You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Godly Wisdom For A Pastor's Wife - Oyenike AreogunDocument131 pagesGodly Wisdom For A Pastor's Wife - Oyenike Areogunezekielekata100% (2)
- South Wales VocabDocument9 pagesSouth Wales VocabMario PuzoNo ratings yet
- Material Safety Data Sheet DynaplugDocument4 pagesMaterial Safety Data Sheet Dynaplugfs1640No ratings yet
- 28 Madrigal & Company, Inc. vs. Zamora, 151 SCRA 355, No. L-48237, No. L-49023 June 30, 1987Document11 pages28 Madrigal & Company, Inc. vs. Zamora, 151 SCRA 355, No. L-48237, No. L-49023 June 30, 1987Winnie Ann Lomosad-MisagalNo ratings yet
- Ni Crio User ManualDocument26 pagesNi Crio User ManualAntonio HerreraNo ratings yet
- Eurythmy: OriginDocument4 pagesEurythmy: OriginDananjaya PranandityaNo ratings yet
- Dissertation Proposal Sample Qualitative Robert MaldonadoDocument9 pagesDissertation Proposal Sample Qualitative Robert MaldonadoLim Soo H'anNo ratings yet
- ÔN TẬP ĐỘNG TỪ KHUYẾT THIẾU VÀ THÌ HTHT QKĐDocument19 pagesÔN TẬP ĐỘNG TỪ KHUYẾT THIẾU VÀ THÌ HTHT QKĐPham TinaNo ratings yet
- Incremental Analysis Week 5 Test Acc 561Document22 pagesIncremental Analysis Week 5 Test Acc 561WodroNo ratings yet
- CREDIT SAMPLEX (Midterms) 1) in Republic v. Jose Bagtas, Is Liable For The Loss of The Even Due To Fortuitous Event Because ofDocument3 pagesCREDIT SAMPLEX (Midterms) 1) in Republic v. Jose Bagtas, Is Liable For The Loss of The Even Due To Fortuitous Event Because ofRachel AndreleeNo ratings yet
- Renner - McDonald Complaint (FILED)Document16 pagesRenner - McDonald Complaint (FILED)jhbryanNo ratings yet
- Safety Data Sheet: Trade Name: Töten Bakterien Page 1/2Document2 pagesSafety Data Sheet: Trade Name: Töten Bakterien Page 1/2Muhammad Ahmed Abd ElmonemNo ratings yet
- G 342 Engine Part 1 PDFDocument26 pagesG 342 Engine Part 1 PDFharley florezNo ratings yet
- General Agreement On Tariffs and TradeDocument5 pagesGeneral Agreement On Tariffs and TradeOliver TalipNo ratings yet
- Diabetes Management ChecklistDocument2 pagesDiabetes Management ChecklistDianne100% (1)
- Paradise Lost (1667)Document29 pagesParadise Lost (1667)zephghosh100% (1)
- Joint University Programmes Admissions SystemDocument2 pagesJoint University Programmes Admissions SystemhoNo ratings yet
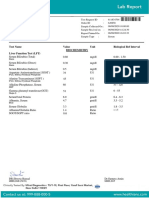
- Test Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Document7 pagesTest Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Himanshu GarkhelNo ratings yet
- Logic 2Document5 pagesLogic 2Bao TrungNo ratings yet
- Basic Taxation - CAVSU - Teaching Demo - Feb 5, 2018Document30 pagesBasic Taxation - CAVSU - Teaching Demo - Feb 5, 2018Renalyn ParasNo ratings yet
- Project Report Vignesh 2Document42 pagesProject Report Vignesh 2Raji rajiNo ratings yet
- The Problem of Partnership Business in NigeriaDocument7 pagesThe Problem of Partnership Business in NigeriarochaNo ratings yet
- VT525 SpecDocument2 pagesVT525 SpecTeo ZeniosNo ratings yet
- كورس بداية اعدادىDocument29 pagesكورس بداية اعدادىAhmed El-BadyNo ratings yet
- If The World Was Ending ChordsDocument4 pagesIf The World Was Ending Chordscookies100% (2)
- Reading For General PurposesDocument5 pagesReading For General PurposesMisykatul JannahNo ratings yet
- CS AssignmentDocument11 pagesCS AssignmentSudharaka SanjeewaNo ratings yet
- Calculating The Mean, Median, Mode and Range For Simple DataDocument2 pagesCalculating The Mean, Median, Mode and Range For Simple DataAnonymous hYMWbANo ratings yet
- Research Instruments Reading Comprehension InstrumentDocument14 pagesResearch Instruments Reading Comprehension InstrumentVirgi MarlanyNo ratings yet
- Bol EnglishDocument12 pagesBol EnglishKarina CorrosNo ratings yet