You might also like
- Evolution of The HMO in The PhilippinesDocument17 pagesEvolution of The HMO in The PhilippinesdelNo ratings yet
- Peripheral Arterial Disease Diagnosis and ManagementDocument22 pagesPeripheral Arterial Disease Diagnosis and ManagementAlexandra LFNo ratings yet
- Peripheral Arterial Disease Diagnosis and Management PDF 35109575873989Document25 pagesPeripheral Arterial Disease Diagnosis and Management PDF 35109575873989Flavia INo ratings yet
- Stroke and Transient Ischaemic Attack in Over 16s Diagnosis and Initial Management PDF 66141665603269Document48 pagesStroke and Transient Ischaemic Attack in Over 16s Diagnosis and Initial Management PDF 66141665603269doctorebrahimNo ratings yet
- Hypertension in Adults Diagnosis and Management PDF 66141722710213Document51 pagesHypertension in Adults Diagnosis and Management PDF 66141722710213Kreisl DizonNo ratings yet
- Acute Coronary SyndromesDocument57 pagesAcute Coronary SyndromesAmiydhar MishraNo ratings yet
- Chronic Heart Failure Chronic Heart Failure OverviewDocument7 pagesChronic Heart Failure Chronic Heart Failure OverviewYoan Manuel Ruiz ArencibiaNo ratings yet
- HypertensionDocument51 pagesHypertensionEvediciNo ratings yet
- Hypertension in Adults Diagnosis and Management PDF 66141722710213Document51 pagesHypertension in Adults Diagnosis and Management PDF 66141722710213hailemariam gebrehiwotNo ratings yet
- Thyroid Disease - Assessment and Management (NICE Guideline) (NG145) (2019)Document59 pagesThyroid Disease - Assessment and Management (NICE Guideline) (NG145) (2019)Jose VilelaNo ratings yet
- Hypertension in Adults Diagnosis and Management PDF 66141722710213Document54 pagesHypertension in Adults Diagnosis and Management PDF 66141722710213dramorenogeriaNo ratings yet
- Chronic Kidney Disease Assessment and Management PDF 66143713055173Document77 pagesChronic Kidney Disease Assessment and Management PDF 66143713055173Javier Martin Bartolo GarciaNo ratings yet
- Headaches in Over 12s Diagnosis and Management PDF 35109624582853Document32 pagesHeadaches in Over 12s Diagnosis and Management PDF 35109624582853Rahman SunnyNo ratings yet
- Unstable Angina and Nstemi Early Management PDF 975749355205 PDFDocument30 pagesUnstable Angina and Nstemi Early Management PDF 975749355205 PDFNovita AfsariNo ratings yet
- Venous Thromboembolic Diseases Diagnosis Management and Thrombophilia Testing PDF 66141847001797Document55 pagesVenous Thromboembolic Diseases Diagnosis Management and Thrombophilia Testing PDF 66141847001797Ola ZahraNo ratings yet
- Unstable Angina and NSTEMI: The Early Management of Unstable Angina and non-ST-segment-elevation Myocardial InfarctionDocument26 pagesUnstable Angina and NSTEMI: The Early Management of Unstable Angina and non-ST-segment-elevation Myocardial InfarctionCristian PeñaNo ratings yet
- Stroke and Transient Ischaemic Attack in Over 16s Diagnosis and Initial Management PDF 66141665603269Document44 pagesStroke and Transient Ischaemic Attack in Over 16s Diagnosis and Initial Management PDF 66141665603269Gonzalo AltamiranoNo ratings yet
- Type 1 Diabetes in Adults Diagnosis and Management PDF 1837276469701Document64 pagesType 1 Diabetes in Adults Diagnosis and Management PDF 1837276469701cendibarraNo ratings yet
