You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Break Your Leg InternDocument199 pagesBreak Your Leg InternkingNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Hesi Psych Study GuideDocument16 pagesHesi Psych Study GuideR100% (17)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Nclex DiseasesDocument6 pagesNclex Diseasesshangguanlongkui95% (21)
- Larynx Wrote by DR Nassem TalaatDocument38 pagesLarynx Wrote by DR Nassem TalaatAbouzr Mohammed ElsaidNo ratings yet
- Case Study HELLPDocument7 pagesCase Study HELLPJovirtNo ratings yet
- Journal Reading RPL EditDocument30 pagesJournal Reading RPL EditAnonymous l6Q1ROq2No ratings yet
- Maternal Mortality in Women With Pre Viable Premature Rupture of MembranesDocument8 pagesMaternal Mortality in Women With Pre Viable Premature Rupture of MembranesAnonymous l6Q1ROq2No ratings yet
- BJOG - 2022 - Tessema - The Role of Intervening Pregnancy Loss in The Association Between Interpregnancy Interval andDocument9 pagesBJOG - 2022 - Tessema - The Role of Intervening Pregnancy Loss in The Association Between Interpregnancy Interval andAnonymous l6Q1ROq2No ratings yet
- Medical Management of Prgenancy LossDocument11 pagesMedical Management of Prgenancy LossAnonymous l6Q1ROq2No ratings yet
- Cervical Cancer Mortality in Norway According To Screening Attendance and AgeDocument8 pagesCervical Cancer Mortality in Norway According To Screening Attendance and AgeAnonymous l6Q1ROq2No ratings yet
- Diagnostics 12 01931 2Document30 pagesDiagnostics 12 01931 2Anonymous l6Q1ROq2No ratings yet
- Effects of Hysterectomy On Pelvic Floor Function and Sexual Function ADocument9 pagesEffects of Hysterectomy On Pelvic Floor Function and Sexual Function AAnonymous l6Q1ROq2No ratings yet
- Maternal Mortality in 8 European Countries With Enhanced Surveillance SystemsDocument10 pagesMaternal Mortality in 8 European Countries With Enhanced Surveillance SystemsAnonymous l6Q1ROq2No ratings yet
- Fmed 09 945621Document10 pagesFmed 09 945621Anonymous l6Q1ROq2No ratings yet
- The Effect of Paternal and Maternal Factors On The Prognosis of Live Birth inDocument12 pagesThe Effect of Paternal and Maternal Factors On The Prognosis of Live Birth inAnonymous l6Q1ROq2No ratings yet
- BJOG - 2022 - Weelden - The Effect of Progestin Therapy in Advanced and Recurrent Endometrial Cancer A Systematic ReviewDocument10 pagesBJOG - 2022 - Weelden - The Effect of Progestin Therapy in Advanced and Recurrent Endometrial Cancer A Systematic ReviewAnonymous l6Q1ROq2No ratings yet
- BJOG - 2022 - Woo Kinshella - Calcium For Pre Eclampsia Prevention A Systematic Review and Network Meta Analysis To GuideDocument11 pagesBJOG - 2022 - Woo Kinshella - Calcium For Pre Eclampsia Prevention A Systematic Review and Network Meta Analysis To GuideAnonymous l6Q1ROq2No ratings yet
- BJOG - 2022 - Demakakos - Adverse Childhood Experiences Are Associated With Increased Risk of Hysterectomy and BilateralDocument9 pagesBJOG - 2022 - Demakakos - Adverse Childhood Experiences Are Associated With Increased Risk of Hysterectomy and BilateralAnonymous l6Q1ROq2No ratings yet
- Maternal VaccinationDocument16 pagesMaternal VaccinationAnonymous l6Q1ROq2No ratings yet
- BJOG - 2022 - Beardmore Gray - Two Year Follow Up of Infant and Maternal Outcomes After Planned Early Delivery or ExpectantDocument10 pagesBJOG - 2022 - Beardmore Gray - Two Year Follow Up of Infant and Maternal Outcomes After Planned Early Delivery or ExpectantAnonymous l6Q1ROq2No ratings yet
- Postpartum Eclampsia or PreeclampsiaDocument11 pagesPostpartum Eclampsia or PreeclampsiaAnonymous l6Q1ROq2No ratings yet
