You might also like
- Metformin A Review of Its Use in The Treatment Typ-DikonversiDocument30 pagesMetformin A Review of Its Use in The Treatment Typ-DikonversiAida H.djamhuriNo ratings yet
- Metabolism: Metformin-Associated Lactic Acidosis: Current Perspectives On Causes and RiskDocument10 pagesMetabolism: Metformin-Associated Lactic Acidosis: Current Perspectives On Causes and RisksureshNo ratings yet
- JRMS 19 658Document7 pagesJRMS 19 658fuckyeahonewNo ratings yet
- Metforminuseinchildren Andadolescentswith PrediabetesDocument13 pagesMetforminuseinchildren Andadolescentswith PrediabetesWarun KumarNo ratings yet
- Metformin HCLDocument3 pagesMetformin HCLAusaf AhmadNo ratings yet
- Glycemia and Kidney RDocument27 pagesGlycemia and Kidney RMARIA VICTORIA VELARDE ALIAGANo ratings yet
- Metformin Cancer ReviewDocument28 pagesMetformin Cancer ReviewWalida FadillahNo ratings yet
- Metformin 1 METFORMIN (500mg, 850mg and 1000mg Tablets) : New Zealand Data SheetDocument11 pagesMetformin 1 METFORMIN (500mg, 850mg and 1000mg Tablets) : New Zealand Data SheetAfifa ZainNo ratings yet
- The Lack of Effectiveness of Metformin Monotherapy As A First Line Medication in Patients With Type 2 Diabetes - ReviewedDocument10 pagesThe Lack of Effectiveness of Metformin Monotherapy As A First Line Medication in Patients With Type 2 Diabetes - ReviewedDiana PerezNo ratings yet
- MetFormin Generic Health TabDocument9 pagesMetFormin Generic Health TabNur Ekayani SyamNo ratings yet
- Comparative Pharmacokinetic Study Between Metformin Alone and Combined With Orlistat in Healthy Mexican VolunteersDocument7 pagesComparative Pharmacokinetic Study Between Metformin Alone and Combined With Orlistat in Healthy Mexican Volunteersintan kusumaningtyasNo ratings yet
- PDF - A Review of Efficacy and Safety of Oral Anti-Diabetic AgentsDocument41 pagesPDF - A Review of Efficacy and Safety of Oral Anti-Diabetic AgentsSahulNo ratings yet
- Metformin: An UpdateDocument9 pagesMetformin: An UpdateRahman MominNo ratings yet
- Metformin For DiabetesDocument9 pagesMetformin For Diabetesubaid khan afridiNo ratings yet
- Saxagliptin and Metformin in Fixed Combination For The Treatment of Type 2 Diabetes in AdultsDocument11 pagesSaxagliptin and Metformin in Fixed Combination For The Treatment of Type 2 Diabetes in AdultsLaura MelatiNo ratings yet
- DM Oral TX McnaDocument20 pagesDM Oral TX Mcnaapi-244842525No ratings yet
- Meds DiabetesDocument5 pagesMeds DiabetesAnjangsari 'aRie' WijayantiNo ratings yet
- The Side Effects of Metformin A ReviewDocument7 pagesThe Side Effects of Metformin A ReviewAlberto LiaoNo ratings yet
- Famasi IIDocument6 pagesFamasi IIMerlyn AngelicaNo ratings yet
- SGLT2 VS MetforminaDocument6 pagesSGLT2 VS MetforminaNOTAS GINECONo ratings yet
- Metformin, Diabetes, Review2Document5 pagesMetformin, Diabetes, Review2Ronal PerinoNo ratings yet
- Diabetologia: UK Prospective Diabetes Study (UKPDS)Document14 pagesDiabetologia: UK Prospective Diabetes Study (UKPDS)GuadalupeNo ratings yet
- METFORMIN FOR DIABETESDocument13 pagesMETFORMIN FOR DIABETESAllan DiazNo ratings yet
- Metformin - More Than Gold Standard' in The Treatment of Type 2 Diabetes MellitusDocument10 pagesMetformin - More Than Gold Standard' in The Treatment of Type 2 Diabetes MellitusArga Krittas MaranNo ratings yet
- Artículo Inglés 1deptal 2021 1 BDocument15 pagesArtículo Inglés 1deptal 2021 1 BRicardo CeballosNo ratings yet
