You might also like
- Ettinger Small Animal Internal Medicine PDFDocument2 pagesEttinger Small Animal Internal Medicine PDFRod0% (8)
- Legislator Email on Safe Patient HandlingDocument5 pagesLegislator Email on Safe Patient HandlingAnonymous dcpGmD60% (5)
- Pressure SoreDocument3 pagesPressure SoreGhadaNo ratings yet
- Paper 1 Mets Among HD PatientsDocument10 pagesPaper 1 Mets Among HD PatientsRicky VirnardoNo ratings yet
- The Effectiveness Diabetic Foot Spa To Peripheral Blood Circulation of DM Type 2 Patient in Puskesmas Wonokromo Surabaya Puji AstutiDocument9 pagesThe Effectiveness Diabetic Foot Spa To Peripheral Blood Circulation of DM Type 2 Patient in Puskesmas Wonokromo Surabaya Puji AstutiAngestidyahNo ratings yet
- Hepatic Steatosis DyslipidemiaDocument6 pagesHepatic Steatosis Dyslipidemiakarina nilasariNo ratings yet
- Quality of Life Patients With Ulcus DiabeticDocument4 pagesQuality of Life Patients With Ulcus DiabeticNadiaRashyaNo ratings yet
- Risk Factor of Cardiovascular Disease Among Older IndividualsDocument4 pagesRisk Factor of Cardiovascular Disease Among Older IndividualsAreej ErhimaNo ratings yet
- Global Epidemiology of Diabetic Foot Ulceration A Systematic Review and Meta AnalysisDocument12 pagesGlobal Epidemiology of Diabetic Foot Ulceration A Systematic Review and Meta AnalysisTri Jaya RetnaNo ratings yet
- Tugas Mini Riset LengkapDocument10 pagesTugas Mini Riset LengkapJerry FahrainNo ratings yet
- Diabetic Foot Risk Factors in Type 2 Diabetes Patients: A Cross-Sectional Case Control StudyDocument5 pagesDiabetic Foot Risk Factors in Type 2 Diabetes Patients: A Cross-Sectional Case Control Studychintya claraNo ratings yet
- Proceedings of The 5th Annual International Conference Syiah Kuala University (AIC Unsyiah) 2015Document6 pagesProceedings of The 5th Annual International Conference Syiah Kuala University (AIC Unsyiah) 2015Mutiara Khaerun NisaNo ratings yet
- Schizophrenia Research: ArticleinfoDocument5 pagesSchizophrenia Research: ArticleinfojhuNo ratings yet
- Identificar PAD en Pacientes Con Pie DiabeticoDocument12 pagesIdentificar PAD en Pacientes Con Pie DiabeticoSamuel GarciaNo ratings yet
- Prevalence and Associated Factors of Diabetic Foot at Risk Among Type 2 Diabetes Mellitus Patients Attending Primary Health Clinics in KuantanDocument9 pagesPrevalence and Associated Factors of Diabetic Foot at Risk Among Type 2 Diabetes Mellitus Patients Attending Primary Health Clinics in Kuantanlailatul husnaNo ratings yet
- ANALISA FAKTOR RISIKO PENYEBAB KEJADIAN PENYAKIT GAGAL GINJAL KRONIK (GGK) DI RUANG HEMODIALISA RS Dr. MOEWARDIDocument13 pagesANALISA FAKTOR RISIKO PENYEBAB KEJADIAN PENYAKIT GAGAL GINJAL KRONIK (GGK) DI RUANG HEMODIALISA RS Dr. MOEWARDIPray PrihatiwiNo ratings yet
- 36-39 DevaDocument4 pages36-39 DevaEndhy KurniawanNo ratings yet
- Risk Factors Associated With Type 2 Diabetes Mellitus and The Frequency of Nafld Affected PatientsDocument5 pagesRisk Factors Associated With Type 2 Diabetes Mellitus and The Frequency of Nafld Affected PatientsIJAR JOURNALNo ratings yet
- Prevalence of Diabetes, Associated Symptoms and Risk Factors Among University StudentsDocument8 pagesPrevalence of Diabetes, Associated Symptoms and Risk Factors Among University Studentsijmb333No ratings yet
- Risk factors for lower extremity ulceration and amputation in diabetic patientsDocument10 pagesRisk factors for lower extremity ulceration and amputation in diabetic patientsEdemberg FreitasNo ratings yet
- Fu RongDocument9 pagesFu RongTín NguyễnNo ratings yet
- Burger Allen ExercisesDocument6 pagesBurger Allen Exerciseslucky 116No ratings yet
- Prevalence, Factors and Complication of Diabetes in An Underdeveloped Region of Khyber Pukhtun Khawa: A Cross-Sectional StudyDocument6 pagesPrevalence, Factors and Complication of Diabetes in An Underdeveloped Region of Khyber Pukhtun Khawa: A Cross-Sectional StudyOpenaccess Research paperNo ratings yet
