You might also like
- Coding Cheat Sheet For Residents in Outpatient MedicineDocument3 pagesCoding Cheat Sheet For Residents in Outpatient MedicineRayCTsai86% (21)
- Free Nclex QuestionsDocument161 pagesFree Nclex QuestionspadmaNo ratings yet
- Avascular Necrosis HipDocument4 pagesAvascular Necrosis HipVidyasagar ReddyNo ratings yet
- Kerri Maniscalco - Meeting Thomas CresswellDocument38 pagesKerri Maniscalco - Meeting Thomas CresswelldbbahahabNo ratings yet
- Screening BDDQ PDFDocument37 pagesScreening BDDQ PDFManuelaMartinezNo ratings yet
- Plastic Surgery Essential 2012Document110 pagesPlastic Surgery Essential 2012Guillermo Meneses100% (1)
- Psychopathology Among Individuals Seeking Minimally InvasiveDocument7 pagesPsychopathology Among Individuals Seeking Minimally InvasiveIsteuria CristinaNo ratings yet
- A Review of Body Dysmorphic Disorder in Aesthetic Surgery Patients and The Legal ImplicationsDocument6 pagesA Review of Body Dysmorphic Disorder in Aesthetic Surgery Patients and The Legal ImplicationsJuliano MarquesNo ratings yet
- SaudiSurgJ7383-3029712 082457Document4 pagesSaudiSurgJ7383-3029712 082457kalwusaidiNo ratings yet
- Identification of Body Dysmorphic Disorder In.38Document4 pagesIdentification of Body Dysmorphic Disorder In.38Fábio LopesNo ratings yet
- Aesthetic Concerns Are Core Business - APSDocument7 pagesAesthetic Concerns Are Core Business - APSAbigail MJNo ratings yet
- Gox 8 E2737Document6 pagesGox 8 E27371klinikpsixologiyaNo ratings yet
- Nihms 275889Document13 pagesNihms 275889marcelo.andrade.007.mfNo ratings yet
- Prevalence of Body Dysmorphic Disorder Among Female Patients Seeking Cosmetic ProceduresDocument5 pagesPrevalence of Body Dysmorphic Disorder Among Female Patients Seeking Cosmetic ProceduresIJAR JOURNALNo ratings yet
- The Impact of Obesity On Plastic SurgeryDocument13 pagesThe Impact of Obesity On Plastic SurgeryCao TrầnNo ratings yet
- Health Science Reports - 2023 - Nabavizadeh - Prevalence of Body Dysmorphic Disorder in Rhinoplasty Candidates ADocument11 pagesHealth Science Reports - 2023 - Nabavizadeh - Prevalence of Body Dysmorphic Disorder in Rhinoplasty Candidates Ahans jablonskyNo ratings yet
- Body Dysmorphic Disorder: Facialplastic Surgeryclinics OfnorthamericaDocument7 pagesBody Dysmorphic Disorder: Facialplastic Surgeryclinics OfnorthamericaTasya Ajeng Trias PutriNo ratings yet
- 1 s2.0 S0950705112001840 MainDocument13 pages1 s2.0 S0950705112001840 Main1201200152No ratings yet
- 2021 - Saki - Comparison of The Efficacy of Microneedling Versus CO2 Fractional Laser To TreatDocument8 pages2021 - Saki - Comparison of The Efficacy of Microneedling Versus CO2 Fractional Laser To Treatتسنيم الصيادNo ratings yet
- 2008 - SARWER CASH - Body Image Interfacing Behavioral andDocument2 pages2008 - SARWER CASH - Body Image Interfacing Behavioral andCarolina RuasNo ratings yet
- Body Dysmorphic Disorder in AestheticDocument5 pagesBody Dysmorphic Disorder in AestheticPaula ArenasNo ratings yet
- DNB Cardiology ThesisDocument5 pagesDNB Cardiology Thesisgloriayoungdesmoines100% (3)
