0% found this document useful (0 votes)
500 views1 pageAdult Fall Risk Assessment Tool
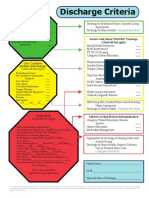
This document contains an adult fall risk assessment and prevention plan. It includes a 10 item modified Morse Fall Scale to assess risk level as low, medium, or high. It outlines interventions for each risk level, with low risk getting observation, medium risk adding toileting assistance and ensuring comfort, and high risk triggering physical/occupational therapy consultation and medication review. Spaces are provided to document fall risk reassessment if the patient's condition changes.
Uploaded by
anumolCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
500 views1 pageAdult Fall Risk Assessment Tool
This document contains an adult fall risk assessment and prevention plan. It includes a 10 item modified Morse Fall Scale to assess risk level as low, medium, or high. It outlines interventions for each risk level, with low risk getting observation, medium risk adding toileting assistance and ensuring comfort, and high risk triggering physical/occupational therapy consultation and medication review. Spaces are provided to document fall risk reassessment if the patient's condition changes.
Uploaded by
anumolCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd