You might also like
- Damage Control in Trauma Care: An Evolving Comprehensive Team ApproachFrom EverandDamage Control in Trauma Care: An Evolving Comprehensive Team ApproachJuan DuchesneNo ratings yet
- A Study of Inguinal Hernia in ChildrenDocument5 pagesA Study of Inguinal Hernia in ChildrenrhmathidayatNo ratings yet
- Abdomen: International Abstracts of Pediatric Surgery 593Document1 pageAbdomen: International Abstracts of Pediatric Surgery 593Yohanes WilliamNo ratings yet
- p1319 PDFDocument4 pagesp1319 PDFSyairodhiNo ratings yet
- Fistula in AnoDocument5 pagesFistula in AnoIoannis ValioulisNo ratings yet
- Intracranial Aneurysms in Childhood: 27-Year Single-Institution ExperienceDocument10 pagesIntracranial Aneurysms in Childhood: 27-Year Single-Institution Experiencezrated786No ratings yet
- Intracranial Aneurysms in Childhood - 27 - Year Sigle Institution ExperienceDocument10 pagesIntracranial Aneurysms in Childhood - 27 - Year Sigle Institution ExperienceRony EvangelistaNo ratings yet
- Intussusception - A Case ReportDocument3 pagesIntussusception - A Case ReportAgustinus HuangNo ratings yet
- In Brief: Inguinal HerniaDocument4 pagesIn Brief: Inguinal HerniaSaf DicamNo ratings yet
- General Considerations: 1392 International AbstractsDocument2 pagesGeneral Considerations: 1392 International Abstractsdewi sumbangNo ratings yet
- Management and Outcome of Testicular Torsion: Background ConclusionDocument4 pagesManagement and Outcome of Testicular Torsion: Background Conclusionabdullahi husseinNo ratings yet
- Pediatric Clinics of North America IIDocument54 pagesPediatric Clinics of North America IIkarenNo ratings yet
- Hirschsprung's Disease: Epidemiology, Diagnosis, and Treatment in A Retrospective Hospital-Based StudyDocument8 pagesHirschsprung's Disease: Epidemiology, Diagnosis, and Treatment in A Retrospective Hospital-Based StudyDandhy Irwan MasdarNo ratings yet
- Rectal Bleeding and PolypsDocument4 pagesRectal Bleeding and PolypsFanny PritaningrumNo ratings yet
- Aydin 2016Document5 pagesAydin 2016nurfitriaNo ratings yet
- Spontaneous Reduction of Intussusception in Infants Is The Glass Half Empty or Half FullDocument4 pagesSpontaneous Reduction of Intussusception in Infants Is The Glass Half Empty or Half FullWorld Journal of Clinical SurgeryNo ratings yet
- Pancreatoblastoma: A Case Report: Indrawati, Rahmayani, Susi Hariyati, SoeriptoDocument5 pagesPancreatoblastoma: A Case Report: Indrawati, Rahmayani, Susi Hariyati, SoeriptoMelati SatriasNo ratings yet
- Matson 1960Document26 pagesMatson 1960Claudia Ivette Villarreal OvalleNo ratings yet
- ParotitisDocument6 pagesParotitisredityoNo ratings yet
- Billmire 1986Document4 pagesBillmire 1986Diannesa April GolosindaNo ratings yet
- Ovarian Cysts and Tumors in Infancy and Childhood: Riginal RticleDocument4 pagesOvarian Cysts and Tumors in Infancy and Childhood: Riginal RticleIwan Budianto HadiNo ratings yet
- Ding 2020Document6 pagesDing 2020Ridha Aswina DalimuntheNo ratings yet
- Diagnosing and managing intussusception in children and adultsDocument6 pagesDiagnosing and managing intussusception in children and adultsCarlos Angel LiraNo ratings yet
- Original Study High Rate of Endometriosis Recurrence in Young WomenDocument4 pagesOriginal Study High Rate of Endometriosis Recurrence in Young WomenAnonymous K0Zh73I72XNo ratings yet
- Ultrasonography Detects Large Mixed-Echo Masses in Immature Ovarian TeratomasDocument8 pagesUltrasonography Detects Large Mixed-Echo Masses in Immature Ovarian TeratomasIlincaNo ratings yet
- Management of Pancreatoblastoma in ChildrenDocument4 pagesManagement of Pancreatoblastoma in ChildrenNermeen Mostafa ElhawaryNo ratings yet
- 1 s2.0 S0266435604000154 Main PDFDocument4 pages1 s2.0 S0266435604000154 Main PDFAlexa1202No ratings yet
- Manejo Quirúrgico de Ránulas Plunging (Cervicales) Una Serie de Casos de 10 Años en El Sureste de Queensland 2017Document5 pagesManejo Quirúrgico de Ránulas Plunging (Cervicales) Una Serie de Casos de 10 Años en El Sureste de Queensland 2017Alex CasauxNo ratings yet