- Translation, Cross-Cultural Adaptation and Validation of The Mandarin Version of The BDDQ-AS For Rhinoplasty PatientsDocument9 pagesTranslation, Cross-Cultural Adaptation and Validation of The Mandarin Version of The BDDQ-AS For Rhinoplasty PatientsWilson Adrian WijayaNo ratings yet
- JN2XX 17 PDFDocument7 pagesJN2XX 17 PDFijasrjournalNo ratings yet
- OET - Writing SamplesDocument4 pagesOET - Writing SamplesMazen Mira50% (2)
- Research PaperDocument6 pagesResearch Paperchentiffany01No ratings yet
- La Padula 2019Document7 pagesLa Padula 2019Carolina Hoch FariasNo ratings yet
- 3investigating Psychosocial Causes of The Tendency For Facial Cosmetic Surgery.Document7 pages3investigating Psychosocial Causes of The Tendency For Facial Cosmetic Surgery.doctorshomare1No ratings yet
- Research Paper On Wound CareDocument5 pagesResearch Paper On Wound Carec9rbzcr0100% (1)
- Dissertation Topics General SurgeryDocument5 pagesDissertation Topics General SurgeryWhereCanIFindSomeoneToWriteMyCollegePaperCanada100% (1)
- PIIS074152141731145XDocument10 pagesPIIS074152141731145XGooDon LeeNo ratings yet
- Gist ThesisDocument4 pagesGist ThesisLori Mitchell100% (2)
- Thoughts On A Live Debate: Is Psychological Assessment Robust Enough For Patients?Document2 pagesThoughts On A Live Debate: Is Psychological Assessment Robust Enough For Patients?api-240232877No ratings yet
- Psychiatric Assessment and Management of Clients Undergoing Cosmetic Surgery: Overview and Need For An Integrated ApproachDocument12 pagesPsychiatric Assessment and Management of Clients Undergoing Cosmetic Surgery: Overview and Need For An Integrated ApproachNatalia López Aliaga UndaNo ratings yet
- Awareness and Knowledge Towards Common Eye Diseases of Citizens in Medina City, Saudi ArabiaDocument7 pagesAwareness and Knowledge Towards Common Eye Diseases of Citizens in Medina City, Saudi ArabiaIJAR JOURNALNo ratings yet
- Body Image, Cosmetic Surgery, and Minimally Invasive TreatmentsDocument7 pagesBody Image, Cosmetic Surgery, and Minimally Invasive TreatmentsJuliano Marques100% (1)
- Os Ideais de Beleza Facial Entre A Estética Chinesa Praticantes Resultados de Uma Grande Pesquisa NacionalDocument13 pagesOs Ideais de Beleza Facial Entre A Estética Chinesa Praticantes Resultados de Uma Grande Pesquisa NacionalIsabelle Araújo OliveiraNo ratings yet
- Rajiv Gandhi Medical College Thesis TopicsDocument8 pagesRajiv Gandhi Medical College Thesis Topicsseewbyvff100% (2)
- Evaluation of Relationship Between Body Dysmorphic Disorder and Self-Esteem in Rhinoplasty Candidates PDFDocument3 pagesEvaluation of Relationship Between Body Dysmorphic Disorder and Self-Esteem in Rhinoplasty Candidates PDFcokyNo ratings yet
- Informative Paper - Artificial Intelligence in Cosmetic SurgeryDocument10 pagesInformative Paper - Artificial Intelligence in Cosmetic Surgeryapi-611115078No ratings yet
- Wound Care ThesisDocument4 pagesWound Care Thesiscandacedaiglelafayette100% (2)
- 35-Analysis of The Factors Affecting Men's Attitudes Toward Cosmetic SurgeryDocument9 pages35-Analysis of The Factors Affecting Men's Attitudes Toward Cosmetic SurgeryJanina BazalarNo ratings yet
- Nursing Research PaperDocument11 pagesNursing Research Paperapi-663012445No ratings yet
- Paper Final Complete Group6Document16 pagesPaper Final Complete Group6api-524151719No ratings yet
