100% found this document useful (1 vote)
2K views2 pagesForm Blood Requisition
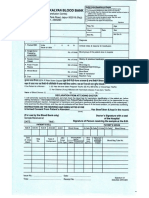
This document is a requisition form for blood or blood components from the Blood Storage Centre at AIIMS Patna. It requires information about the patient, their diagnosis, blood type if known, the reason for transfusion, and the type of blood product required. It specifies that blood samples must be properly labeled with at least 3-5ml in a plain vial and 2ml in an EDTA vial. The form must be signed and have no blank sections or the samples will be unacceptable. The receiving center information and crossmatch results will be filled in, with the technologist and medical officer signatures required.
Uploaded by
shubham kumar ramCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
100% found this document useful (1 vote)
2K views2 pagesForm Blood Requisition
This document is a requisition form for blood or blood components from the Blood Storage Centre at AIIMS Patna. It requires information about the patient, their diagnosis, blood type if known, the reason for transfusion, and the type of blood product required. It specifies that blood samples must be properly labeled with at least 3-5ml in a plain vial and 2ml in an EDTA vial. The form must be signed and have no blank sections or the samples will be unacceptable. The receiving center information and crossmatch results will be filled in, with the technologist and medical officer signatures required.
Uploaded by
shubham kumar ramCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
- Blood Requisition Form
- Cross Match Record