You might also like
- Expectant Mother and Baby Information SheetDocument3 pagesExpectant Mother and Baby Information SheetJANETH POLINAR72% (53)
- Expectant Mother and Baby Information SheetDocument3 pagesExpectant Mother and Baby Information SheetKristine HP100% (7)
- Pediatric History and Physical Exam TemplateDocument4 pagesPediatric History and Physical Exam TemplateJay Pee Tumaliuan Tumanguil0% (2)
- RegistrantDocument1 pageRegistrantkayerosareNo ratings yet
- Follow UpDocument1 pageFollow UpYohana KifliNo ratings yet
- PRC Form DeliveriesDocument4 pagesPRC Form DeliveriesRosemarie De GuiaNo ratings yet
- Psa Request FormDocument3 pagesPsa Request FormLiza CruzNo ratings yet
- The Philippine Red CrossDocument3 pagesThe Philippine Red CrossKeith Gretchen Lumibao CorumNo ratings yet
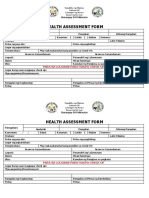
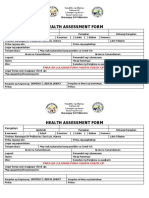
- Health Assessment Form - BHERTDocument2 pagesHealth Assessment Form - BHERTPoblacion 04 San LuisNo ratings yet
- PRC FormDocument1 pagePRC FormCONSUELO MALAZARTENo ratings yet
- Expectant Mother and Baby Information SheetDocument3 pagesExpectant Mother and Baby Information SheetaccountingpcortezNo ratings yet
- In Case of Emergency: in Case of EmergencyDocument1 pageIn Case of Emergency: in Case of EmergencyRonel SuwaisoNo ratings yet
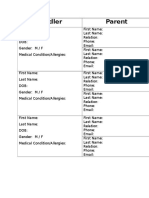
- ToddlerDocument1 pageToddlerJo ZNo ratings yet
- KR Form 1Document1 pageKR Form 1dilg.apayao.luna02No ratings yet
- Single Mother and Baby Info SheetDocument3 pagesSingle Mother and Baby Info SheetontoyatNo ratings yet
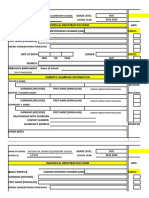
- Individual Early Registration FormDocument1 pageIndividual Early Registration FormSumodio AprilKohNo ratings yet
- The Philippine Red Cross National Headquarters Manila: Rcy Council Officers Information Sheet:: Adviser PresidentDocument2 pagesThe Philippine Red Cross National Headquarters Manila: Rcy Council Officers Information Sheet:: Adviser PresidentGenie SorianoNo ratings yet
- PCR New 2022Document2 pagesPCR New 2022PDRRMO MISOCCNo ratings yet
- CV of Matrix & ExperienceDocument1 pageCV of Matrix & Experienceneocafe1060No ratings yet
- Lab FormDocument1 pageLab FormRHU PeñarandaNo ratings yet
- Student ProfileDocument6 pagesStudent ProfileRoseNo ratings yet
- Litdral Translation Marriage CertificateDocument1 pageLitdral Translation Marriage Certificateirving41594No ratings yet
- Employee Record Form: Employee'S Passport PhotographDocument3 pagesEmployee Record Form: Employee'S Passport PhotographRicksonNo ratings yet
- Blank Life BookDocument20 pagesBlank Life BookArcont ScriptNo ratings yet
- Intake and Output RecordDocument2 pagesIntake and Output RecordKeannu GervacioNo ratings yet
- Enrolment Form 2018 FinalDocument1 pageEnrolment Form 2018 Finalgaicelleann.delarosaNo ratings yet
- Lto Reg FormDocument1 pageLto Reg FormMichelle MalanaNo ratings yet
- GCSPF FormDocument1 pageGCSPF FormWarrior ShortsNo ratings yet
- VS Template 2Document1 pageVS Template 2Nibshian Dela RosaNo ratings yet