- Unismuh Kuliah Sistem EndokrinDocument104 pagesUnismuh Kuliah Sistem EndokrinilhamaminsyaputraNo ratings yet
- Management of Persistent Hyperglycemia in Type 2 Diabetes MellitusDocument47 pagesManagement of Persistent Hyperglycemia in Type 2 Diabetes MellitusEslam khedrNo ratings yet
- Patient CharacteristicsDocument7 pagesPatient CharacteristicsHazem AlmasryNo ratings yet
- Diabetes MedicationDocument17 pagesDiabetes MedicationTaj lamajedNo ratings yet
- Diabetes Care 2015Document8 pagesDiabetes Care 2015Bego ZubietaNo ratings yet
- FR_H_6788_001_FinalSPCDocument28 pagesFR_H_6788_001_FinalSPCabenezer g/kirstosNo ratings yet
- ArtículoDocument8 pagesArtículo014100700jNo ratings yet
- Metformina y DiabetesDocument21 pagesMetformina y DiabetesBetty Isabel GarcíaNo ratings yet
- Metformin: Dosing & UsesDocument8 pagesMetformin: Dosing & UsesMaria Alejandra Siachoque JaraNo ratings yet
- Oral Management of Diabetes Type IIDocument34 pagesOral Management of Diabetes Type IIYasser Gebril100% (1)
- Canadian: Hypoglycemia: Understanding The EnemyDocument8 pagesCanadian: Hypoglycemia: Understanding The EnemyndistantiNo ratings yet
- DM2 Remissã o Dez 2022Document3 pagesDM2 Remissã o Dez 2022Bruna LempekNo ratings yet
- Contreras F. y Otros. (2008) - Effect of Drugs Interacting With The PDFDocument6 pagesContreras F. y Otros. (2008) - Effect of Drugs Interacting With The PDFjjg8116No ratings yet
- F 2433 CMED Saxagliptin A Selective DPP 4 Inhibitor For The Treatment of Type 2 D.PDF 3311Document12 pagesF 2433 CMED Saxagliptin A Selective DPP 4 Inhibitor For The Treatment of Type 2 D.PDF 3311Ridha Surya NugrahaNo ratings yet
- ADO1 Agst 2013Document48 pagesADO1 Agst 2013blackjackNo ratings yet
- Pharmacological Management of Type 1 DiabetesDocument6 pagesPharmacological Management of Type 1 DiabetesMI RFNo ratings yet
- TRIEXER ER TabletsDocument37 pagesTRIEXER ER TabletsJohn SukumarNo ratings yet
- Acute Complications of Diabetes MellitusDocument43 pagesAcute Complications of Diabetes MellitusalphaphoenixNo ratings yet
- GLIMITAB M-1/GLIMITAB M-2 Tablets: CompositionDocument6 pagesGLIMITAB M-1/GLIMITAB M-2 Tablets: Compositiongaurav7augNo ratings yet
- Pi GlucophageDocument35 pagesPi GlucophageJennyLapitanNo ratings yet
- Bioedge Mar '18 - 2 - ADA 2018 GuidelinesDocument4 pagesBioedge Mar '18 - 2 - ADA 2018 GuidelinesSiddiq MohammedNo ratings yet
- METFORMINDocument11 pagesMETFORMINsalsabila JacobNo ratings yet
- Metformin and Digestive DisordersDocument7 pagesMetformin and Digestive Disorders-Yohanes Firmansyah-No ratings yet
- 253 FullDocument18 pages253 FullpandemahendraNo ratings yet
- Trajenta DuoDocument30 pagesTrajenta DuoNovita Dewi LestariNo ratings yet
- 0304 Melillo MetforminDocument2 pages0304 Melillo MetformindavidshookNo ratings yet
- The Potency of Some Brands of Anti-Diabetic Medicine - Metformin Hydrochloride B.P 500 MG Tablet On The Ghanaian MarketDocument6 pagesThe Potency of Some Brands of Anti-Diabetic Medicine - Metformin Hydrochloride B.P 500 MG Tablet On The Ghanaian MarketAlexander DeckerNo ratings yet
- Charokopou 2015Document9 pagesCharokopou 2015Bella Nasar AlamriNo ratings yet
- Pitfalls in managing diabetes during hospitalization and illnessDocument7 pagesPitfalls in managing diabetes during hospitalization and illnessUmesh BabuNo ratings yet
