You might also like
- Syndrome of Inappropriate Vasopressin Sexretion (Siadh)Document22 pagesSyndrome of Inappropriate Vasopressin Sexretion (Siadh)Moni RethNo ratings yet
- Hyponatremia in DCLDDocument27 pagesHyponatremia in DCLDGowtham KrishnaNo ratings yet
- Disorders of Fluid ElectrolytesDocument31 pagesDisorders of Fluid ElectrolytesjabirNo ratings yet
- Electrolytedisturbances 111102083753 Phpapp02Document137 pagesElectrolytedisturbances 111102083753 Phpapp02bobbyfildianNo ratings yet
- Electrolyte ImbalanceDocument79 pagesElectrolyte Imbalancemarauder_popNo ratings yet
- Osmoregulation and Control of Icfv Lecture-IDocument50 pagesOsmoregulation and Control of Icfv Lecture-IfadhiliNo ratings yet
- Chapter 15: ElectrolytesDocument6 pagesChapter 15: ElectrolytesTelle AngNo ratings yet
- Gangguan Keseimbangan Cairan Dan ElektrolitDocument77 pagesGangguan Keseimbangan Cairan Dan ElektrolitPutri Santri100% (2)
- Tau Chempath Lecture - Fluid & Electrolyte BalanceDocument48 pagesTau Chempath Lecture - Fluid & Electrolyte BalanceJoshua KalundaNo ratings yet
- Disorders-Of-Sodium-Balance - CAMBRIDGEDocument10 pagesDisorders-Of-Sodium-Balance - CAMBRIDGEDenisa Carmen ColiofNo ratings yet
- Fluid & ElectrolyteDocument69 pagesFluid & ElectrolytePaul Ebenezer100% (1)
- Diagnosis and Management of Common Electrolyte DisordersDocument42 pagesDiagnosis and Management of Common Electrolyte DisorderspandeNo ratings yet
- ADH UpdatedDocument24 pagesADH UpdateddrgeetanshmittalNo ratings yet
- Diagnosis and Management of Common Electrolyte Disorders: Eric I. Rosenberg, MD, MSPH, FACPDocument44 pagesDiagnosis and Management of Common Electrolyte Disorders: Eric I. Rosenberg, MD, MSPH, FACPsetiawan_sukmadjayacNo ratings yet
- Electrolyte Imbalance - Handout PDFDocument23 pagesElectrolyte Imbalance - Handout PDFFaisal Ridho SaktiNo ratings yet
- Electrolyte AbnormalitiesDocument74 pagesElectrolyte Abnormalitiesbluecrush1No ratings yet
- Gangguan Faal GinjalDocument36 pagesGangguan Faal GinjalDanus RamadanusNo ratings yet
- Hyponatremia ADocument44 pagesHyponatremia ASteven Godelman100% (3)
- Fluid & Electrolyte Disturbances 2021Document98 pagesFluid & Electrolyte Disturbances 2021ToyoNo ratings yet
- Electrolyte ImbalanceDocument44 pagesElectrolyte ImbalanceTiven StiveNo ratings yet
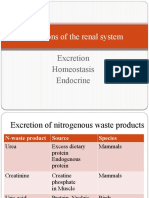
- Functions of The Renal SystemDocument30 pagesFunctions of The Renal SystemBlessing ChirwaNo ratings yet
- Water and Electrolyte ImbalanceDocument49 pagesWater and Electrolyte ImbalanceNur atikahNo ratings yet
- Uzma Mehdi, M.D, Ms NephrologyDocument46 pagesUzma Mehdi, M.D, Ms Nephrologykrish vjNo ratings yet
- Fluid and Electrolytes: Dr. Nupur SarkarDocument24 pagesFluid and Electrolytes: Dr. Nupur SarkarNupurshinjiniNo ratings yet
- Trastornos HidroelectroliticosDocument45 pagesTrastornos HidroelectroliticosIván Mesias PachasNo ratings yet
- Hyponatremia: Dr. Lyra FebriandaDocument49 pagesHyponatremia: Dr. Lyra FebriandaLyra FebriandaNo ratings yet
- Fluid and Electrolyte Imbalances Part 2Document46 pagesFluid and Electrolyte Imbalances Part 2Gabrielle Frances FernandezNo ratings yet
- Electrolyte and Metabolic Disturbances Electrolyte and Metabolic DisturbancesDocument58 pagesElectrolyte and Metabolic Disturbances Electrolyte and Metabolic DisturbancesAbdulrahman Mahmoud GhaziNo ratings yet
- Water and Electrolytes DisturbancesDocument63 pagesWater and Electrolytes Disturbancesj.doe.hex_87No ratings yet
- Electrolyte Abnormalities in The Hospitalized PatientDocument70 pagesElectrolyte Abnormalities in The Hospitalized PatientClaudiaNo ratings yet
- HyponatremiaDocument39 pagesHyponatremiakrataiwanNo ratings yet