- Acute Kidney Injury Prevention Detection and Management PDF 66141786535621 PDFDocument26 pagesAcute Kidney Injury Prevention Detection and Management PDF 66141786535621 PDFNelson RosasNo ratings yet
- Head Injury Assessment and Early Management PDF 66143892774085Document75 pagesHead Injury Assessment and Early Management PDF 66143892774085evripidis tziokasNo ratings yet
- Pancreatitis PDF 66141537952453Document23 pagesPancreatitis PDF 66141537952453birhanu Ayenew AnleyNo ratings yet
- Posttraumatic Stress Disorder PDF 66141601777861Document54 pagesPosttraumatic Stress Disorder PDF 66141601777861Cesia Constanza Leiva GonzalezNo ratings yet
- Multimorbidity Clinical Assessment and ManagementDocument23 pagesMultimorbidity Clinical Assessment and ManagementAs Minhas OrigensNo ratings yet
- Acute Myocardial Infarction AMI - Secondary PreventionDocument59 pagesAcute Myocardial Infarction AMI - Secondary PreventiondcicareNo ratings yet
- Rehabilitation After Critical Illness in Adults PDF 975687209413Document20 pagesRehabilitation After Critical Illness in Adults PDF 975687209413martinNo ratings yet
- Guidline Glaucoma From NICEDocument37 pagesGuidline Glaucoma From NICEIntan Oktaviana AdiyantoNo ratings yet
- hip-fracture-management-pdf-35109449902789Document26 pageship-fracture-management-pdf-35109449902789Jawhar DhiafNo ratings yet
- Diverticular Disease Diagnosis and Management PDF 66141784856005Document37 pagesDiverticular Disease Diagnosis and Management PDF 66141784856005Javiera Paz Guerrero CassanelloNo ratings yet
- Chronic-Heart-Failure-Managing-Chronic-Heart-Failure 2Document15 pagesChronic-Heart-Failure-Managing-Chronic-Heart-Failure 2ErikaAdamNo ratings yet
- CG95Document33 pagesCG95KawaNo ratings yet
- The Management of Atrial FibrillationDocument41 pagesThe Management of Atrial FibrillationJoyee BasuNo ratings yet
- Parkinsons Disease in Adults PDF 1837629189061Document31 pagesParkinsons Disease in Adults PDF 1837629189061ManCkNo ratings yet
- Delirium Prevention Diagnosis and Management in Hospital and Longterm Care PDF 35109327290821Document25 pagesDelirium Prevention Diagnosis and Management in Hospital and Longterm Care PDF 35109327290821Sara OlmosNo ratings yet
- PEP NiceDocument40 pagesPEP NiceMaria Antonia Ribot MiquelNo ratings yet
- Acute Kidne Acute Kidney Injury: Pre y Injury: Prevvention, Ention, Detection and Management Detection and ManagementDocument39 pagesAcute Kidne Acute Kidney Injury: Pre y Injury: Prevvention, Ention, Detection and Management Detection and ManagementIdris IkhsanNo ratings yet
- Stroke Stroke OverviewDocument7 pagesStroke Stroke OverviewJennicaNo ratings yet
- Guía NICE - 2021Document60 pagesGuía NICE - 2021reymistery10No ratings yet
- abdominal-aortic-aneurysm-diagnosis-and-management-pdf-66141843642565Document53 pagesabdominal-aortic-aneurysm-diagnosis-and-management-pdf-66141843642565Ricardo Arturo Frias RodriguezNo ratings yet
- Subarachnoid Haemorrhage Caused by A Ruptured Aneu 230305 033407Document48 pagesSubarachnoid Haemorrhage Caused by A Ruptured Aneu 230305 033407Berenice G VelazquezNo ratings yet