- Update On: Diabetes MellitusDocument37 pagesUpdate On: Diabetes MellitusDr. Mamunul Abedin100% (1)
- AssignmentDocument5 pagesAssignmentStephen maurenNo ratings yet
- 11 Metformin in 2019Document5 pages11 Metformin in 2019haroldcaNo ratings yet
- Vildagliptin Improves Glycemic Control in Jordanian Patients with Type 2 DiabetesDocument5 pagesVildagliptin Improves Glycemic Control in Jordanian Patients with Type 2 DiabetesAlbert EdoNo ratings yet
- Management of Diabetes Mellitus in Surgical PatientsDocument12 pagesManagement of Diabetes Mellitus in Surgical PatientsAnggoro Bayu Agung DjangkaruNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Test 1 CAE Reading and Use of EnglishDocument3 pagesTest 1 CAE Reading and Use of EnglishLucian SiriteanuNo ratings yet
- Infectii de CateterDocument3 pagesInfectii de CateterLucian Siriteanu100% (1)
- ReviewDocument10 pagesReviewLucian SiriteanuNo ratings yet
- ReviewDocument10 pagesReviewLucian SiriteanuNo ratings yet
- Satoskar Bhandarker Cology PDFDocument1,852 pagesSatoskar Bhandarker Cology PDFTamanna Mohanty70% (10)
- SGLT2 Inhibitors: The Future For Treatment of Type 2 Diabetes Mellitus and Other Chronic DiseasesDocument6 pagesSGLT2 Inhibitors: The Future For Treatment of Type 2 Diabetes Mellitus and Other Chronic DiseasesLucian SiriteanuNo ratings yet
- SGLT2 Inhibitors and Mechanisms of Cardiovascular Benefit: A State-Of-The-Art ReviewDocument10 pagesSGLT2 Inhibitors and Mechanisms of Cardiovascular Benefit: A State-Of-The-Art ReviewLucian SiriteanuNo ratings yet
- Letter To The EditorDocument3 pagesLetter To The EditorLucian SiriteanuNo ratings yet
- The Actions of SGLT2 Inhibitors On Metabolism, Renal Function and Blood PressureDocument10 pagesThe Actions of SGLT2 Inhibitors On Metabolism, Renal Function and Blood PressureLucian SiriteanuNo ratings yet
- Evaluarea Hematuriei NEJMDocument11 pagesEvaluarea Hematuriei NEJMLucian SiriteanuNo ratings yet
- Evaluarea Hematuriei NEJMDocument11 pagesEvaluarea Hematuriei NEJMLucian SiriteanuNo ratings yet
- Solutii de Repletie VolemicaDocument1 pageSolutii de Repletie VolemicaLucian SiriteanuNo ratings yet
- Hyponatremia 2017Document10 pagesHyponatremia 2017Isnandita EmeraldaNo ratings yet
- Hyponatremia 2017Document10 pagesHyponatremia 2017Isnandita EmeraldaNo ratings yet
- Solutii de Repletie VolemicaDocument1 pageSolutii de Repletie VolemicaLucian SiriteanuNo ratings yet
- Acute Lung Edema Management PracticeDocument5 pagesAcute Lung Edema Management PracticeYunia DuanaNo ratings yet
- Acc Aha BradycardiaDocument191 pagesAcc Aha BradycardiaPanneer SelvamNo ratings yet
- Dermatologie Clinica Si VenerologieDocument384 pagesDermatologie Clinica Si VenerologieFlorin Patraşcu75% (4)
- CVA Case ClerkingDocument11 pagesCVA Case ClerkingOtaiKatiNo ratings yet
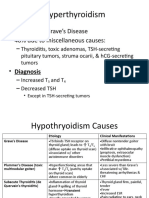
- Graves Disease and Hyperthyroidism Causes 60% of CasesDocument6 pagesGraves Disease and Hyperthyroidism Causes 60% of CasesLeitavia D.No ratings yet
- Escherichia ColiDocument31 pagesEscherichia ColiLizzie Fizzie100% (1)
- Pengaruh Cognitive Behavioral Therapy (CBT) Terhadap Perubahan Kecemasan, Mekanisme Koping, Harga Diri Pada Pasien Gangguan Jiwa Dengan SkizofreniaDocument23 pagesPengaruh Cognitive Behavioral Therapy (CBT) Terhadap Perubahan Kecemasan, Mekanisme Koping, Harga Diri Pada Pasien Gangguan Jiwa Dengan Skizofreniaharyati soyNo ratings yet
