You might also like
- Basic Principles of Obturator Design For Partially Edentulous Patients. Part I: ClassificationDocument69 pagesBasic Principles of Obturator Design For Partially Edentulous Patients. Part I: ClassificationDrFarha NazNo ratings yet
- A Clinical Pathway For Complete Immediate Denture TherapyDocument18 pagesA Clinical Pathway For Complete Immediate Denture TherapyPragya PandeyNo ratings yet
- ResearchDocument26 pagesResearchJhen de Vera83% (12)
- Ansi A10.42Document23 pagesAnsi A10.42pedro la rosa100% (1)
- The Art of Threads A Comprehensive ReviewDocument17 pagesThe Art of Threads A Comprehensive Reviewalejandro Gonzàlez80% (5)
- Benefits of RPD: Elements and Compromised Function. The Removal of Exostoses and Tori Is Not A Complex ProcedureDocument8 pagesBenefits of RPD: Elements and Compromised Function. The Removal of Exostoses and Tori Is Not A Complex ProcedureSonia LeeNo ratings yet
- 3 Integratin Treatment Procedures in Occluso-RehabilitationDocument18 pages3 Integratin Treatment Procedures in Occluso-RehabilitationgabrielaNo ratings yet
- Mouth Prep VikasDocument35 pagesMouth Prep VikasVikas AggarwalNo ratings yet
- محاضة رقم 4Document8 pagesمحاضة رقم 4ابو الجودNo ratings yet
- Full Crown ModuleDocument16 pagesFull Crown ModuleDragos 1No ratings yet
- Preparation of Mouth For Removable Partial DenturesDocument47 pagesPreparation of Mouth For Removable Partial DenturesSeena Sam100% (2)
- 6.preprosthetic Surgery A Review of LiteratureDocument7 pages6.preprosthetic Surgery A Review of Literaturemirah indrianiNo ratings yet
- Immediate DenturesDocument35 pagesImmediate DenturesSimran SahniNo ratings yet
- 10 1111@jerd 12466Document4 pages10 1111@jerd 12466NémethBálintNo ratings yet
- Crown & Bridge or Fixed Prosthodontics Lectures - Level - 3Document4 pagesCrown & Bridge or Fixed Prosthodontics Lectures - Level - 3ruchikaNo ratings yet
- 1457792866immediate DenturesDocument5 pages1457792866immediate DenturesegarochmawatiNo ratings yet
- Klasifikasi AramanyDocument7 pagesKlasifikasi AramanyThio ZhuNo ratings yet
- A To Z Orthodontics Vol 20 SurgicalDocument23 pagesA To Z Orthodontics Vol 20 Surgicalshruti premsagarNo ratings yet
- Basic Principles of Obturator Design IIDocument7 pagesBasic Principles of Obturator Design IIGilberto Arturo Huapaya MarcosNo ratings yet
- Mouth Preparation in RPDDocument14 pagesMouth Preparation in RPDDr. Mangala Jyothi KJNo ratings yet
- Ecde 10 00327Document8 pagesEcde 10 00327Erisa BllakajNo ratings yet
- ObturatorsDocument79 pagesObturatorsPremshith CpNo ratings yet
- Perio 2005 PresentationDocument115 pagesPerio 2005 Presentationraiesa hashemNo ratings yet
- Full Mouth RehabDocument37 pagesFull Mouth RehabAravind Krishnan100% (4)
- Complications of Teeth ExtractionDocument13 pagesComplications of Teeth Extractionfbbqbcht6yNo ratings yet
- Insersi Instruksi Evaluasi GTL Presentasi DRG - HelmiDocument37 pagesInsersi Instruksi Evaluasi GTL Presentasi DRG - HelmigilangNo ratings yet
- Complications of Teeth ExtractionDocument13 pagesComplications of Teeth Extractionit's EimyNo ratings yet
- OverdentureDocument76 pagesOverdentureRaj Sha80% (5)