- Pdmr201410 Pediatric AppendicitisDocument14 pagesPdmr201410 Pediatric AppendicitismaithamNo ratings yet
- Benign Esophageal TumorsDocument24 pagesBenign Esophageal TumorsMikael Angeloo100% (1)
- Hirschsprung Disease PDFDocument8 pagesHirschsprung Disease PDFAlchemistalazkaNo ratings yet
- Shappdf25 PDFDocument6 pagesShappdf25 PDFOzzy YunandarNo ratings yet
- Nasopharyngeal Tumor Incidence and Types in TunisiaDocument9 pagesNasopharyngeal Tumor Incidence and Types in TunisiaMohamed ChekraouiNo ratings yet
- 10.1.1.546.6206 BedahDocument7 pages10.1.1.546.6206 Bedahfikri hanifNo ratings yet
- Current Postnatal Management of Antenatally Diagnosed HydronephrosisDocument8 pagesCurrent Postnatal Management of Antenatally Diagnosed HydronephrosisIoannis ValioulisNo ratings yet
- Use of White Blood Cell Count and Negative Appendectomy RateDocument8 pagesUse of White Blood Cell Count and Negative Appendectomy RatePremaKurniaNo ratings yet
- Factors for Successful Nonsurgical Treatment of Pediatric Peritonsillar AbscessDocument4 pagesFactors for Successful Nonsurgical Treatment of Pediatric Peritonsillar AbscessruthameliapNo ratings yet
- Cute Appendicitis in Children: Emergency Department Diagnosis and ManagementDocument13 pagesCute Appendicitis in Children: Emergency Department Diagnosis and ManagementMusyawarah MelalaNo ratings yet
- Current Approach To The Diagnosis and Emergency Department Management of Appendicitis in ChildrenDocument6 pagesCurrent Approach To The Diagnosis and Emergency Department Management of Appendicitis in ChildrenmaithamNo ratings yet
- University of Colorado School of Medicine University of Colorado School of Medicine and Children's Hospital ColoradoDocument2 pagesUniversity of Colorado School of Medicine University of Colorado School of Medicine and Children's Hospital ColoradoashwiniNo ratings yet
- A Retrospective Analysis of Fourniers Gangrene at A TertiaryGovernment Hospital in The PhilippinesDocument3 pagesA Retrospective Analysis of Fourniers Gangrene at A TertiaryGovernment Hospital in The PhilippinesGian PagadduNo ratings yet
- Adnexal Masses in Pregnancy: Surgery Compared With ObservationDocument6 pagesAdnexal Masses in Pregnancy: Surgery Compared With ObservationAgustinus FatollaNo ratings yet
- Infantile Hypertrophic Pyloric Stenosis: A Single Institution's ExperienceDocument3 pagesInfantile Hypertrophic Pyloric Stenosis: A Single Institution's ExperienceTeuku FennyNo ratings yet
- Risk Factors for Wound Dehiscence After Midline LaparotomyDocument4 pagesRisk Factors for Wound Dehiscence After Midline LaparotomyMelisa ClaireNo ratings yet
- GeneticsDocument16 pagesGeneticsJEFFERSON MUÑOZNo ratings yet
- Herlyn Werner WunderlichDocument3 pagesHerlyn Werner WunderlichAgung SentosaNo ratings yet
- Disgerminom OvarianDocument7 pagesDisgerminom OvarianIfrim MihaelaNo ratings yet
- Pediatric Sigmoid Volvulus Case ReportDocument4 pagesPediatric Sigmoid Volvulus Case ReportFKUPR 2017No ratings yet
- 144 FullDocument4 pages144 FullJames FilipNo ratings yet
- DMV Cipe Di AtriaDocument6 pagesDMV Cipe Di AtriaAngélica ContrerasNo ratings yet
- 976 FullDocument6 pages976 FullazifadewiatasyaNo ratings yet
- Jurnal 5Document7 pagesJurnal 5rahayuNo ratings yet
- Benign Esophageal TumoursDocument24 pagesBenign Esophageal Tumourseztouch12No ratings yet
- Incisional HerniaDocument4 pagesIncisional HerniaRini YolandaNo ratings yet
- Laryngomalaci 2016 Ajoshua Bedwell, MD, GeorgeZalzal, MDNDocument4 pagesLaryngomalaci 2016 Ajoshua Bedwell, MD, GeorgeZalzal, MDNwawa chenNo ratings yet
- Recurrent Respiratory Papillomatosis: Case ReportDocument6 pagesRecurrent Respiratory Papillomatosis: Case ReportPradhana FwNo ratings yet
- Correlation of Alvarado Score For Acute Appendicitis With Pathological Acute AppendicitisDocument5 pagesCorrelation of Alvarado Score For Acute Appendicitis With Pathological Acute Appendicitisagus subagiartaNo ratings yet