- Type 2 Diabetes in Adults Management PDF 1837338615493Document53 pagesType 2 Diabetes in Adults Management PDF 1837338615493hakim shaikhNo ratings yet
- Management of Stable Angina: Quick Reference GuideDocument13 pagesManagement of Stable Angina: Quick Reference GuideImania AssagafNo ratings yet
- Type 2 Diabetes in Adults Management PDF 1837338615493Document59 pagesType 2 Diabetes in Adults Management PDF 1837338615493ENINE RESTAURANT CompanyNo ratings yet
- CG 79 Nice GuidelineDocument35 pagesCG 79 Nice GuidelineSisi PapaNo ratings yet
- Guía NICe 2022Document55 pagesGuía NICe 2022Lucila BernasconiNo ratings yet
- Hypertension in Adults Diagnosis and Management PDF 66141722710213Document47 pagesHypertension in Adults Diagnosis and Management PDF 66141722710213ElvisNo ratings yet
- Crohns Disease Management PDF 66141667282885Document24 pagesCrohns Disease Management PDF 66141667282885Amila ShyamalNo ratings yet
- Glaucoma Diagnosis and Management PDF 1837689655237Document37 pagesGlaucoma Diagnosis and Management PDF 1837689655237hailemariam gebrehiwotNo ratings yet
- Irritable Bowel Syndrome in Adults Diagnosis and Management PDF 975562917829Document22 pagesIrritable Bowel Syndrome in Adults Diagnosis and Management PDF 975562917829SUBHADIPNo ratings yet
- Esclerosis Multiple en Adultos Manejo NICE 2022Document52 pagesEsclerosis Multiple en Adultos Manejo NICE 2022tabeto100No ratings yet
- Glaucoma: Diagnosis and Management Glaucoma: Diagnosis and ManagementDocument41 pagesGlaucoma: Diagnosis and Management Glaucoma: Diagnosis and ManagementThieya WardahNo ratings yet
- Attention Deficit Hyperactivity Disorder Diagnosis and Management PDF 1837699732933Document61 pagesAttention Deficit Hyperactivity Disorder Diagnosis and Management PDF 1837699732933evertonlfoNo ratings yet
- Prostate Cancer Diagnosis and Management PDF 66141714312133Document58 pagesProstate Cancer Diagnosis and Management PDF 66141714312133Tafadzwa BonderaNo ratings yet
- CHBM 3Document25 pagesCHBM 3سعيد آل خزيمNo ratings yet
- Sindromes Coronarios Agudos NICE 2020Document54 pagesSindromes Coronarios Agudos NICE 2020selcontreras5No ratings yet
- Diabetic Foot Problems Prevention and Management PDF 1837279828933Document47 pagesDiabetic Foot Problems Prevention and Management PDF 1837279828933Isidora GreeneNo ratings yet
- Ulcerative Colitis Management PDF 66141712632517Document31 pagesUlcerative Colitis Management PDF 66141712632517nathanaellee92No ratings yet
- Venous Thromboembolic Diseases Diagnosis Management and Thrombophilia Testing PDF 66141847001797Document47 pagesVenous Thromboembolic Diseases Diagnosis Management and Thrombophilia Testing PDF 66141847001797Fachrida RahmahNo ratings yet
- Niceng180er4 bm2Document53 pagesNiceng180er4 bm2ManCkNo ratings yet
- NICE DiverticuarDocument37 pagesNICE DiverticuarjackdurrantNo ratings yet
- Hypertension in Pregnancy Diagnosis and Management PDF 66141717671365Document57 pagesHypertension in Pregnancy Diagnosis and Management PDF 66141717671365Jeli Jati Anggeria100% (1)
- Congestive Heart FailureDocument6 pagesCongestive Heart FailureMarcelita DuwiriNo ratings yet
- App10 Et1Document48 pagesApp10 Et1Marcelita DuwiriNo ratings yet