- Eclinicalmedicine: Sabrina Donzelli, Fabio Zaina, Stefano NegriniDocument2 pagesEclinicalmedicine: Sabrina Donzelli, Fabio Zaina, Stefano NegrinirenihardiyantiNo ratings yet
- IDRiD Diabetic Retinopathy - Segmentation and Grading ChallengeDocument26 pagesIDRiD Diabetic Retinopathy - Segmentation and Grading ChallengeSAMIKSHA PACHADENo ratings yet
- Research Paper Skin CancerDocument7 pagesResearch Paper Skin Cancersuw1vadibys2100% (1)
- Literature Review Breast EngorgementDocument7 pagesLiterature Review Breast Engorgementfvhqqm3b100% (1)
- CosmeticsDocument11 pagesCosmeticsdoctorshomare1No ratings yet
- 1 s2.0 S1658361219301052 MainDocument9 pages1 s2.0 S1658361219301052 MainkalwusaidiNo ratings yet
- Cancer Dissertation AwardDocument5 pagesCancer Dissertation AwardPaperWritersCanada100% (1)
- TEMA 2 BEDAH FixDocument32 pagesTEMA 2 BEDAH FixrahmanNo ratings yet
- DIR Spring 2022Document8 pagesDIR Spring 2022kahkashanahmed065No ratings yet
- Paediatric Radiography DissertationDocument4 pagesPaediatric Radiography DissertationGhostWriterCollegePapersHartford100% (1)
- World Journal Of: Clinical CasesDocument10 pagesWorld Journal Of: Clinical CasesMATEJ MAMICNo ratings yet
- CrerandFranklin BDD 2006Document14 pagesCrerandFranklin BDD 2006marcelo.andrade.007.mfNo ratings yet
- Breast Cancer Detection Using Machine LearningDocument6 pagesBreast Cancer Detection Using Machine LearningIJRASETPublicationsNo ratings yet
- Visualization and Quantification of The AssociatioDocument10 pagesVisualization and Quantification of The AssociatioFernando Lapuente-GarcíaNo ratings yet
- Body Dysmorphic Disorder: A Screening Guide For OrthodontistsDocument4 pagesBody Dysmorphic Disorder: A Screening Guide For Orthodontistsdruzair007No ratings yet
- Knowledge, Attitude and Practice of Family Physicians Toward Obesity Counseling in Cluster One, Riyadh, Saudi ArabiaDocument7 pagesKnowledge, Attitude and Practice of Family Physicians Toward Obesity Counseling in Cluster One, Riyadh, Saudi ArabiaIJAR JOURNALNo ratings yet
- Complications Associated With Medical Tourism For Facial Rejuvenation - A Systematic ReviewDocument8 pagesComplications Associated With Medical Tourism For Facial Rejuvenation - A Systematic ReviewKerlida SantosNo ratings yet
- Rguhs Thesis SynopsisDocument6 pagesRguhs Thesis Synopsisafloziubadtypc100% (2)
- 2013 - Tamizaje de Cancer en Ancianos Con DiscapacidadDocument6 pages2013 - Tamizaje de Cancer en Ancianos Con DiscapacidadRodrigoMarinNo ratings yet
- Recent Advances in Understanding and Managing BodyDocument6 pagesRecent Advances in Understanding and Managing BodyFábio LopesNo ratings yet
- 4 - VealeDocument81 pages4 - VealeFábio LopesNo ratings yet
- 54 Topico 4Document9 pages54 Topico 4Fábio LopesNo ratings yet
- Claim Your Free PDF ConverterDocument1 pageClaim Your Free PDF ConverterFábio LopesNo ratings yet
- Victorian HospitalsDocument55 pagesVictorian Hospitalshadia_unitedNo ratings yet
- Surgical InstrumentDocument89 pagesSurgical Instrumentravi rana100% (1)
- Correcta Posicion Del TornilloDocument5 pagesCorrecta Posicion Del TornilloSilvia PluisNo ratings yet
- HRC 3 MPDocument21 pagesHRC 3 MPDespoina KolaNo ratings yet
