocument8 pagesThe Determinants of Service Quality and Customer Satisfaction in Malaysian e Hailing ServicesYoannisa AtinaNo ratings yet
- 2nd Round Selected StudentsDocument1 page2nd Round Selected StudentsSiri KRNo ratings yet
- Jurnal Praktikum Dasar-Dasar Pemisahan Kimia Pembuatan Membran Polysulfon (PSF)Document9 pagesJurnal Praktikum Dasar-Dasar Pemisahan Kimia Pembuatan Membran Polysulfon (PSF)Rizki AuNo ratings yet
- Estimating Crack Widths in Steel Fibre-Reinforced ConcreteDocument12 pagesEstimating Crack Widths in Steel Fibre-Reinforced ConcreteRm1262No ratings yet
- Inhalation AnestheticsDocument27 pagesInhalation AnestheticsMarcelitaTaliaDuwiriNo ratings yet
- Electric Circuits 1 MSDocument4 pagesElectric Circuits 1 MSEvaNo ratings yet
- Boiler Sizing Guide PDFDocument1 pageBoiler Sizing Guide PDFfmkhan21100% (1)
- Gunny PasteDocument2 pagesGunny PastejpesNo ratings yet
- EN 301.908-2 Ver 3.2.1Document37 pagesEN 301.908-2 Ver 3.2.1DHDIDIDNo ratings yet
- Functional Endoscopic Sinus SurgeryDocument3 pagesFunctional Endoscopic Sinus SurgeryDanielicah CruzNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (28)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (2)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No ratings yet
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (58)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- Troubled: A Memoir of Foster Care, Family, and Social ClassFrom EverandTroubled: A Memoir of Foster Care, Family, and Social ClassRating: 4.5 out of 5 stars4.5/5 (27)