- Is There A Relationship Between Periodontal Disease and Causes of Death? A Cross Sectional StudyDocument6 pagesIs There A Relationship Between Periodontal Disease and Causes of Death? A Cross Sectional StudyYaarit IustainNo ratings yet
- Platelet width as clue to diabetes complicationsDocument3 pagesPlatelet width as clue to diabetes complicationsDr. Asaad Mohammed Ahmed BabkerNo ratings yet
- A Case-Control Study of Salivary Redox Homeostasis in Hypertensive ChildrenDocument23 pagesA Case-Control Study of Salivary Redox Homeostasis in Hypertensive ChildrenfghdhmdkhNo ratings yet
- Faktor-Faktor Yang Mempengaruhi Penyembuhan Luka Gangrene Pada Penderita Diabetes Mellitus Di Ruang Rawat Inap Rsud Dr. Pirngadi MedanDocument5 pagesFaktor-Faktor Yang Mempengaruhi Penyembuhan Luka Gangrene Pada Penderita Diabetes Mellitus Di Ruang Rawat Inap Rsud Dr. Pirngadi MedanYUDINA ZEBUANo ratings yet
- Effect of Carambola Fruit Juice of Changes in Blood Pressure Patients With Hypertension in Nursing HomesDocument16 pagesEffect of Carambola Fruit Juice of Changes in Blood Pressure Patients With Hypertension in Nursing Homesmasukan nama100% (1)
- Prevalence and Major Risk Factors of Diabetic Retinopathy: A Cross-Sectional Study in EcuadorDocument5 pagesPrevalence and Major Risk Factors of Diabetic Retinopathy: A Cross-Sectional Study in EcuadorJorge Andres Talledo DelgadoNo ratings yet
- Knowledge and Practice Regarding Foot Care Among Patients With Type 2 Diabetes MellitusDocument6 pagesKnowledge and Practice Regarding Foot Care Among Patients With Type 2 Diabetes MellitusTJPRC PublicationsNo ratings yet
- Role of Diet in Hyperuricemia and GoutDocument14 pagesRole of Diet in Hyperuricemia and Goutemilianoarteagagarcia11No ratings yet
- Clinical Presentation and Outcome in Diabetic Foot Cases: A Prospective Study in A Tertiary Care Teaching Hospital of Uttarakhand, IndiaDocument4 pagesClinical Presentation and Outcome in Diabetic Foot Cases: A Prospective Study in A Tertiary Care Teaching Hospital of Uttarakhand, IndiaNaily Nuzulur RohmahNo ratings yet
- 2017 - Bansal - Corelation of HbA1c Levels and Duration of Diabetes With PADDocument4 pages2017 - Bansal - Corelation of HbA1c Levels and Duration of Diabetes With PADbuat nugas28No ratings yet
- 40 Iajps40102020Document4 pages40 Iajps40102020iajpsNo ratings yet
- de Boer JAMA 2011Document8 pagesde Boer JAMA 2011slavenNo ratings yet
- 2 PBDocument4 pages2 PBSuryati HusinNo ratings yet
- ,content, 31,2,361 FullDocument2 pages,content, 31,2,361 FullMilka MimingNo ratings yet
- Tresierra Ayala2017Document4 pagesTresierra Ayala2017latifaNo ratings yet
- HTTPDocument65 pagesHTTPAndreea SlabuNo ratings yet
- Peripheral Arterial Disease in Patients With Diabetes: State-Of-The-Art PaperDocument9 pagesPeripheral Arterial Disease in Patients With Diabetes: State-Of-The-Art PaperdonkeyendutNo ratings yet
- Congestion Cardiaca y PeriodontitisDocument7 pagesCongestion Cardiaca y Periodontitiscruzjulio480No ratings yet
- Admin, JUXTA 015 Ahmad FixDocument4 pagesAdmin, JUXTA 015 Ahmad FixBelli Zoel FiqriNo ratings yet
- DBT y Obs SarcopenicaDocument8 pagesDBT y Obs SarcopenicaestesiesundriveNo ratings yet
- Thesis Protocol: DNB General MedicineDocument30 pagesThesis Protocol: DNB General Medicinegattu santoshNo ratings yet
- Association Between Psoriasis and The Metabolic Syndrome: Short CommunicationDocument5 pagesAssociation Between Psoriasis and The Metabolic Syndrome: Short CommunicationketlyneNo ratings yet
- GoutDocument17 pagesGoutnadita erischaNo ratings yet
- 271 2118 1 PBDocument6 pages271 2118 1 PByketamNo ratings yet
