You might also like
- Pharmacotherapeutic Management of Cardiovascular Disease Complications: A Textbook for Medical StudentsFrom EverandPharmacotherapeutic Management of Cardiovascular Disease Complications: A Textbook for Medical StudentsNo ratings yet
- 3 ❤ Smart Sheet for History Taking in Pediatrics خلفية صفراءDocument14 pages3 ❤ Smart Sheet for History Taking in Pediatrics خلفية صفراءsalah almozahemNo ratings yet
- IRMA Pediatric Palliative CommunicationDocument40 pagesIRMA Pediatric Palliative CommunicationHelmi IrmawantyNo ratings yet
- Case-Based Pace, ICDs, and CRT Volume 1Document234 pagesCase-Based Pace, ICDs, and CRT Volume 1oxequlalisNo ratings yet
- Diabetes - Clinicians Desk Reference PDFDocument209 pagesDiabetes - Clinicians Desk Reference PDFCarmen UngureanuNo ratings yet
- Diffi Cult To Treat Asthma: Sandhya Khurana Fernando Holguin EditorsDocument339 pagesDiffi Cult To Treat Asthma: Sandhya Khurana Fernando Holguin Editorsneumologia.intervencionNo ratings yet
- Allowing Spirituality Into The Healing Process: Original ResearchDocument9 pagesAllowing Spirituality Into The Healing Process: Original ResearchAmanda DavisNo ratings yet
- Essentials of Internal MedicineDocument832 pagesEssentials of Internal MedicineHtet Kyaw KyawNo ratings yet
- Acute Pancreatitis: in The ClinicDocument16 pagesAcute Pancreatitis: in The ClinicdeltanueveNo ratings yet
- Copc LectureDocument36 pagesCopc LectureRoger Jr BrazilNo ratings yet
- Internal MedicineDocument161 pagesInternal Medicinemain.genevive.diligNo ratings yet
- Diabetes and Complications: When Documenting Diabetes, It's Important To Note The FollowingDocument2 pagesDiabetes and Complications: When Documenting Diabetes, It's Important To Note The Followingmeikaizen100% (1)
- JNC 8Document40 pagesJNC 8Nadira Wulandari100% (1)
- Febrile Neutropenia Care GuidelineDocument2 pagesFebrile Neutropenia Care GuidelinedenokayuMRNo ratings yet
- Hipercalcemia JamaDocument13 pagesHipercalcemia JamaSebastián Camilo Duque100% (1)
- UntitledDocument301 pagesUntitledS.R.GNo ratings yet
- Part C: Questions and Answers Regarding Assessing The Appropriateness and Effectiveness of Methadone Maintenance TreatmentDocument5 pagesPart C: Questions and Answers Regarding Assessing The Appropriateness and Effectiveness of Methadone Maintenance TreatmentYogesh ShindeNo ratings yet
- Fibromyalgia A Clinical ReviewDocument9 pagesFibromyalgia A Clinical ReviewastrogliaNo ratings yet
- Fibromyalgia Fam Resilience PDFDocument19 pagesFibromyalgia Fam Resilience PDFirimes carmelaNo ratings yet
- History and Physical Exam TemplateDocument3 pagesHistory and Physical Exam TemplatederekcftamNo ratings yet
- (Ruth Ballweg, MPA, PA-C, Edward M. Sullivan, MS, (B-Ok - Xyz) PDFDocument939 pages(Ruth Ballweg, MPA, PA-C, Edward M. Sullivan, MS, (B-Ok - Xyz) PDFJim Velasquez100% (1)
- H&P GuideDocument7 pagesH&P GuideTBWPNo ratings yet
- Cardiology IDocument112 pagesCardiology IAhmad Makhlouf100% (1)
- Treatment of Resistant and Refractory HypertensionDocument21 pagesTreatment of Resistant and Refractory HypertensionLuis Rodriguez100% (1)
- HTA Europeo PDFDocument675 pagesHTA Europeo PDFFrancisco Javier Palma P100% (1)
- Acute Kidney InjuryDocument15 pagesAcute Kidney InjuryManish VijayNo ratings yet
- The Management of Common and Selected Psychiatric EmergenciesDocument129 pagesThe Management of Common and Selected Psychiatric EmergenciesHasaan Khan100% (1)
- Protocol - IM DyspneaDocument7 pagesProtocol - IM DyspneaTrisNo ratings yet