- Chronic Fatigue Syndrome: Aetiology, Diagnosis and TreatmentDocument12 pagesChronic Fatigue Syndrome: Aetiology, Diagnosis and TreatmentMarcelita DuwiriNo ratings yet
- Treatment of Congestive Heart Failure: Guidelines For The Primary Care Physician and The Heart Failure SpecialistDocument12 pagesTreatment of Congestive Heart Failure: Guidelines For The Primary Care Physician and The Heart Failure SpecialistJane Arian BerzabalNo ratings yet
- Guideline Clinical Investigation Medicinal Products Treatment Chronic Heart Failure Revision 2 enDocument15 pagesGuideline Clinical Investigation Medicinal Products Treatment Chronic Heart Failure Revision 2 enMarcelita DuwiriNo ratings yet
- Chronic Fatigue Syndrome A ReviewDocument16 pagesChronic Fatigue Syndrome A ReviewMarcelita DuwiriNo ratings yet
- Mja 250553Document6 pagesMja 250553Marcelita DuwiriNo ratings yet
- CDC Grand Rounds: Chronic Fatigue Syndrome - Advancing Research and Clinical EducationDocument5 pagesCDC Grand Rounds: Chronic Fatigue Syndrome - Advancing Research and Clinical EducationMarcelita DuwiriNo ratings yet
- Nephrotic Syndrome and Hypertension Nahla I. A L. Gabban Essam Ahmed Abdullah Haider Nadhim Abd FicmsDocument6 pagesNephrotic Syndrome and Hypertension Nahla I. A L. Gabban Essam Ahmed Abdullah Haider Nadhim Abd FicmsMarcelita DuwiriNo ratings yet
- Fulltext - JPCHC v5 Id1035Document9 pagesFulltext - JPCHC v5 Id1035Marcelita DuwiriNo ratings yet
- Medip, IJCP-2856 ODocument6 pagesMedip, IJCP-2856 OMarcelita DuwiriNo ratings yet
- TPMD 200176Document2 pagesTPMD 200176Marcelita DuwiriNo ratings yet
- Tinea Corporis Caused by Microsporum Canis - A CasDocument2 pagesTinea Corporis Caused by Microsporum Canis - A CasMarcelita DuwiriNo ratings yet
- Aspc 01 0014Document2 pagesAspc 01 0014Marcelita DuwiriNo ratings yet
- OSDE HIV-AIDS PresentationDocument22 pagesOSDE HIV-AIDS PresentationMarcelita DuwiriNo ratings yet
- Compulsory Health Certificate for Amarnath YatraDocument1 pageCompulsory Health Certificate for Amarnath YatraEknath KoliNo ratings yet
- Reducing NMR Through Basic Neonatal Care UpgradationDocument31 pagesReducing NMR Through Basic Neonatal Care UpgradationdrravikchNo ratings yet
- Human Diseases 8th Edition Zelman Test BankDocument19 pagesHuman Diseases 8th Edition Zelman Test BankAshleyWilsonicye100% (11)
- Bioavailability & Bioequivalence Pharmacokinetic PrinciplesDocument24 pagesBioavailability & Bioequivalence Pharmacokinetic PrinciplesKoya AnushareddyNo ratings yet
- Analysis of Quantitative Studies - EditedDocument7 pagesAnalysis of Quantitative Studies - EditedViotry ChepkwonyNo ratings yet
- Perceptions Attitudes and Practices Toward Research - 2014 - Saudi PharmaceutiDocument5 pagesPerceptions Attitudes and Practices Toward Research - 2014 - Saudi PharmaceutiRawan MaherNo ratings yet
- Peace Corps Medical Doctor, Nurse, Nurse Practitioner or Physician Assistant - Contract PCMODocument3 pagesPeace Corps Medical Doctor, Nurse, Nurse Practitioner or Physician Assistant - Contract PCMOAccessible Journal Media: Peace Corps DocumentsNo ratings yet
- A Comparative Study of Two Nebulizers in The Emergency Department Breath-Actuated Nebulizer and Handheld NebulizerDocument7 pagesA Comparative Study of Two Nebulizers in The Emergency Department Breath-Actuated Nebulizer and Handheld Nebulizerfachrudin arNo ratings yet