- Pengaruh Rendam Kaki Dengan Air Hangat Terhadap Penurunan Tekanan Darah Pada Penderita Hipertensi Di Kelurahan Timbangan Tahun 2017 Nanda Masraini Daulay, Febrina Angraini SimamoraDocument9 pagesPengaruh Rendam Kaki Dengan Air Hangat Terhadap Penurunan Tekanan Darah Pada Penderita Hipertensi Di Kelurahan Timbangan Tahun 2017 Nanda Masraini Daulay, Febrina Angraini Simamoratia suhadaNo ratings yet
- Senam Prolanis Menurunkan Tekanan Darah Lansia Penderita HipertensiDocument10 pagesSenam Prolanis Menurunkan Tekanan Darah Lansia Penderita HipertensiilhamNo ratings yet
- Nutrition and Vascular DementiaDocument6 pagesNutrition and Vascular Dementiaapi-150223943No ratings yet
- Seminar: Ning Cheung, Paul Mitchell, Tien Yin WongDocument13 pagesSeminar: Ning Cheung, Paul Mitchell, Tien Yin WongChandrahas ReddyNo ratings yet
- Journal of Diabetes and Its Complications: Yiqun Chen, Frank A. Sloan, Arseniy P. YashkinDocument6 pagesJournal of Diabetes and Its Complications: Yiqun Chen, Frank A. Sloan, Arseniy P. YashkinrodrigoNo ratings yet
- Cystatin C As An Early Marker of Diabetic Nephropathy in Nigerian Adults With Type 2 DiabetesDocument9 pagesCystatin C As An Early Marker of Diabetic Nephropathy in Nigerian Adults With Type 2 Diabetesijmb333No ratings yet
- Metabolites 10 00195 v2Document11 pagesMetabolites 10 00195 v2Aulia lestariNo ratings yet
- Disparities in Periodontitis Prevalence Among Chronic Kidney Disease PatientsDocument5 pagesDisparities in Periodontitis Prevalence Among Chronic Kidney Disease PatientsKristelle HernandezNo ratings yet
- Paper13 PDFDocument6 pagesPaper13 PDFSekar MentariNo ratings yet
- Prediabetes: Why Should We Care?: Ashkan Zand, M.D. Karim Ibrahim, M.D. Bhargavi Patham, M.DDocument9 pagesPrediabetes: Why Should We Care?: Ashkan Zand, M.D. Karim Ibrahim, M.D. Bhargavi Patham, M.DCharlotte KeckhutNo ratings yet
- Younger Patients at Greater Risk of GERDDocument11 pagesYounger Patients at Greater Risk of GERDsahama2508No ratings yet
- Jurnal Berkala Epidemiologi: Hubungan Status Gizi Dan Lingkar Perut Dengan Kejadian Hipertensi Pada Usia LanjutDocument8 pagesJurnal Berkala Epidemiologi: Hubungan Status Gizi Dan Lingkar Perut Dengan Kejadian Hipertensi Pada Usia LanjutPasaribub3004No ratings yet
- Advpub JE20150123Document7 pagesAdvpub JE20150123Sherly KristiNo ratings yet
- Urinary Tract Stones Risk Factors in Patients With Benign Prostatic Hyperplasia in West Java, IndonesiaDocument6 pagesUrinary Tract Stones Risk Factors in Patients With Benign Prostatic Hyperplasia in West Java, IndonesiaS3V4_9154No ratings yet
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyFrom EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyRating: 1 out of 5 stars1/5 (1)
- Complementary and Alternative Medical Lab Testing Part 15: MusculoskeletalFrom EverandComplementary and Alternative Medical Lab Testing Part 15: MusculoskeletalNo ratings yet
- Epidemiology of COVID-19: Sudipta Dhar Chowdhury Anu Mary OommenDocument5 pagesEpidemiology of COVID-19: Sudipta Dhar Chowdhury Anu Mary Oommenagil ferdiansyahNo ratings yet
- Management of Maxillofacial Trauma in Emergency: An Update of Challenges and ControversiesDocument9 pagesManagement of Maxillofacial Trauma in Emergency: An Update of Challenges and ControversiesAdnan Basyar AdnaniNo ratings yet
- Risk Factors for Descending Necrotizing MediastinitisDocument3 pagesRisk Factors for Descending Necrotizing MediastinitisHusnul KhatimahNo ratings yet
- Streptococcal Tonsillitis As A Cause of Urticaria Tonsillitis and UrticariaDocument5 pagesStreptococcal Tonsillitis As A Cause of Urticaria Tonsillitis and Urticariaagil ferdiansyahNo ratings yet
- Ijma 9 408Document3 pagesIjma 9 408agil ferdiansyahNo ratings yet
