You might also like
- Annotated-Cortez 642 Needs 20assessment 20report 20 282 29 1Document18 pagesAnnotated-Cortez 642 Needs 20assessment 20report 20 282 29 1api-643542636No ratings yet
- Nutr 642 Needs Assessment 2Document17 pagesNutr 642 Needs Assessment 2api-644004909No ratings yet
- Prevalence of Diabetes, Associated Symptoms and Risk Factors Among University StudentsDocument8 pagesPrevalence of Diabetes, Associated Symptoms and Risk Factors Among University Studentsijmb333No ratings yet
- Health Center - PaterosDocument5 pagesHealth Center - PaterosmawaaahNo ratings yet
- Needs Assessment 11Document16 pagesNeeds Assessment 11api-434499729No ratings yet
- Keenan Amanda Community Needs AssessmnetDocument16 pagesKeenan Amanda Community Needs Assessmnetapi-710211553No ratings yet
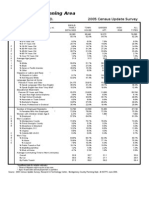
- North Bethesda/Garrett Park Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument2 pagesNorth Bethesda/Garrett Park Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
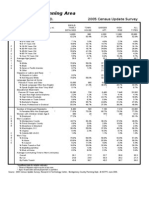
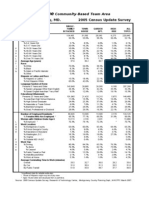
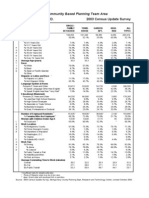
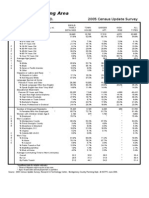
- Rockville Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument2 pagesRockville Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Oral Health Program 1-2 2Document19 pagesOral Health Program 1-2 2api-336681944No ratings yet
- Kensington / University Boulevard Sector Plan: Montgomery County, MD. 2005 Census Update SurveyDocument2 pagesKensington / University Boulevard Sector Plan: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Georgia Avenue Corridor: 2005 Census Update SurveyDocument2 pagesGeorgia Avenue Corridor: 2005 Census Update SurveyM-NCPPCNo ratings yet
- Aspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument44 pagesAspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Aspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument2 pagesAspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Data Analysis and Interpretation of HIV KnowledgeDocument23 pagesData Analysis and Interpretation of HIV KnowledgeKaryl CanaresNo ratings yet
- Germantown Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument7 pagesGermantown Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- COVID-19 Mass Vaccination Analysis 3-22-2021-UPDATEDocument11 pagesCOVID-19 Mass Vaccination Analysis 3-22-2021-UPDATEDavid IbanezNo ratings yet
- Silver Spring Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument7 pagesSilver Spring Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Case Ana Pancreatic CaDocument21 pagesCase Ana Pancreatic CakingpinNo ratings yet
- Potomac: Montgomery County, MD. 2005 Census Update SurveyDocument2 pagesPotomac: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Appendix 2: Germantown Planning Area Demographics Research & Technology Center (RTC)Document6 pagesAppendix 2: Germantown Planning Area Demographics Research & Technology Center (RTC)M-NCPPCNo ratings yet
- Bethesda/Chevy Chase Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument2 pagesBethesda/Chevy Chase Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Running Head: Health Outcomes in San Bernardino County 1Document8 pagesRunning Head: Health Outcomes in San Bernardino County 1api-301955307No ratings yet
- Aspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument42 pagesAspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Ypsilanti Community Needs Assessment-Morgan JonesDocument16 pagesYpsilanti Community Needs Assessment-Morgan Jonesapi-701100692No ratings yet
- Georgia Avenue: Montgomery County, MD. 2005 Census Update SurveyDocument7 pagesGeorgia Avenue: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- 2011 Breastfeeding Report CardDocument4 pages2011 Breastfeeding Report CardZulaicha MumarridzohNo ratings yet
- I-270 Corridor: Montgomery County, MD. 2003 Census Update SurveyDocument2 pagesI-270 Corridor: Montgomery County, MD. 2003 Census Update SurveyM-NCPPCNo ratings yet