- Obesity and Pelvic Floor March 2018Document5 pagesObesity and Pelvic Floor March 2018Elsa KarinasariNo ratings yet
- Granny Part 2Document2 pagesGranny Part 2roosteenee50% (2)
- Paper+4+ (2022 2 1) +Analysis+of+Medical+Term+Translation+Techniques+in+the+Five+Feet+Apart+NovelDocument8 pagesPaper+4+ (2022 2 1) +Analysis+of+Medical+Term+Translation+Techniques+in+the+Five+Feet+Apart+NovelditahermaNo ratings yet
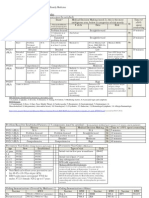
- Quality of Care: AREAS OF VISIT - : The Community Health Center (CHC) - DUDU On 19Document4 pagesQuality of Care: AREAS OF VISIT - : The Community Health Center (CHC) - DUDU On 19Yogesh PandeNo ratings yet
- City of Carmel-By-The-Sea: City Council Staff ReportDocument13 pagesCity of Carmel-By-The-Sea: City Council Staff ReportL. A. PatersonNo ratings yet
- Dehisced Surgical Wounds - Medihoney Power Webinar Episode 9Document42 pagesDehisced Surgical Wounds - Medihoney Power Webinar Episode 9Lynn Paredes MargullisNo ratings yet
- ART Rules March, 2022-1 PDFDocument96 pagesART Rules March, 2022-1 PDFsasankNo ratings yet
- Nursing Attendant-Ii, Ipcr ParametersDocument4 pagesNursing Attendant-Ii, Ipcr ParametersEldwinCauilanNo ratings yet
- Micro-Line Straight Handpiece-Angled Handpiece (TA-Nr. 012581) (03-13)Document6 pagesMicro-Line Straight Handpiece-Angled Handpiece (TA-Nr. 012581) (03-13)Renata NataNo ratings yet
- Training in LaparosDocument11 pagesTraining in LaparosEbrahim ShabaanNo ratings yet
- Health Bulletin 2019 Print Version (2) - FinalDocument263 pagesHealth Bulletin 2019 Print Version (2) - FinalNousen TaraNo ratings yet
- Director Marketing Product Manager in Minneapolis MN Resume Judy EastmanDocument3 pagesDirector Marketing Product Manager in Minneapolis MN Resume Judy EastmanJudyEastmanNo ratings yet
- Reducing Surgical Risks inDocument12 pagesReducing Surgical Risks inRaul FonsecaNo ratings yet
- Barotac Viejo District HospitalDocument16 pagesBarotac Viejo District Hospitaldocdumdum50% (2)
- Total Gastrectomy ConsentDocument18 pagesTotal Gastrectomy ConsentTanyaNganNo ratings yet
- J Vet Emergen Crit Care - 2022 - Lee - Epidemiology of Severe Trauma in Cats An ACVECC VetCOT Registry StudyDocument9 pagesJ Vet Emergen Crit Care - 2022 - Lee - Epidemiology of Severe Trauma in Cats An ACVECC VetCOT Registry StudyGuillermo MuzasNo ratings yet
- Flexor Tendon Repair Rehabilitation Protocols - A Systematic ReviewDocument20 pagesFlexor Tendon Repair Rehabilitation Protocols - A Systematic ReviewPatricio VásquezNo ratings yet
- Post-Operative Sore Throat in Ett PatientsDocument3 pagesPost-Operative Sore Throat in Ett PatientsSA SHNo ratings yet
- Chlorhexidine-Alcohol Compared With Povidone-Iodine Preoperative Skin Antisepsis For Cesarean Delivery A Systematic Review and Meta-AnalysisDocument6 pagesChlorhexidine-Alcohol Compared With Povidone-Iodine Preoperative Skin Antisepsis For Cesarean Delivery A Systematic Review and Meta-AnalysisjohnturpoNo ratings yet
- Extravasation GuidanceDocument24 pagesExtravasation Guidancechercal100% (1)
- Admission, Criteria - Adult Intensive Care Unit.Document5 pagesAdmission, Criteria - Adult Intensive Care Unit.EsamNo ratings yet
- Parcus SutureDocument1 pageParcus SutureJuan Martinez Del AngelNo ratings yet