- Kasabach Merritt SyndromeDocument33 pagesKasabach Merritt SyndromeAndrew Arnold David VillanuevaNo ratings yet
- DR - Muhammad Aasam Maan: Consultant Pain SpecialistDocument23 pagesDR - Muhammad Aasam Maan: Consultant Pain SpecialistMuhammad Aasim MaanNo ratings yet
- Family Medicine Family CaseDocument17 pagesFamily Medicine Family Casecorina_oliverNo ratings yet
- The PFC MatrixDocument1 pageThe PFC MatrixAd AstraNo ratings yet
- Adolescent Health Care PDFDocument729 pagesAdolescent Health Care PDFAlain BriseñoNo ratings yet
- Benedict M. Glover (Editor), Pedro Brugada (Editor) - Clinical Handbook of Cardiac Electrophysiology-Springer Nature (2021)Document230 pagesBenedict M. Glover (Editor), Pedro Brugada (Editor) - Clinical Handbook of Cardiac Electrophysiology-Springer Nature (2021)Gabriel CruzNo ratings yet
- Anemia Prevention and Management Program Implementation GuideDocument60 pagesAnemia Prevention and Management Program Implementation GuideIchlasul MadriddistaNo ratings yet
- Diabetes Medication SummaryDocument1 pageDiabetes Medication Summarywoody_2512No ratings yet
- Pediatric Pharmacology: Dr. Putrya Hawa, M.Biomed Faculty of Medicine, UIIDocument27 pagesPediatric Pharmacology: Dr. Putrya Hawa, M.Biomed Faculty of Medicine, UIIAfied Fitrah100% (1)
- Fact Sheet On HypertensionDocument1 pageFact Sheet On HypertensionMichael Vance Boctot100% (1)
- QA PAFP Journal July December 59-2-2021 Pages 115 126Document12 pagesQA PAFP Journal July December 59-2-2021 Pages 115 126Norjetalexis Maningo CabreraNo ratings yet
- Hypertensive Emergencies in The Emergency DepartmentDocument13 pagesHypertensive Emergencies in The Emergency DepartmentLuis Lopez RevelesNo ratings yet
- 000-Intro To Internal MedicineDocument6 pages000-Intro To Internal MedicineRizky KykyNo ratings yet
- Aki 2018Document45 pagesAki 2018NURUL ROMADHONNo ratings yet
- Powell 2022 Oi 221002 1664506604.73378Document12 pagesPowell 2022 Oi 221002 1664506604.73378AntoineNo ratings yet
- CVA Case PresentationDocument16 pagesCVA Case PresentationgolokipokNo ratings yet
- CV Tao JocelynDocument5 pagesCV Tao Jocelynapi-534834771No ratings yet
- PDFDocument70 pagesPDFPaul Benjomin AgregadoNo ratings yet
- Pediatrics 2 LaboratoryDocument40 pagesPediatrics 2 LaboratoryAmaetenNo ratings yet
- DM Egregious ElevenDocument18 pagesDM Egregious ElevendavidtuanandartuaNo ratings yet
- Professional ResumeDocument1 pageProfessional ResumeDouglas RutledgeNo ratings yet
- 01-09 2022 Pharm Chronic Care in Cardiology 2022 R4Document62 pages01-09 2022 Pharm Chronic Care in Cardiology 2022 R4Amira HelayelNo ratings yet
- Oxford Psychiatry Library David Nutt David Castle Psychedelics As Psychiatric Medications Oxford UDocument180 pagesOxford Psychiatry Library David Nutt David Castle Psychedelics As Psychiatric Medications Oxford URosa Elena Marquez ANo ratings yet
- HistoryandPhysicalExamDocument105 pagesHistoryandPhysicalExamsilentscream0618No ratings yet
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Tuberculous Meningitis: Manual of Diagnosis and TherapyFrom EverandTuberculous Meningitis: Manual of Diagnosis and TherapyJerome ChinNo ratings yet
- Evidence-Based Infectious DiseasesFrom EverandEvidence-Based Infectious DiseasesDominik MertzNo ratings yet
- Advances in Cattle WelfareFrom EverandAdvances in Cattle WelfareCassandra TuckerNo ratings yet
- A Concept-Based Approach To Learning: DevelopmentDocument62 pagesA Concept-Based Approach To Learning: DevelopmentAli Nawaz AyubiNo ratings yet