- Albemarle County Drive Time Demographics From The Center of US 29 and RIO RoadDocument6 pagesAlbemarle County Drive Time Demographics From The Center of US 29 and RIO Roadapi-25884944No ratings yet
- Bethesda/Chevy Chase Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument7 pagesBethesda/Chevy Chase Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Germantown Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument2 pagesGermantown Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- CDC - Breast Cancer Screening RatesDocument3 pagesCDC - Breast Cancer Screening RatesemedjuckNo ratings yet
- Regional Services Centers : Montgomery County, MD. 2005 Census Update SurveyDocument2 pagesRegional Services Centers : Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Clark County COVID-19 Testing Results-JulyDocument2 pagesClark County COVID-19 Testing Results-JulyJosh RichardsonNo ratings yet
- North Bethesda/Garrett Park Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument7 pagesNorth Bethesda/Garrett Park Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Bethesda-Chevy Ch./N. Beth.: Montgomery County, MD. 2003 Census Update SurveyDocument2 pagesBethesda-Chevy Ch./N. Beth.: Montgomery County, MD. 2003 Census Update SurveyM-NCPPCNo ratings yet
- Mid-County: Montgomery County, MD. 2005 Census Update SurveyDocument7 pagesMid-County: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- How Are Income and Wealth Linked To Health and LongevityDocument22 pagesHow Are Income and Wealth Linked To Health and Longevityshu100% (2)
- May 2013 Project Connect Report-FinalDocument17 pagesMay 2013 Project Connect Report-Finalapi-218293468No ratings yet
- Eastern County: Montgomery County, MD. 2005 Census Update SurveyDocument2 pagesEastern County: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Chronic Disease ProfileDocument18 pagesChronic Disease ProfileFELIX KIPKORIRNo ratings yet
- Aspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument7 pagesAspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Aspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument147 pagesAspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- bm13 BRC Census ReportDocument58 pagesbm13 BRC Census Reportapi-260102290No ratings yet
- 12 - CHEER Predicting PreDM CVD Risk Obese TeensDocument61 pages12 - CHEER Predicting PreDM CVD Risk Obese TeensMinerva StanciuNo ratings yet
- Prevalence of Overweight and Obesity Among US Children, Adolescents, and Adults, 1999-2002Document4 pagesPrevalence of Overweight and Obesity Among US Children, Adolescents, and Adults, 1999-2002cubewormNo ratings yet
- Mid-County: Montgomery County, MD. 2005 Census Update SurveyDocument2 pagesMid-County: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Eastern CountyDocument2 pagesEastern CountyM-NCPPCNo ratings yet
- Poolesville & Vicinity Planning Areas: Montgomery County, MD. 2005 Census Update SurveyDocument7 pagesPoolesville & Vicinity Planning Areas: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Potomac/Cabin John Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument2 pagesPotomac/Cabin John Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Assessment Test. RevisedDocument16 pagesAssessment Test. RevisedBrian KyaloNo ratings yet
- South Carolina: 2018 County Health Rankings ReportDocument16 pagesSouth Carolina: 2018 County Health Rankings ReportGreenville NewsNo ratings yet
- Colesville/White Oak Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument2 pagesColesville/White Oak Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Travilah Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument2 pagesTravilah Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- ABR-MSUE County Portrait ClareDocument16 pagesABR-MSUE County Portrait ClareDaveNo ratings yet
- Nline Eight Management Ounseling Program For Ealthcare ProvidersDocument59 pagesNline Eight Management Ounseling Program For Ealthcare ProvidershermestriNo ratings yet