- Materials. Atlanta, Georgia: U.S. Department of Health and Human ServicesDocument1 pageMaterials. Atlanta, Georgia: U.S. Department of Health and Human ServicesAnonymous l6Q1ROq2No ratings yet
- Medical Board - Guidelines - Registered Health Practitioners and Students in Relation To Blood Borne VirusesDocument57 pagesMedical Board - Guidelines - Registered Health Practitioners and Students in Relation To Blood Borne Virusesddavies69No ratings yet
- Keanekaragaman Dan Dominasi Nyamuk Di Daerah Endemis Filariasis Limfatik, Kota PekalonganDocument9 pagesKeanekaragaman Dan Dominasi Nyamuk Di Daerah Endemis Filariasis Limfatik, Kota PekalonganabighofurNo ratings yet
- Reuma ToDocument15 pagesReuma ToMuzahem ZetawiNo ratings yet
- Drug and AlcoholDocument5 pagesDrug and AlcoholLèoñà LeiphakNo ratings yet
- Annals of General Psychiatry: The Nosological Significance of Folie À Deux: A Review of The LiteratureDocument8 pagesAnnals of General Psychiatry: The Nosological Significance of Folie À Deux: A Review of The LiteratureAnonymous A2d5hUNeMiNo ratings yet
- Sarcoidoza Ers Ghid - FullDocument251 pagesSarcoidoza Ers Ghid - FullCătălina BlajinNo ratings yet
- Superfical and CutaneousDocument53 pagesSuperfical and CutaneousmulatumeleseNo ratings yet
- READING ON Tick-Borne DiseasesDocument3 pagesREADING ON Tick-Borne DiseasesMonique LeonardoNo ratings yet
- An Overview of Muscle Histopathology in Myositis: Differentiating Subtypes of MyositisDocument35 pagesAn Overview of Muscle Histopathology in Myositis: Differentiating Subtypes of MyositisIsaac MaderoNo ratings yet
- Case History and Data Interpretation in Medical PracticeDocument563 pagesCase History and Data Interpretation in Medical PracticesaifabaasNo ratings yet
- Adalimumab: General InformationDocument6 pagesAdalimumab: General InformationAhmed Ben MohamedNo ratings yet
- Concepts of Man and His Basic Human NeedsDocument7 pagesConcepts of Man and His Basic Human Needsharold dimaiwatNo ratings yet
- 10.1 AstringentsDocument32 pages10.1 AstringentsSaha DirllahNo ratings yet
- Immunology Mcqs-4: InstructionsDocument22 pagesImmunology Mcqs-4: InstructionsadehkordiNo ratings yet
- MedicinalDocument12 pagesMedicinalchrist.sony95No ratings yet
- AutismDocument11 pagesAutismapi-347584593No ratings yet
- Damage Control SurgeryDocument31 pagesDamage Control SurgeryDyo Resna100% (1)
- High-Risk Newborn Small For Gestational Age WhatDocument3 pagesHigh-Risk Newborn Small For Gestational Age WhatimUrb00100% (1)
- Neurologic Disorders Associated With Mitral Valve ProlapseDocument6 pagesNeurologic Disorders Associated With Mitral Valve Prolapsegeorgiana_884431330No ratings yet
- Therese Ronamae Loquez2 - Patient Drug DatabaseDocument4 pagesTherese Ronamae Loquez2 - Patient Drug DatabaseRonamaeNo ratings yet
- Multiple Associated Anomalies in Patients of Duodenal Atresia: A Case SeriesDocument2 pagesMultiple Associated Anomalies in Patients of Duodenal Atresia: A Case SeriesMuhammad Bilal MirzaNo ratings yet
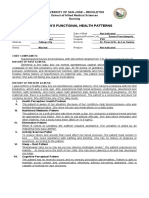
- Gordon'S Functional Health Patterns: University of San Jose - Recoletos School of Allied Medical Sciences NursingDocument2 pagesGordon'S Functional Health Patterns: University of San Jose - Recoletos School of Allied Medical Sciences NursingIvan A. EleginoNo ratings yet
- MBBS Pathology 3ed Semester Questions 2019-20Document11 pagesMBBS Pathology 3ed Semester Questions 2019-20RAJDEEP DASNo ratings yet
- Treatment of Hypernatremia in Adults - UpToDateDocument35 pagesTreatment of Hypernatremia in Adults - UpToDateJuLio Czar Carmona100% (1)
- T2R Survival Guide - 2019Document22 pagesT2R Survival Guide - 2019chioNo ratings yet