- Diagnosis&Manajemen ShockDocument8 pagesDiagnosis&Manajemen ShockHJKIMNo ratings yet
- Anti HTNDocument59 pagesAnti HTNzaha shamseerNo ratings yet
- The Pathophysiology of Hypertension: Abdul Majid/ Eka Roina MDocument51 pagesThe Pathophysiology of Hypertension: Abdul Majid/ Eka Roina MYohanna SinuhajiNo ratings yet
- E.Nasr M.D Professor of Medecine Nephrology Division ST George Hospital University of BalamandDocument51 pagesE.Nasr M.D Professor of Medecine Nephrology Division ST George Hospital University of Balamandsami crowNo ratings yet
- Fluid & ElectrolyteDocument26 pagesFluid & Electrolytesanjana bhatia100% (1)
- 2.2 Fluid & ElectrolytesDocument80 pages2.2 Fluid & ElectrolytesAizza ZarateNo ratings yet
- Hyponatremia: Presenter: DR Arun Karmakar Moderator: Prof. N. SharatkumarDocument50 pagesHyponatremia: Presenter: DR Arun Karmakar Moderator: Prof. N. SharatkumarLyra FebriandaNo ratings yet
- Diabetes Insipidus, Siadh and Cerebral Salt-WastingDocument33 pagesDiabetes Insipidus, Siadh and Cerebral Salt-WastingEuphrasiaNo ratings yet
- Diagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaDocument51 pagesDiagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaHilmaNo ratings yet
- Fluid Electrolyte Balances and ImbalanceDocument157 pagesFluid Electrolyte Balances and ImbalanceManisha Shakya0% (1)
- Dr. Vineet ChaturvediDocument69 pagesDr. Vineet ChaturvediVinay PatilNo ratings yet
- Electrolyte ImbalanceDocument44 pagesElectrolyte ImbalanceDevi Christina Damanik (Papua medical School)No ratings yet
- MNT Penyakit GinjalDocument41 pagesMNT Penyakit GinjalNurfitriana DwiNo ratings yet
- S.gaus-Management of Life-Threatening (Kuliah Sistem) 2Document46 pagesS.gaus-Management of Life-Threatening (Kuliah Sistem) 2Ta RaNo ratings yet
- Renal Lecture 1aDocument34 pagesRenal Lecture 1atyhbbhhNo ratings yet
- Di, Siadh, CSW Tabel PerbedaanDocument17 pagesDi, Siadh, CSW Tabel PerbedaanMichael Tambunan100% (1)
- Fluid & Electrolytes: DR Win Min OoDocument55 pagesFluid & Electrolytes: DR Win Min OoBiomedical Science MyanmarNo ratings yet
- Body Fluids and ElectrolytesDocument42 pagesBody Fluids and ElectrolytesQusaiBadr100% (1)
- Handout 7 Peripheral Vascular Disorders PDFDocument9 pagesHandout 7 Peripheral Vascular Disorders PDFGrape JuiceNo ratings yet
- Hypokalaemia and HyperkalaemiaDocument39 pagesHypokalaemia and HyperkalaemiaRZ NgNo ratings yet
- Hypertension 66Document36 pagesHypertension 66rajeswariNo ratings yet
- Management of Acute Kidney InjuryDocument31 pagesManagement of Acute Kidney InjurysumitNo ratings yet
- Di, Siadh, CSWDocument17 pagesDi, Siadh, CSWNyomanGinaHennyKristiantiNo ratings yet
- Fluid & Electrolyte Management & Acid Base Disorders: Alice Augustin Amina S Anagha P RDocument47 pagesFluid & Electrolyte Management & Acid Base Disorders: Alice Augustin Amina S Anagha P RAsif AbbasNo ratings yet
- Acute Kidney Failure: Dr. Syamsudin, M.Biomed Fakultas Farmasi Universitas PancasilaDocument48 pagesAcute Kidney Failure: Dr. Syamsudin, M.Biomed Fakultas Farmasi Universitas PancasilariyuNo ratings yet
- LP3 NCM 112 Electrolytes2021 UpdatedDocument57 pagesLP3 NCM 112 Electrolytes2021 UpdatedJade CentinoNo ratings yet
- ELECTROLYTES Edited Semi Finals XDDocument52 pagesELECTROLYTES Edited Semi Finals XDzerachiel zephyrNo ratings yet
- Hyponatremia 2017Document10 pagesHyponatremia 2017Isnandita EmeraldaNo ratings yet
- 5x Treatspoints TNCDocument6 pages5x Treatspoints TNCMuhammad Amiro RasheeqNo ratings yet
- 5x Treatspoints Merchant ListDocument1 page5x Treatspoints Merchant ListMuhammad Amiro RasheeqNo ratings yet
- Guidelines For The Management of HyponatraemiaDocument8 pagesGuidelines For The Management of HyponatraemiaMuhammad Amiro RasheeqNo ratings yet