- Abstrack Latar Belakang Tujuan Metodologi (Sample) Hasil Kesimpulan Max. 300 Kata. Keywords 4Document6 pagesAbstrack Latar Belakang Tujuan Metodologi (Sample) Hasil Kesimpulan Max. 300 Kata. Keywords 4stephanie carolineNo ratings yet
- Residents Aged 65 and Older: The Share of Population Age 65+ Continues To GrowDocument6 pagesResidents Aged 65 and Older: The Share of Population Age 65+ Continues To GrowM-NCPPCNo ratings yet
- Bus Plan RojeanDocument18 pagesBus Plan RojeanMark LuceroNo ratings yet
- The tragedy of COVID-19 maternal deaths in BrazilDocument3 pagesThe tragedy of COVID-19 maternal deaths in BrazilPrix_aeNo ratings yet
- MUET Reading Task - Print OutDocument5 pagesMUET Reading Task - Print Out萱儿林No ratings yet
- 50 Fun Facts About JapanDocument4 pages50 Fun Facts About JapanChristine AntiqueraNo ratings yet
- Unsu Explantation PDFDocument7 pagesUnsu Explantation PDFBondhan Adi PratomoNo ratings yet
- Yellow Cab LawsuitDocument38 pagesYellow Cab LawsuitMichael RobertsNo ratings yet
- The Authors Guild vs. Google, Inc. Facts: Plaintiffs, Who Are Authors of Published Books UnderDocument15 pagesThe Authors Guild vs. Google, Inc. Facts: Plaintiffs, Who Are Authors of Published Books UnderElead Gaddiel S. AlbueroNo ratings yet
- Lesson PlanDocument3 pagesLesson Planapi-479604636No ratings yet
- Scientific Theological Aspects of GeocentricityDocument222 pagesScientific Theological Aspects of GeocentricityAdi Dumitru100% (1)
- Journal All Pages Jan2019 PDFDocument68 pagesJournal All Pages Jan2019 PDFmahadev_prasad_7No ratings yet
- Happiest People On EarthDocument79 pagesHappiest People On EarthVictoria muneneNo ratings yet
- WNL Slum Golf The Sport That Stormed The Streets of Mumbai UppDocument5 pagesWNL Slum Golf The Sport That Stormed The Streets of Mumbai UppStephen McKennaNo ratings yet
- 1 Fill in The Right Article: X / The. 21pDocument3 pages1 Fill in The Right Article: X / The. 21pNo YesNo ratings yet
- CRMDocument32 pagesCRMJoel Dsouza100% (1)
- Leyte Edible Oil Supervisors and Confidential20170704-911-1fckbjxDocument12 pagesLeyte Edible Oil Supervisors and Confidential20170704-911-1fckbjxJustin ParasNo ratings yet
- Change Management PresentationDocument15 pagesChange Management PresentationAshu AyshaNo ratings yet
- Chapter 2 Problems Working PapersDocument28 pagesChapter 2 Problems Working PapersZachLoving0% (1)
- Article 3.07Document29 pagesArticle 3.07khajehNo ratings yet
- Comparing Chinese and Pakistani EtiquetteDocument29 pagesComparing Chinese and Pakistani Etiquettemuhammad kaunain khanNo ratings yet
- Central Luzon Doctors' Hospital Nursing Drug StudyDocument7 pagesCentral Luzon Doctors' Hospital Nursing Drug StudyJane BautistaNo ratings yet
- Research in Daily Life 2Document166 pagesResearch in Daily Life 2Zianna Marie De RamosNo ratings yet
- Ephemeris 01012009 To 19022011Document15 pagesEphemeris 01012009 To 19022011prvnprvnNo ratings yet
- One Foot in The Grave - Copy For PlayersDocument76 pagesOne Foot in The Grave - Copy For Playerssveni meierNo ratings yet
- ResumeDocument2 pagesResumeapi-299996983No ratings yet
- Badass 3.5e Prestige ClassDocument4 pagesBadass 3.5e Prestige ClassTony HolcombNo ratings yet
- 2nd EditionDocument93 pages2nd EditionDhandapani NagarajanNo ratings yet
- Swapan Kumar Nath Sanjay G Revankar Problem-Based PDFDocument1,163 pagesSwapan Kumar Nath Sanjay G Revankar Problem-Based PDFRestu100% (1)
- Remove Phenol using Activated CarbonDocument10 pagesRemove Phenol using Activated CarbonjimboNo ratings yet
- Flexible Budgets and Variance AnalysisDocument50 pagesFlexible Budgets and Variance AnalysisRanjini SettyNo ratings yet
- Daphnia Write UpDocument3 pagesDaphnia Write UpASDFGHJKL9571% (7)
- Engineering Prob & Stat Lecture Notes 6Document12 pagesEngineering Prob & Stat Lecture Notes 6EICQ/00154/2020 SAMUEL MWANGI RUKWARONo ratings yet
- Professional CV FormatDocument2 pagesProfessional CV FormatShawn ParkerNo ratings yet