You might also like
- Pentagon Review Royal PentagonDocument33 pagesPentagon Review Royal PentagonRichard Ines Valino99% (70)
- Health InsuranceDocument40 pagesHealth InsuranceSubhadeep SahaNo ratings yet
- Predictors and Outcomes of Shunt-Dependent Hydrocephalus in Patients With Aneurysmal Sub-Arachnoid HemorrhageDocument8 pagesPredictors and Outcomes of Shunt-Dependent Hydrocephalus in Patients With Aneurysmal Sub-Arachnoid HemorrhageNovia AyuNo ratings yet
- (D) Seet2009Document6 pages(D) Seet2009Mohamed MohammedNo ratings yet
- Transfusiones EstablesDocument4 pagesTransfusiones EstablesSusana ViafaraNo ratings yet
- ICU Registered Nurses 2Document8 pagesICU Registered Nurses 211 - JEMELYN LOTERTENo ratings yet
- Mckenzie 2018Document7 pagesMckenzie 2018HeriadyUsmanNo ratings yet
- Artigo - INTUBAÇÃO - Cabeceira ElevadaDocument7 pagesArtigo - INTUBAÇÃO - Cabeceira Elevadatt6jj7pgpxNo ratings yet
- New 2 PDFDocument9 pagesNew 2 PDFImanuel SoniNo ratings yet
- 10 1053@j Jvca 2019 05 017 PDFDocument6 pages10 1053@j Jvca 2019 05 017 PDFangelicaNo ratings yet
- Outcomes After Long-Term Acute Care: An Analysis of 133 Mechanically Ventilated PatientsDocument6 pagesOutcomes After Long-Term Acute Care: An Analysis of 133 Mechanically Ventilated PatientsRoma WestNo ratings yet
- J Chest 2017 08 022Document30 pagesJ Chest 2017 08 022malvindersahiNo ratings yet
- Resuscitation: In-Hospital Cardiac Arrest Outcomes Among Patients With COVID-19 Pneumonia in Wuhan, ChinaDocument6 pagesResuscitation: In-Hospital Cardiac Arrest Outcomes Among Patients With COVID-19 Pneumonia in Wuhan, ChinaOthoniel RamirezNo ratings yet
- Etiologies of Bilateral Pleural EffusionsDocument8 pagesEtiologies of Bilateral Pleural EffusionsAlexander Lukky SugondoNo ratings yet
- 1 s2.0 S1053077022009168 MainDocument8 pages1 s2.0 S1053077022009168 MainOttofianus Alvedo Hewick KalangiNo ratings yet
- Article in Press: Age of Blood and Survival After Massive TransfusionDocument5 pagesArticle in Press: Age of Blood and Survival After Massive TransfusionJosé BlasNo ratings yet
- Subclinical Hypoperfusion in Trauma Patients and Its Influence On Surgical Fracture Fixation: Systematic Review and Meta-AnalysisDocument9 pagesSubclinical Hypoperfusion in Trauma Patients and Its Influence On Surgical Fracture Fixation: Systematic Review and Meta-AnalysisMateoZuluagaGomezNo ratings yet
- 1.1. Pocus en Emg y Critical Care 2018 PDFDocument8 pages1.1. Pocus en Emg y Critical Care 2018 PDFEmergencias RebagliatiNo ratings yet
- Circulation 2011 Kilgannon 2717 22Document7 pagesCirculation 2011 Kilgannon 2717 22Na d'Nazaie CodeNo ratings yet
- Angiography After Out-of-Hospital Cardiac Arrest Without ST-Segment ElevationDocument10 pagesAngiography After Out-of-Hospital Cardiac Arrest Without ST-Segment ElevationYuritza Patricia Vargas OlivaresNo ratings yet
- Endoscopic Retrograde Cholangiopancreatography (ERCP) in Critically Ill Patients Is Safe and Effective When Performed in The Endoscopy SuiteDocument8 pagesEndoscopic Retrograde Cholangiopancreatography (ERCP) in Critically Ill Patients Is Safe and Effective When Performed in The Endoscopy SuiteAgung KaryawinaraNo ratings yet
- TOR Out of HospitalDocument8 pagesTOR Out of HospitalAndrea RivaNo ratings yet
- JurnalDocument6 pagesJurnalayuniNo ratings yet
- Ejemplo1 Tabla1Document12 pagesEjemplo1 Tabla1Isabel MartNo ratings yet
- Effects of Timing of Appendectomy On The Risks of Perforation and Postoperative Complications of Acute AppendicitisDocument9 pagesEffects of Timing of Appendectomy On The Risks of Perforation and Postoperative Complications of Acute AppendicitisLydia EniithNo ratings yet