- Fixed-Removable Prostheses: Done By: Tabark Y. MizilDocument28 pagesFixed-Removable Prostheses: Done By: Tabark Y. MizilMustafa AhmedhamdiNo ratings yet
- Orthodontic Preparation For Orthognathic PDFDocument14 pagesOrthodontic Preparation For Orthognathic PDFbubuvulpeaNo ratings yet
- Scopus 1Document5 pagesScopus 1Shinta rahma MansyurNo ratings yet
- 6,7,8,9Document131 pages6,7,8,9Karaz StudiosNo ratings yet
- Klasifikasi AramanyDocument7 pagesKlasifikasi AramanyErwin SutonoNo ratings yet
- Fundamentals of Cavity PreparationDocument76 pagesFundamentals of Cavity Preparationragakodali0% (1)
- Provisional Restorations (Part 1) : ClinicalDocument5 pagesProvisional Restorations (Part 1) : ClinicalsuareztepperNo ratings yet
- JOHCD-Maintenance of Implant SupportedDocument3 pagesJOHCD-Maintenance of Implant SupportedManoj HumagainNo ratings yet
- Fundamentals of Tooth PreparationDocument50 pagesFundamentals of Tooth Preparationمعاذ نوري محمدNo ratings yet
- Maintenance of Gingival Form Following Implant PlacementDocument4 pagesMaintenance of Gingival Form Following Implant PlacementRomina BitaNo ratings yet
- Bedrossian Treatment Planning The Maxilla PDFDocument11 pagesBedrossian Treatment Planning The Maxilla PDFSitiKhadijahNo ratings yet
- 2018 Admixed TechDocument3 pages2018 Admixed TechBrijesh MaskeyNo ratings yet
- Band and Pontic: A Modified Band and Loop Space Maintainer - Clinical InnovationDocument3 pagesBand and Pontic: A Modified Band and Loop Space Maintainer - Clinical InnovationIJAR JOURNALNo ratings yet
- The Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFDocument7 pagesThe Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFAhmed Mohammed Saaduddin SapriNo ratings yet
- Try in and Maintenance in RPDDocument4 pagesTry in and Maintenance in RPDDr. Mangala Jyothi KJNo ratings yet
- Enhancement of Orthodontic Anchoring by The Use of Bone Anchorage A Case ReportDocument6 pagesEnhancement of Orthodontic Anchoring by The Use of Bone Anchorage A Case ReportAthenaeum Scientific PublishersNo ratings yet
- Complete Rehabilitation of A Patient With Occlusal Wear PDFDocument7 pagesComplete Rehabilitation of A Patient With Occlusal Wear PDFsarfarazahmad19No ratings yet
- Supplement The Base To Complement The Crown: Localized Ridge Augmentation Using Connective Tissue GraftDocument5 pagesSupplement The Base To Complement The Crown: Localized Ridge Augmentation Using Connective Tissue GraftBianca DimofteNo ratings yet
- CHAPTER 13 - Preparation of The Mouth For R - 2011 - McCracken S Removable Parti PDFDocument20 pagesCHAPTER 13 - Preparation of The Mouth For R - 2011 - McCracken S Removable Parti PDFFlorin Razvan CurcăNo ratings yet
- Interceptive Orthodontics-A Short Review: April 2011Document5 pagesInterceptive Orthodontics-A Short Review: April 2011Vijay ChinthaNo ratings yet
- Mouth PreparationDocument64 pagesMouth Preparationsamar yousif mohamedNo ratings yet
- Definitive Obturator Modified For Crown - PPTX DR AmrDocument49 pagesDefinitive Obturator Modified For Crown - PPTX DR AmrHatem Ibrahim Ahmed AburiaNo ratings yet
- Practice: Surgical Guidelines For Dental Implant PlacementDocument14 pagesPractice: Surgical Guidelines For Dental Implant PlacementAna94No ratings yet