- Case Study of Bronchial Asthma in Acute ExacerbationDocument16 pagesCase Study of Bronchial Asthma in Acute Exacerbationdextroid1290% (29)
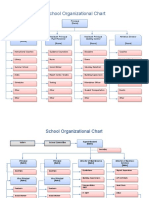
- School Organizational ChartDocument4 pagesSchool Organizational ChartislahNo ratings yet
- The Cambridge Handbook of Clinical Assessment and Diagnosis (2019)Document534 pagesThe Cambridge Handbook of Clinical Assessment and Diagnosis (2019)Ofelia Kerr100% (4)
- Graded RecitationDocument22 pagesGraded RecitationClara MaeNo ratings yet
- Growing Uganda's mushroom farming industryDocument2 pagesGrowing Uganda's mushroom farming industrymaboni ismaelNo ratings yet
- A Case Study On Occupational Health and Safety of Footwear Manufacturing IndustryDocument6 pagesA Case Study On Occupational Health and Safety of Footwear Manufacturing IndustryZakir KhanNo ratings yet
- Launching of The Internet-Based Education ProgramDocument6 pagesLaunching of The Internet-Based Education ProgramaminoacidNo ratings yet
- Being in The World Selected Pa Ludwig BinswangerDocument388 pagesBeing in The World Selected Pa Ludwig BinswangerRamazan ÇarkıNo ratings yet
- Coulter Slidemaking - Service ManualDocument443 pagesCoulter Slidemaking - Service ManualIoana BeteaNo ratings yet
- Sex Education Literacy Stem 11 A.Document54 pagesSex Education Literacy Stem 11 A.Bangtan SeonyeondanNo ratings yet
- Audiometer Impedqnce Audiometer AT235 - USER - MANUALDocument103 pagesAudiometer Impedqnce Audiometer AT235 - USER - MANUALKafina Multi SejahteraNo ratings yet
- EpidemiologyDocument100 pagesEpidemiologyKailash NagarNo ratings yet
- Pediatric Cardiology II Lecture SummaryDocument5 pagesPediatric Cardiology II Lecture SummaryMedisina101No ratings yet
- Participants List DDO's and Their Staff 25Document3 pagesParticipants List DDO's and Their Staff 25Manoj Digi LoansNo ratings yet
- Openhrt 2021 001732Document9 pagesOpenhrt 2021 001732benypermadiNo ratings yet
- COMPENSATION Class 1 PDFDocument5 pagesCOMPENSATION Class 1 PDFpsicologothNo ratings yet
- Drug Law Seminar PaperDocument70 pagesDrug Law Seminar PaperBapulNo ratings yet
- Project On-Law of Torts Topic - NegligenceDocument10 pagesProject On-Law of Torts Topic - NegligenceSoumya Shefali ChandrakarNo ratings yet
- Yds Kelime Bilgisi TestiDocument3 pagesYds Kelime Bilgisi TestiMehmet CELİKNo ratings yet
- Updated Format SynopsisDocument13 pagesUpdated Format Synopsissiboyif881No ratings yet
- ML SyllDocument2 pagesML Syllmurlak37No ratings yet
- An Analysis of The Mercury Content of The Water and Life Forms in Manila Bay (Cavite Area)Document24 pagesAn Analysis of The Mercury Content of The Water and Life Forms in Manila Bay (Cavite Area)Jesse Nicole SantosNo ratings yet
- Mikkelsen 2017 Diários em Crianças Estudo QualitativoDocument6 pagesMikkelsen 2017 Diários em Crianças Estudo QualitativoGabriela LealNo ratings yet
- Cardiac ArrestDocument50 pagesCardiac ArrestAnju Radhika100% (1)
- Writing Sample 2Document9 pagesWriting Sample 2api-582848179No ratings yet
- RFP 23-031 Electronic & Physical Site SecurityDocument31 pagesRFP 23-031 Electronic & Physical Site SecurityElle PolonNo ratings yet
- Talent Management SystemDocument22 pagesTalent Management SystemDeepa Yadav100% (1)
- Prof Prac 2 EssayDocument3 pagesProf Prac 2 EssayEryka DyenghongNo ratings yet
- Sodium Bicarbonate: PresentationDocument3 pagesSodium Bicarbonate: Presentationmadimadi11No ratings yet