- Acute appendicitis in children: Key differences from adultsDocument6 pagesAcute appendicitis in children: Key differences from adultsLidiaNo ratings yet
- WJMH 32 110Document6 pagesWJMH 32 110Yacine Tarik AizelNo ratings yet
- Mangement of Thyroglossal Duct CystDocument3 pagesMangement of Thyroglossal Duct CystmohamedhazemelfollNo ratings yet
- Altair Flow Simulator 2021.2 Release Notes HighlightsDocument4 pagesAltair Flow Simulator 2021.2 Release Notes HighlightsOliver RailaNo ratings yet
- 5 Dossier SampleDocument22 pages5 Dossier SampleSabeehuddin SafdarNo ratings yet
- MD Anderson Medical Oncology 4th Edition 2022Document1,694 pagesMD Anderson Medical Oncology 4th Edition 2022Iskandar414100% (6)
- Module 2 Backbencher - ClubDocument16 pagesModule 2 Backbencher - ClubH shashidhar ReddyNo ratings yet
- 10 Days 7 NightsDocument5 pages10 Days 7 NightsSisca SetiawatyNo ratings yet
- Consumer Behaviour 1Document11 pagesConsumer Behaviour 1Rushika ShahNo ratings yet
- RFPDocument88 pagesRFPJayaram Peggem P0% (1)
- User Manual Rish Insu 10Document10 pagesUser Manual Rish Insu 10Manoj TyagiNo ratings yet
- Malware Analysis Project ClusteringDocument11 pagesMalware Analysis Project ClusteringGilian kipkosgeiNo ratings yet
- Department of Civil Engineering, Semester 7th: Different Types of BridgesDocument39 pagesDepartment of Civil Engineering, Semester 7th: Different Types of BridgesSiddhartha SahaNo ratings yet
- Motor Vehicles and Road Traffic Regulation 48.50Document411 pagesMotor Vehicles and Road Traffic Regulation 48.50Clayton AllenNo ratings yet
- Mid 185 - Pid 70 - Fmi 2Document3 pagesMid 185 - Pid 70 - Fmi 2Akbar100% (1)
- Razwan Iqbalcv1Document3 pagesRazwan Iqbalcv1razwaniqbalNo ratings yet
- InfluencerDocument198 pagesInfluencerAkanksha SethiNo ratings yet
- Mapua IT LED Display "Boot SequenceDocument10 pagesMapua IT LED Display "Boot SequenceKristine ToledoNo ratings yet
- Walmart Drug ListDocument6 pagesWalmart Drug ListShirley Pigott MDNo ratings yet
- Comparisonbetweenvrv Vrfbrandssuppliersuaemarket May2016 Bygetco 160430182626Document128 pagesComparisonbetweenvrv Vrfbrandssuppliersuaemarket May2016 Bygetco 160430182626phuongnhsfc100% (1)
- Credit Risk ManagementDocument85 pagesCredit Risk ManagementDarpan GawadeNo ratings yet
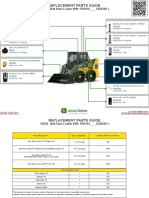
- 312GR Skid Steer Loader PIN 1T0312G G366358 Replacement Parts GuideDocument3 pages312GR Skid Steer Loader PIN 1T0312G G366358 Replacement Parts GuideNelson Andrade VelasquezNo ratings yet
- Harvard Algorithms cs124 NotesDocument6 pagesHarvard Algorithms cs124 NotesYamini DasguptaNo ratings yet
- 10 - A TFT-LCD Source-Driver IC With Charge-Recycling TechniqueDocument11 pages10 - A TFT-LCD Source-Driver IC With Charge-Recycling Techniquematwan29No ratings yet
- Ball ValveDocument12 pagesBall ValveIdabaNo ratings yet
- Systematic Review of The Market Wide Herding Behavior in Asian RegionDocument9 pagesSystematic Review of The Market Wide Herding Behavior in Asian RegionIJAR JOURNALNo ratings yet
- Modern Control Systems Linear Approximation Laplace TransformDocument3 pagesModern Control Systems Linear Approximation Laplace TransformramNo ratings yet
- Copier CoDocument9 pagesCopier CoHun Yao ChongNo ratings yet
- Bachelor of Computer Applications: Pondicherry UniversityDocument49 pagesBachelor of Computer Applications: Pondicherry Universitybalaanand_mcaNo ratings yet
- Q Asgt - Biz Law - A192Document10 pagesQ Asgt - Biz Law - A192otaku himeNo ratings yet
- 524 799 Coach - K - Coach - Knight - CaseDocument15 pages524 799 Coach - K - Coach - Knight - Casekaushalmighty100% (1)
- National Power Corporation vs Philipp Brothers Oceanic Ruling on Moral DamagesDocument2 pagesNational Power Corporation vs Philipp Brothers Oceanic Ruling on Moral DamagesRandy SiosonNo ratings yet
- Test Bank For Web Development and Design Foundations With Html5 6 e 6th Edition 0132783398Document9 pagesTest Bank For Web Development and Design Foundations With Html5 6 e 6th Edition 0132783398Thomas White100% (23)