- Performance in The Shuttle Walk Test Is Associated With Cardiopulmonary Complications After Lung ResectionsDocument10 pagesPerformance in The Shuttle Walk Test Is Associated With Cardiopulmonary Complications After Lung ResectionsAnonymous Skzf3D2HNo ratings yet
- HemothoraxDocument7 pagesHemothoraxElsa CenNo ratings yet
- Accepted Manuscript: 10.1016/j.chest.2016.03.043Document22 pagesAccepted Manuscript: 10.1016/j.chest.2016.03.043Med Issam MahouachiNo ratings yet
- The RUSH Exam Rapid Ultrasound in SHock in The Evaluation of The Critically LLLDocument28 pagesThe RUSH Exam Rapid Ultrasound in SHock in The Evaluation of The Critically LLLMiguel Angel Montoya UrreloNo ratings yet
- Chen 2018Document23 pagesChen 2018María PérezNo ratings yet
- 1 s2.0 S0929664617300487 MainDocument8 pages1 s2.0 S0929664617300487 MainSuryati HusinNo ratings yet
- Skoretz 2014Document8 pagesSkoretz 2014Gonzalo FragaNo ratings yet
- 10 1016@j Jemermed 2019 12 004Document10 pages10 1016@j Jemermed 2019 12 004Fraternity LiviNo ratings yet
- Final Edit Synopsis RUPS PDFDocument20 pagesFinal Edit Synopsis RUPS PDFAMSP IPGMERNo ratings yet
- Inferior Vena Cava Diameter and Collapsibility IndexDocument9 pagesInferior Vena Cava Diameter and Collapsibility IndexmalisalukmanNo ratings yet
- Efficiency and Efficacy of Planning and Care On A Post-Anesthesia Care Unit: A Retrospective Cohort StudyDocument8 pagesEfficiency and Efficacy of Planning and Care On A Post-Anesthesia Care Unit: A Retrospective Cohort Studypooria shNo ratings yet
- HEMOPTISISDocument6 pagesHEMOPTISISJufrialdy AldyNo ratings yet
- Spinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDocument5 pagesSpinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDella Puspita SariNo ratings yet
- 2020 - Early Screening For Aortic Dissection With Point-Of-Care Ultrasound by Emergency PhysiciansDocument7 pages2020 - Early Screening For Aortic Dissection With Point-Of-Care Ultrasound by Emergency PhysiciansMartha Isabel BurgosNo ratings yet
- Thoracoscopic Drainage of EmpyemaDocument5 pagesThoracoscopic Drainage of EmpyemaDr Nilesh NagdeveNo ratings yet
- Paper Reintubación Variable Sexo y EdadDocument5 pagesPaper Reintubación Variable Sexo y EdadAres Kinesiology TapeNo ratings yet
- 2a.330-Removal of Humoral Mediators and The Effect On The Survival of Septic Patients by Hemoperfusion With Neutral Microporous Resin ColumnDocument7 pages2a.330-Removal of Humoral Mediators and The Effect On The Survival of Septic Patients by Hemoperfusion With Neutral Microporous Resin Columngmejiar5237No ratings yet
- Extracorporeal Cardiopulmonary Resuscitation With Therapeutic Hypothermia For Prolonged Refractory In-Hospital Cardiac ArrestDocument10 pagesExtracorporeal Cardiopulmonary Resuscitation With Therapeutic Hypothermia For Prolonged Refractory In-Hospital Cardiac Arrestika nur annisaNo ratings yet
- Readmission and Other Adverse Events After Transsphenoidal Surgery: Prevalence, Timing, and Predictive FactorsDocument9 pagesReadmission and Other Adverse Events After Transsphenoidal Surgery: Prevalence, Timing, and Predictive FactorsbobNo ratings yet
- Thoracoscopic Sympathetic Block To Predict CompensatoryDocument9 pagesThoracoscopic Sympathetic Block To Predict Compensatory이민우No ratings yet
- Critical Care in The Emergency Department: Patient TransferDocument5 pagesCritical Care in The Emergency Department: Patient TransferIqbal TawakkalNo ratings yet
- Two-Year Outcome After Endovascular Treatment For Acute Ischemic StrokeDocument9 pagesTwo-Year Outcome After Endovascular Treatment For Acute Ischemic Strokedoni anandaNo ratings yet
- WJC 7 86Document16 pagesWJC 7 86misbahNo ratings yet
- Jos 2015 01655Document14 pagesJos 2015 01655Arvin Anwar SamanteNo ratings yet