- 7 Complications of Tooth Extraction PDFDocument10 pages7 Complications of Tooth Extraction PDFlyli Star AngeloNo ratings yet
- Immediate Denture: Advantages of Immediate DenturesDocument6 pagesImmediate Denture: Advantages of Immediate Denturesابراهيم منعم حسينNo ratings yet
- Factors Associated With Post Core Correction of Malpositioned TeethDocument3 pagesFactors Associated With Post Core Correction of Malpositioned TeethM Ghazy FajruyumaNo ratings yet
- Preprosthetic Surgery MADE EASYDocument14 pagesPreprosthetic Surgery MADE EASYMohammedNo ratings yet
- Immediate Dentures - 2Document18 pagesImmediate Dentures - 2Ayad IbrahimNo ratings yet
- Surgical Exposure and Fix Orthondontic Combination For Maxilla Canine Impacted TreatmentDocument5 pagesSurgical Exposure and Fix Orthondontic Combination For Maxilla Canine Impacted TreatmentRAKERNAS PDGI XINo ratings yet
- IRA Klein,: Mmedmte Denture ServiceDocument11 pagesIRA Klein,: Mmedmte Denture ServiceClaudia AngNo ratings yet
- 6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothDocument6 pages6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothSahana RangarajanNo ratings yet
- Preventive and Interceptive Orthodontics (Basic)Document49 pagesPreventive and Interceptive Orthodontics (Basic)Kamal Shanto100% (1)
- Treatment Planning Single Maxillary Anterior Implants for DentistsFrom EverandTreatment Planning Single Maxillary Anterior Implants for DentistsNo ratings yet
- Interceptive Orthodontics: A Practical Guide to Occlusal ManagementFrom EverandInterceptive Orthodontics: A Practical Guide to Occlusal ManagementNo ratings yet
- Osmf 521Document131 pagesOsmf 521Mohamed KilaniNo ratings yet
- Imp 521Document149 pagesImp 521Mohamed KilaniNo ratings yet
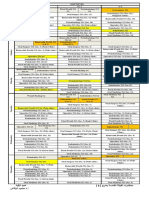
- جدول الفرقة الخامسة خريف 2022Document2 pagesجدول الفرقة الخامسة خريف 2022Mohamed KilaniNo ratings yet
- Rprosd 521Document130 pagesRprosd 521Mohamed KilaniNo ratings yet
- Perio 521Document181 pagesPerio 521Mohamed KilaniNo ratings yet
- Pedo 521Document160 pagesPedo 521Mohamed KilaniNo ratings yet
- Suturing TechniquesDocument2 pagesSuturing TechniquesMohamed KilaniNo ratings yet
- Management of Non-Carious LesionsDocument22 pagesManagement of Non-Carious LesionsMohamed KilaniNo ratings yet
- INDEX of CLINICAL PARTIAL DENTURE BOOKDocument1 pageINDEX of CLINICAL PARTIAL DENTURE BOOKMohamed KilaniNo ratings yet
- Hall Technique: DefinitionDocument6 pagesHall Technique: DefinitionMohamed KilaniNo ratings yet
- Clinical RPD Book CoverDocument1 pageClinical RPD Book CoverMohamed KilaniNo ratings yet
- Chapter 2 Primary ImpressionDocument8 pagesChapter 2 Primary ImpressionMohamed Kilani100% (1)
- Chapter 5 Metal TRY IN OF RPDDocument10 pagesChapter 5 Metal TRY IN OF RPDMohamed KilaniNo ratings yet
- Chapter 1 DiagnosisDocument32 pagesChapter 1 DiagnosisMohamed KilaniNo ratings yet
- Medical Declaration Form - Less Than 50 - EnglishDocument1 pageMedical Declaration Form - Less Than 50 - EnglishMohammed GeoffreyNo ratings yet
- Temporomandibular Disorders: A Term Whose Time Has Passed!: PerspectivesDocument2 pagesTemporomandibular Disorders: A Term Whose Time Has Passed!: PerspectivesUmer HussainNo ratings yet