- Inborn Errors of Metabolism: Disorders of Amino AcidsDocument60 pagesInborn Errors of Metabolism: Disorders of Amino AcidsPyneandy KimberlyNo ratings yet
- Effect of Intraoperative Dexmedetomidine On Post-Craniotomy PainDocument9 pagesEffect of Intraoperative Dexmedetomidine On Post-Craniotomy PainIva SantikaNo ratings yet
- Amit BiomedSignalDocument14 pagesAmit BiomedSignalDr-Amit Kumar SinghNo ratings yet
- WW.04.05 Contraction Stress Test (Oxytocin Challenge Test) PDFDocument3 pagesWW.04.05 Contraction Stress Test (Oxytocin Challenge Test) PDFDiah Kurniawati100% (1)
- Implementasi Terapi Komplementer untuk Mengatasi Sesak pada Pasien ISPADocument5 pagesImplementasi Terapi Komplementer untuk Mengatasi Sesak pada Pasien ISPAMerdeka AgustinaNo ratings yet
- Uterine Rupture and Cervical TearDocument16 pagesUterine Rupture and Cervical Tearsangita patil0% (1)
- Caduet (Dr. Ismahun Maret 2009)Document41 pagesCaduet (Dr. Ismahun Maret 2009)Yulia SumarnaNo ratings yet
- Center For BrainHealthDocument5 pagesCenter For BrainHealthJames KuhnNo ratings yet
- Care of The Acutely Unwell FinalDocument100 pagesCare of The Acutely Unwell Finalgireeshsachin100% (1)
- Pharmacology NotesDocument6 pagesPharmacology NotesHarsh PawarNo ratings yet
- The 4th Edition of The Head and Neck WHO Blue BookDocument11 pagesThe 4th Edition of The Head and Neck WHO Blue Bookjarzcorpify100% (1)
- Jordanian Surgical Society - PPT LastDocument166 pagesJordanian Surgical Society - PPT LastNessreen Jamal100% (1)
- AneurysmDocument10 pagesAneurysmMarquel CulmerNo ratings yet
- Community Health Nursing Board ExamDocument15 pagesCommunity Health Nursing Board Examrhenier_ilado86% (14)
- Achilles Tendinopathy What Runners Should Know FinitoDocument4 pagesAchilles Tendinopathy What Runners Should Know FinitoAdmirNo ratings yet
- Explaining StrokeDocument16 pagesExplaining StrokeAhmed GaberNo ratings yet
- Kalium DuruleDocument3 pagesKalium DuruleRhika Mae Flores ValdezNo ratings yet
- Bronchiolitis Obliterans PDFDocument7 pagesBronchiolitis Obliterans PDFSatnam KaurNo ratings yet
- Nclex New Lastest 1Document240 pagesNclex New Lastest 1Nadim KhalidNo ratings yet
- The Incidence of Venous Thromboembolism in Commercial Airline Pilots. A Cohort Study of 2630 PilotsDocument6 pagesThe Incidence of Venous Thromboembolism in Commercial Airline Pilots. A Cohort Study of 2630 Pilotsluis11256No ratings yet
- Interaksi Obat Obat MaagDocument8 pagesInteraksi Obat Obat MaagSiti NurohmahhNo ratings yet
- (Psychological Disorders) Vatsal Thakkar, Pat Levitt - Depression and Bipolar Disorder-Chelsea House Publications (2006) PDFDocument111 pages(Psychological Disorders) Vatsal Thakkar, Pat Levitt - Depression and Bipolar Disorder-Chelsea House Publications (2006) PDFUrsache BogdanNo ratings yet
- MnemonicS in OphthaDocument22 pagesMnemonicS in Ophthaabuahmed&janaNo ratings yet
- Diabetic Medicine - 2022 - Dhatariya - The Management of Diabetic Ketoacidosis in Adults An Updated Guideline From TheDocument20 pagesDiabetic Medicine - 2022 - Dhatariya - The Management of Diabetic Ketoacidosis in Adults An Updated Guideline From Thenguyenngocanh9798No ratings yet
- Ncm117-Lecture NotesDocument18 pagesNcm117-Lecture NotesTherese Margaret100% (1)
- CORDERO Performance Task 5Document1 pageCORDERO Performance Task 5Maria Hilda Vicio AragonNo ratings yet