- Performance Evaluation of Five Different Disseminated Intravascular Coagulation (DIC) Diagnostic Criteria For Predicting Mortality in Patients With Complicated SepsisDocument8 pagesPerformance Evaluation of Five Different Disseminated Intravascular Coagulation (DIC) Diagnostic Criteria For Predicting Mortality in Patients With Complicated SepsisDwika AudiyanandaNo ratings yet
- Reference Point For Central Venous Pressure.145 PDFDocument1 pageReference Point For Central Venous Pressure.145 PDFRuth AkswaNo ratings yet
- Ivac 176Document5 pagesIvac 176Issa AbuzeidNo ratings yet
- Transthoracic Echocardiography For Cardiopulmonary Monitoring in Intensive Care (FATE)Document9 pagesTransthoracic Echocardiography For Cardiopulmonary Monitoring in Intensive Care (FATE)Anish H DaveNo ratings yet
- Transthoracic Echocardiography During Prone Position Ventilation: Lessons From The COVID-19 PandemicDocument7 pagesTransthoracic Echocardiography During Prone Position Ventilation: Lessons From The COVID-19 PandemicGeraldo Pozos VazquezNo ratings yet
- JournalDocument6 pagesJournalchardel_08No ratings yet
- Ecotee Guided Canulation Ecmo CovidDocument10 pagesEcotee Guided Canulation Ecmo Covidjuajimenez55No ratings yet
- A Descriptive Comparison of Ultrasound-Guided Central Venous Cannulation of The Internal Jugular Vein To Landmark-Based Subclavian Vein CannulationDocument7 pagesA Descriptive Comparison of Ultrasound-Guided Central Venous Cannulation of The Internal Jugular Vein To Landmark-Based Subclavian Vein CannulationcignalNo ratings yet
- (19330693 - Journal of Neurosurgery) Bypassing The Intensive Care Unit For Patients With Acute Ischemic Stroke Secondary To Large-Vessel OcclusionDocument5 pages(19330693 - Journal of Neurosurgery) Bypassing The Intensive Care Unit For Patients With Acute Ischemic Stroke Secondary To Large-Vessel OcclusionBruno MañonNo ratings yet
- Cost of Extracorporeal Membrane Oxygenation: Evidence From The Rikshospitalet University Hospital, Oslo, NorwayDocument4 pagesCost of Extracorporeal Membrane Oxygenation: Evidence From The Rikshospitalet University Hospital, Oslo, NorwayArief LiemNo ratings yet
- Meroni2017 CompressedDocument8 pagesMeroni2017 Compresseddayllyn iglesiasNo ratings yet
- Trombolisis en PCR ExtrahospitalarioDocument12 pagesTrombolisis en PCR ExtrahospitalarioMariangel PerezNo ratings yet
- Damage Control Resuscitation: Identification and Treatment of Life-Threatening HemorrhageFrom EverandDamage Control Resuscitation: Identification and Treatment of Life-Threatening HemorrhagePhilip C. SpinellaNo ratings yet
- Catalogue - Bertin - Complet - NHP - Eng WebDocument40 pagesCatalogue - Bertin - Complet - NHP - Eng WebWELLINGTON VASCONCELOSNo ratings yet
- Cutaneous Chemical Burns: Assessment and Early Management: Australian Family Physician May 2015Document6 pagesCutaneous Chemical Burns: Assessment and Early Management: Australian Family Physician May 2015WELLINGTON VASCONCELOSNo ratings yet
- Sequeira 2016Document7 pagesSequeira 2016WELLINGTON VASCONCELOSNo ratings yet
- Hazardous Materials Incident Command 141.348Document1 pageHazardous Materials Incident Command 141.348WELLINGTON VASCONCELOSNo ratings yet
- Ics 1109Document9 pagesIcs 1109WELLINGTON VASCONCELOSNo ratings yet
- Journal ClubDocument3 pagesJournal ClubAmreen RahmanNo ratings yet
- Small Vessel Disease in The Heart and Brain Berry (2019) ##Document16 pagesSmall Vessel Disease in The Heart and Brain Berry (2019) ##Jim BeamNo ratings yet
- Secondary Stroke PreventionDocument17 pagesSecondary Stroke PreventionNidia BracamonteNo ratings yet
- Caste, Health and BuddhismDocument10 pagesCaste, Health and BuddhismsrdarapuriNo ratings yet