- Molo District Health Center: AP (Pre-Natal)Document2 pagesMolo District Health Center: AP (Pre-Natal)Krystel Joy AuroNo ratings yet
- Nfhs Student Health RecordDocument2 pagesNfhs Student Health Recordestudillojesusimo64No ratings yet
- Send Out Form (Perps)Document1 pageSend Out Form (Perps)jelly aNo ratings yet
- Humanities and Social Sciences: Grade 12 Block 9 Gerrah Mia M Chiang AdviserDocument1 pageHumanities and Social Sciences: Grade 12 Block 9 Gerrah Mia M Chiang AdviserCelah C LlaniguezNo ratings yet
- Health Assessment Form: para Sa Luluwas para Magpa-Check UpDocument3 pagesHealth Assessment Form: para Sa Luluwas para Magpa-Check UpPoblacion 04 San LuisNo ratings yet
- Student FormDocument2 pagesStudent FormGracel DagaasNo ratings yet
- National Id Application FormDocument1 pageNational Id Application FormDan GoNo ratings yet
- Paper Information FormDocument4 pagesPaper Information FormMartin RylanceNo ratings yet
- Intake Interview FormDocument4 pagesIntake Interview Formrakhee mehtaNo ratings yet
- HEALTH AND TRAVEL DECLARATION FormDocument1 pageHEALTH AND TRAVEL DECLARATION FormJM Nycyl S. GanancialNo ratings yet
- Boyscout Registration Card Boyscout Registration CardDocument1 pageBoyscout Registration Card Boyscout Registration CardLailyn SantosNo ratings yet
- 1 Application FormDocument1 page1 Application Formapi-3853937No ratings yet
- 2024 Medical Ward EndorsementDocument3 pages2024 Medical Ward EndorsementKarl AbantoNo ratings yet
- Vital SignDocument4 pagesVital SignLoraine SandovalNo ratings yet
- Emergency CardDocument1 pageEmergency CardMynerva JeanNo ratings yet
- Lembar Follow UpDocument1 pageLembar Follow UphayolhoptNo ratings yet
- Dapa ProformaDocument4 pagesDapa ProformaMintu BaruahNo ratings yet
- Assessment Form-PT KirimDocument3 pagesAssessment Form-PT KirimIrvannil Karimah NurcahyoNo ratings yet
- Admission Form - Kooweerup Regional Health ServiceDocument1 pageAdmission Form - Kooweerup Regional Health ServiceAileen ThomsNo ratings yet
- Admitting Trans in ChartDocument2 pagesAdmitting Trans in ChartDiwata BuenviajeNo ratings yet
- Partner 1 Partner 2: Apture of ATA ORMDocument1 pagePartner 1 Partner 2: Apture of ATA ORMjasmine.donohoeNo ratings yet
- Control FormDocument3 pagesControl FormElijah DavidNo ratings yet
- Axa Mansard Health Corporate Proposal Form: Dependents DetailsDocument1 pageAxa Mansard Health Corporate Proposal Form: Dependents DetailsGolden StarNo ratings yet
- Bio - DateDocument1 pageBio - Dategomathi 6faceNo ratings yet
- Employee Personal ProfileDocument3 pagesEmployee Personal ProfileGeorge RizkNo ratings yet
- Espoir Academy Admission Application Editable 3.0Document3 pagesEspoir Academy Admission Application Editable 3.0regan.chetty07No ratings yet
- RCY Council Accreditation ReqmntsDocument11 pagesRCY Council Accreditation ReqmntsRey LacsonNo ratings yet
- IPRFormDocument2 pagesIPRFormSuvendu SahaNo ratings yet
- Name of Hospital .. .. Department of .Document4 pagesName of Hospital .. .. Department of .Sukanya ChakravortyNo ratings yet