- 5a3af95ff1046 Resource Managment Curriculum SternDocument20 pages5a3af95ff1046 Resource Managment Curriculum SternDavid SternNo ratings yet
- Diagnosing and Treating Restricted Mandibular OpeningDocument8 pagesDiagnosing and Treating Restricted Mandibular OpeningAmar BhochhibhoyaNo ratings yet
- Hospital Management SystemDocument38 pagesHospital Management SystemSinta ApNo ratings yet
- NICE Antenatal Care Guidelines SummaryDocument22 pagesNICE Antenatal Care Guidelines SummaryShoaib AkhtarNo ratings yet
- Reglas de Oro en VM en SDRADocument9 pagesReglas de Oro en VM en SDRADiana Laura Sarmiento VázquezNo ratings yet
- Psychosocial interventions ease suffering in complex palliative care patientsDocument7 pagesPsychosocial interventions ease suffering in complex palliative care patientsSiti Malkah KamilahNo ratings yet
- CHP Program 2017Document14 pagesCHP Program 2017Matt GrovesNo ratings yet
- Best Dental Clinics in PrasadampaduDocument3 pagesBest Dental Clinics in Prasadampadukrishna dentalNo ratings yet
- Community Medicine MCQsDocument5 pagesCommunity Medicine MCQsMustafa AdlanNo ratings yet
- Comparison of Vision-Related Quality of Life Between Wearing Orthokeratology Lenses and Spectacles in Myopic Children LDocument5 pagesComparison of Vision-Related Quality of Life Between Wearing Orthokeratology Lenses and Spectacles in Myopic Children Lกนกกานต์ ธาดาธัญลักษณ์No ratings yet
- Is The Nursing Profession in Good Health - Penang MonthlyDocument11 pagesIs The Nursing Profession in Good Health - Penang MonthlyleewfNo ratings yet
- (English (Auto-Generated) ) Why Innovative Uses of Telehealth Should Be Championed - Christine Zack - TEDxReno (DownSub - Com)Document12 pages(English (Auto-Generated) ) Why Innovative Uses of Telehealth Should Be Championed - Christine Zack - TEDxReno (DownSub - Com)audiNo ratings yet
- AV Comment Letter On 2024 MA Advance Notice FINALDocument5 pagesAV Comment Letter On 2024 MA Advance Notice FINALArnold VenturesNo ratings yet
- Uti TreatmentDocument4 pagesUti TreatmentAnne OhNo ratings yet
- QA Policy ManualDocument65 pagesQA Policy Manualmba07-807No ratings yet
- Medical Scribe Resume Morgan NicholsonDocument1 pageMedical Scribe Resume Morgan NicholsonCarol ReidNo ratings yet
- Rundown BCP XviDocument1 pageRundown BCP XviBung HerryNo ratings yet
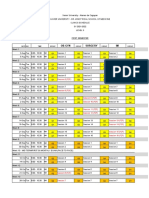
- Level 3 Clinics Schedule Clinics Groupings Group Leaders and PreceptorsDocument24 pagesLevel 3 Clinics Schedule Clinics Groupings Group Leaders and PreceptorsKIM LORIE YAP PASCUALNo ratings yet
- Admin, 044 - 838 - Anthonyus S Bima Pakasi - GalleyDocument5 pagesAdmin, 044 - 838 - Anthonyus S Bima Pakasi - GalleyGusprian Paulus HasibuanNo ratings yet
- Pelaksanaan Sistem Informasi Kesehatan Daerah (SIKDA) Generik Di Unit Rekam Medis Puskesmas Siak Hulu Tahun 2020 Muhammad Dedi Widodo, Reno RenaldiDocument6 pagesPelaksanaan Sistem Informasi Kesehatan Daerah (SIKDA) Generik Di Unit Rekam Medis Puskesmas Siak Hulu Tahun 2020 Muhammad Dedi Widodo, Reno RenaldiRiri LangoyNo ratings yet
- Project Uplift ReportsDocument21 pagesProject Uplift ReportsReno Gazette JournalNo ratings yet