- Pediatric Rehabilitation ServicesDocument10 pagesPediatric Rehabilitation ServicesRiris NariswariNo ratings yet
- Upma Recipe 3 Ways - Sooji Upma - Rava Upma - Uppittu Recipe - Hebbar's KitchenDocument3 pagesUpma Recipe 3 Ways - Sooji Upma - Rava Upma - Uppittu Recipe - Hebbar's KitchenbkNo ratings yet
- Tangina Mo BizarDocument1 pageTangina Mo BizarJhon eric EscultorNo ratings yet
- District DataDocument242 pagesDistrict Dataayush.bullethealthcareNo ratings yet
- Hiv Aids Laka Engtin Nge Kan Him Ang - Nuho TanDocument7 pagesHiv Aids Laka Engtin Nge Kan Him Ang - Nuho TanachungaNo ratings yet
- 10 Besar Penyakit RJ 2019Document10 pages10 Besar Penyakit RJ 2019afid kurniawanNo ratings yet
- Neonatal Antiepileptic Medication Treatment Patterns A Decade of ChangeDocument8 pagesNeonatal Antiepileptic Medication Treatment Patterns A Decade of ChangeEduardo Rios DuboisNo ratings yet
- Umid Final Booklet - (Selva)Document64 pagesUmid Final Booklet - (Selva)Jitendra Singh0% (1)
- Summary Report For:: 29-1131.00 - VeterinariansDocument6 pagesSummary Report For:: 29-1131.00 - Veterinariansapi-266289406No ratings yet
- Special Level 1Document12 pagesSpecial Level 1Aye Tube100% (2)
- CaO MSDS Cheney - LimeDocument6 pagesCaO MSDS Cheney - LimearmandogavinoNo ratings yet
- Insurance Japan Long TermDocument9 pagesInsurance Japan Long TermutisariNo ratings yet
- 5440 PU66 8H PU Topcoat Gloss - 3 - 20 (Ficha Técnica Pintura)Document6 pages5440 PU66 8H PU Topcoat Gloss - 3 - 20 (Ficha Técnica Pintura)Rubén AviationGroupNo ratings yet
- Brick Work JSA HSE ProfessionalsDocument1 pageBrick Work JSA HSE ProfessionalsStansilous Tatenda NyagomoNo ratings yet
- TESDA-SOP-TSDO-01-F05 (List of Consumables)Document1 pageTESDA-SOP-TSDO-01-F05 (List of Consumables)라영민No ratings yet
- Nonlinear PharmacokineticsDocument22 pagesNonlinear PharmacokineticsNadya Prafita100% (1)
- Exploratory Factor Analysis For Indonesian Version of PID-5Document1 pageExploratory Factor Analysis For Indonesian Version of PID-5DharmaNo ratings yet
- HR BipartitismDocument18 pagesHR BipartitismrobingehlotNo ratings yet
- Dr. Ma. Florecilla C. Cinches Dr. Teresita T. TumaponDocument5 pagesDr. Ma. Florecilla C. Cinches Dr. Teresita T. TumaponTim ArroyoNo ratings yet
- CHOLElithiasisDocument93 pagesCHOLElithiasisfranciscomaricris13No ratings yet
- Vendor ManualDocument19 pagesVendor Manualvinurules20No ratings yet
- Biologic Agents To Optimize Outcomes Following ACL Repair and Reconstruction A Systematic Review of Clinical EvidenceDocument38 pagesBiologic Agents To Optimize Outcomes Following ACL Repair and Reconstruction A Systematic Review of Clinical EvidenceyasimNo ratings yet
- Occuper's Liability (Textbook + Lecture Notes)Document28 pagesOccuper's Liability (Textbook + Lecture Notes)Malvika MahindraNo ratings yet
- Counseling For Behavior Change: F. Daniel Duffy, MD, MACP Michael G. Goldstein, MDDocument28 pagesCounseling For Behavior Change: F. Daniel Duffy, MD, MACP Michael G. Goldstein, MDKodhandaiah Nesanuru NNo ratings yet
- LifebuoyDocument10 pagesLifebuoyPrateek Gupta100% (1)