- Febrile Seizure and Epilepsy PDFDocument36 pagesFebrile Seizure and Epilepsy PDFMuhammad Amiro RasheeqNo ratings yet
- ETIC Flyer 2801Document2 pagesETIC Flyer 2801Muhammad Amiro RasheeqNo ratings yet
- Case Study On Head InjuryDocument15 pagesCase Study On Head InjuryPriya SinghNo ratings yet
- Pediatrics in Review. Dehydration 2015Document14 pagesPediatrics in Review. Dehydration 2015Jorge Eduardo Espinoza Rios100% (2)
- Cheat Sheet For Fluid Balance and ElectrolytesDocument2 pagesCheat Sheet For Fluid Balance and ElectrolytesLiel TorresNo ratings yet
- Ii. Hydroelectrolytic Imbalance PDFDocument30 pagesIi. Hydroelectrolytic Imbalance PDFIvanes IgorNo ratings yet
- Rutger's PANRE and PANCE Practice Questions 2 of 2Document38 pagesRutger's PANRE and PANCE Practice Questions 2 of 2nubianlocks100% (3)
- Drug Induced Dyselectrolytemia - A Case ReportDocument4 pagesDrug Induced Dyselectrolytemia - A Case ReportBaru Chandrasekhar RaoNo ratings yet
- Oncological Emergencies From Pathophysiology and Diagnosis To Treatment: A Narrative ReviewDocument22 pagesOncological Emergencies From Pathophysiology and Diagnosis To Treatment: A Narrative ReviewDeni IrwandiNo ratings yet
- Cerebral Salt Wasting Syndrome - StatPearls - NCBI BookshelfDocument4 pagesCerebral Salt Wasting Syndrome - StatPearls - NCBI BookshelfOnggo WiliyantoNo ratings yet
- Etiology and Evaluation of Hypernatremia in Adults - UpToDateDocument26 pagesEtiology and Evaluation of Hypernatremia in Adults - UpToDateMihaela Alexandra RepeziNo ratings yet
- Acute Hemodialysis PrescriptionDocument13 pagesAcute Hemodialysis PrescriptionR DNo ratings yet
- Nutrition For Endurance Sports Marathon, Triathlon, PDFDocument10 pagesNutrition For Endurance Sports Marathon, Triathlon, PDFSheilla ElfiraNo ratings yet
- Fulminant Hepatic FailureDocument33 pagesFulminant Hepatic FailureRojan CardinalNo ratings yet
- Siadh - Patho, Signs, Causes, TreatmentDocument1 pageSiadh - Patho, Signs, Causes, TreatmentVishalNo ratings yet
- Cc2lab Sodium Potassium Quiz WT RevDocument13 pagesCc2lab Sodium Potassium Quiz WT RevJHON JORIES VISMONTENo ratings yet
- PN NCLEX Integrated A 1Document75 pagesPN NCLEX Integrated A 1jedisay1100% (1)
- Dehydration Isonatremic, Hyponatremic, andDocument15 pagesDehydration Isonatremic, Hyponatremic, andalfredoibcNo ratings yet
- Hyponatremia Pocket GuideDocument13 pagesHyponatremia Pocket GuideAtif GazaliNo ratings yet
- Metabolic EncephalopathyDocument26 pagesMetabolic Encephalopathywirdahaja100% (3)
- Assignment SodiumDocument5 pagesAssignment SodiumaqsaNo ratings yet
- Duloxetine PDFDocument4 pagesDuloxetine PDFscribdseewalNo ratings yet
- Renal Siadh Di CSWDocument54 pagesRenal Siadh Di CSWRizka Nurul Firdaus100% (1)
- Metabolic Encephalopaty PDFDocument46 pagesMetabolic Encephalopaty PDFRez QNo ratings yet
- DS PNSSDocument3 pagesDS PNSSKathryne May JinonNo ratings yet
- 1a Introduction To SurgeryDocument109 pages1a Introduction To SurgeryZllison Mae Teodoro MangabatNo ratings yet
- A1.Fundamentals - 25item With Rationale (NCLEX)Document5 pagesA1.Fundamentals - 25item With Rationale (NCLEX)Blardy Falking You Benchod BlardyNo ratings yet
- Amoebiasis CBCDocument2 pagesAmoebiasis CBCImongheartNo ratings yet
- 17 - Toronto Notes 2011 - NephrologyDocument92 pages17 - Toronto Notes 2011 - NephrologyKhairulsani Yusof100% (2)
- Nursing Care Plan For "Fluid and Electrolyte Imbalances"Document37 pagesNursing Care Plan For "Fluid and Electrolyte Imbalances"jhonroks90% (50)
- Case No. 6 Lost The PlotDocument7 pagesCase No. 6 Lost The PlotNermeen AlrajhiNo ratings yet
- Nurse's Study Guide To BurnsDocument14 pagesNurse's Study Guide To BurnsCassie GonzalezNo ratings yet