- 13I - Cardiogenic Shock Caused by SARS-CoV-2 in A Patient With Serial Negative Nucleic Acid Amplification Tests Case ReportDocument3 pages13I - Cardiogenic Shock Caused by SARS-CoV-2 in A Patient With Serial Negative Nucleic Acid Amplification Tests Case Reportagil ferdiansyahNo ratings yet
- Jamacardiology Daniels 2021 Oi 210042 1631046558.86932Document10 pagesJamacardiology Daniels 2021 Oi 210042 1631046558.86932agil ferdiansyahNo ratings yet
- Fibula 7Document4 pagesFibula 7agil ferdiansyahNo ratings yet
- PIIS0923753419396838Document6 pagesPIIS0923753419396838agil ferdiansyahNo ratings yet
- Toward Nanotechnology-Enabled Approaches Against The COVID-19 PandemicDocument24 pagesToward Nanotechnology-Enabled Approaches Against The COVID-19 Pandemicmadcraft9832No ratings yet
- PelajaranDocument25 pagesPelajaranmarisa isahNo ratings yet
- RasproDocument63 pagesRasprofany hertinNo ratings yet
- Colostrum - How Does It Keep Health?Document9 pagesColostrum - How Does It Keep Health?JakirNo ratings yet
- Maxillary Molar Distalization With The Dual-ForceDocument5 pagesMaxillary Molar Distalization With The Dual-ForceMaria SilvaNo ratings yet
- Carpal Tunnel SyndromeDocument37 pagesCarpal Tunnel SyndromePramadya Vardhani MustafizaNo ratings yet
- Basic DefinitionDocument7 pagesBasic Definitionsamiurrehman4994No ratings yet
- Knowledge and Attitude of Maternity Nurses Regarding Cord Blood Collection and Stem Cells: An Educational InterventionDocument12 pagesKnowledge and Attitude of Maternity Nurses Regarding Cord Blood Collection and Stem Cells: An Educational InterventionSanjay Kumar SanjuNo ratings yet
- Sanofi, J&J, BoehringerDocument4 pagesSanofi, J&J, BoehringerBlazy InhumangNo ratings yet
- Hospital Management System UML and Specification DocumentDocument16 pagesHospital Management System UML and Specification DocumentManish PareekNo ratings yet
- Unofficial Guide To Practical SkillsDocument34 pagesUnofficial Guide To Practical SkillsFrancisco Javier Moraga Vásquez0% (1)
- Vaccine Guide - Randall NeustaedterDocument6 pagesVaccine Guide - Randall NeustaedterttreksNo ratings yet
- Excl.: Hydrosalpinx (N70.1) : of OvaryDocument9 pagesExcl.: Hydrosalpinx (N70.1) : of OvaryDaniel SusantoNo ratings yet
- Ncma217 Performancetask#5 TinioDocument7 pagesNcma217 Performancetask#5 TinioAndhee Mae TinioNo ratings yet
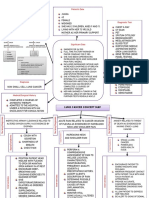
- Lung Cancer Concept Map-Group 2Document2 pagesLung Cancer Concept Map-Group 2Maria Cristina100% (2)
- Viral Hepatitis Atoe and MoreDocument31 pagesViral Hepatitis Atoe and MoreAnkita SamantaNo ratings yet
- Prevention of Waterborne DiseasesDocument2 pagesPrevention of Waterborne DiseasesRixin JamtshoNo ratings yet
- How to Prepare for the FCPS Part 1 Exam in ENTDocument4 pagesHow to Prepare for the FCPS Part 1 Exam in ENTDoodNo ratings yet
- Follicular Jaw CystsDocument6 pagesFollicular Jaw CystsMixelia Ade NoviantyNo ratings yet
- Change in HIV Window Period A Clinical PerspectiveDocument46 pagesChange in HIV Window Period A Clinical PerspectiveSvarogNo ratings yet
- Laya Allpmirules 040 1023Document48 pagesLaya Allpmirules 040 10238768263No ratings yet
- Walaa SNC Network List Mar 2021Document9 pagesWalaa SNC Network List Mar 2021ning yangNo ratings yet
- Schizophrenia Case StudyDocument14 pagesSchizophrenia Case Studyapi-593859653No ratings yet
- Abortion Law Policy and Services in India A Critical ReviewDocument9 pagesAbortion Law Policy and Services in India A Critical ReviewAhkam KhanNo ratings yet
- HIV and AIDS in Malawi Groups Most Affected by HIV in Malawi HIV Disproportionately Affects Women in Malawi PDFDocument14 pagesHIV and AIDS in Malawi Groups Most Affected by HIV in Malawi HIV Disproportionately Affects Women in Malawi PDFJames ChinamasaNo ratings yet
- Niple PainDocument13 pagesNiple PainPUPUT NUGRAHANo ratings yet
- Hippocrates EnglishDocument4 pagesHippocrates EnglishOtilia GuliiNo ratings yet