- Care of Clients With Life Threatening Conditions, Acutely Ill/Multi-Organ Problems, High Acuity, and Emergency SituationDocument75 pagesCare of Clients With Life Threatening Conditions, Acutely Ill/Multi-Organ Problems, High Acuity, and Emergency SituationleonielainecolbornNo ratings yet
- Diagnosis and Treatment of Peripheral Arterial DiseaseDocument5 pagesDiagnosis and Treatment of Peripheral Arterial Diseasedrpiratheepan4274No ratings yet
- PSY322 Chap 7 - Physical Disorders and Health PsychologyDocument10 pagesPSY322 Chap 7 - Physical Disorders and Health PsychologyGabrielle Parla100% (1)
- Stroke Prevention in Patients With Acute Ischemic Stroke and Atrial Fibrillation in Germany - A Cross Sectional SurveyDocument4 pagesStroke Prevention in Patients With Acute Ischemic Stroke and Atrial Fibrillation in Germany - A Cross Sectional Surveymasyuni cantika sariNo ratings yet
- Body Weight Support Treadmill TrainingDocument23 pagesBody Weight Support Treadmill Trainingvidyasagar pagillaNo ratings yet
- Cortical Visual Impairment: Pediatrics in Review November 2009Document13 pagesCortical Visual Impairment: Pediatrics in Review November 2009Amal AlmutiriNo ratings yet
- Diagnosis and Management of Subarachnoid HemorrhageDocument25 pagesDiagnosis and Management of Subarachnoid HemorrhageMisael ClintonNo ratings yet
- Common Medical AbbreviationDocument25 pagesCommon Medical AbbreviationKim Glaidyl BontuyanNo ratings yet
- Cerebral AneurysmDocument6 pagesCerebral AneurysmNavjot BrarNo ratings yet
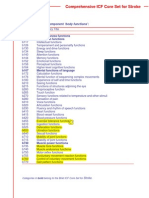
- Comprehensive and Brief ICF Core Sets Stroke1Document4 pagesComprehensive and Brief ICF Core Sets Stroke1robins kumarNo ratings yet
- Pin Perdossi 2020 Vol 3Document369 pagesPin Perdossi 2020 Vol 3Rita Purnama DeuNo ratings yet
- Vascular Dementia (Case Study)Document22 pagesVascular Dementia (Case Study)Coleen Mae CamaristaNo ratings yet
- A Study To Assess The Effectiveness of Swallowing Exercises On Swallowing Ability Among Patients WithDocument8 pagesA Study To Assess The Effectiveness of Swallowing Exercises On Swallowing Ability Among Patients WithpriyagerardNo ratings yet
- MIMS Doctor August 2015 RGDocument48 pagesMIMS Doctor August 2015 RGDika MidbrainNo ratings yet
- Reduction in Spasticity in Stroke Patient With Paraffin TherapyDocument10 pagesReduction in Spasticity in Stroke Patient With Paraffin TherapyayuNo ratings yet
- (What Do I Do Now - ) Sara C. LaHue, Morris Levin - Emergency Neurology (What Do I Do Now - ) - Oxford University Press (2021)Document241 pages(What Do I Do Now - ) Sara C. LaHue, Morris Levin - Emergency Neurology (What Do I Do Now - ) - Oxford University Press (2021)Andreea AtănăsoaeiNo ratings yet
- Cerebrovascular AccidentDocument79 pagesCerebrovascular AccidentKathy B. AbuanNo ratings yet
- Gynera: Coated TabletsDocument67 pagesGynera: Coated TabletsOdeke VascoNo ratings yet
- Global Burden of Cardiovascular Disease: Cardiovascular Diseases in IndiaDocument17 pagesGlobal Burden of Cardiovascular Disease: Cardiovascular Diseases in IndiaSaurabh BhattacharyaNo ratings yet
- Abstract of Re-Orientation Course For Ayurvedic DoctorsDocument22 pagesAbstract of Re-Orientation Course For Ayurvedic DoctorsYoga FMUNo ratings yet
- Tiki Taka Notes Final PDFDocument104 pagesTiki Taka Notes Final PDFAditiSahak62No ratings yet
- Heat Stroke: Ann Disaster Med Vol 2 Suppl 2 2004Document13 pagesHeat Stroke: Ann Disaster Med Vol 2 Suppl 2 2004AniNo ratings yet
- Final CVD 2 Hypertension Stroke PAD Student Full PageDocument74 pagesFinal CVD 2 Hypertension Stroke PAD Student Full PageChelsea JiangNo ratings yet
- Σκορ ΛιονηDocument38 pagesΣκορ ΛιονηΑντώνιος ΧατζηγεωργίουNo ratings yet