You might also like
- BackgroundDocument15 pagesBackgroundcony.juulNo ratings yet
- 2017 Article 3322Document7 pages2017 Article 3322Kevin MandakNo ratings yet
- Survival Rates For Patients With Resected Gastric Adenocarcinoma Finally Have Increased in The United StatesDocument7 pagesSurvival Rates For Patients With Resected Gastric Adenocarcinoma Finally Have Increased in The United StatesXavier QuinteroNo ratings yet
- J Cachexia Sarcopenia Muscle - 2016 - Klassen - Muscle Strength in Breast Cancer Patients Receiving Different TreatmentDocument12 pagesJ Cachexia Sarcopenia Muscle - 2016 - Klassen - Muscle Strength in Breast Cancer Patients Receiving Different TreatmentVukašin Schooly StojanovićNo ratings yet
- ARTICLEMuscle Mass Measured Using Bioelectrical Impedanceanalysis, Calf Circumference and Grip Strength in OlderadultsDocument5 pagesARTICLEMuscle Mass Measured Using Bioelectrical Impedanceanalysis, Calf Circumference and Grip Strength in OlderadultsPPDS Rehab Medik UnhasNo ratings yet
- 1 s2.0 S1743919118306460 MainDocument8 pages1 s2.0 S1743919118306460 MainAnna Margarita MarasiganNo ratings yet
- 11C MetioninaDocument8 pages11C MetioninaPUIGCOZARNo ratings yet
- s00464 013 2881 ZDocument200 pagess00464 013 2881 ZLuis Carlos Moncada TorresNo ratings yet
- Skeletal Muscle Omics Signatures in Cancer CachexiaDocument13 pagesSkeletal Muscle Omics Signatures in Cancer CachexiaMarina GomesNo ratings yet
- T 202200883Document7 pagesT 202200883i'm KaiyNo ratings yet
- Research Literature Gap Activity - Christina OngDocument4 pagesResearch Literature Gap Activity - Christina Ongapi-396204505No ratings yet
- Glioma Imaging: Physiologic, Metabolic, and Molecular ApproachesFrom EverandGlioma Imaging: Physiologic, Metabolic, and Molecular ApproachesWhitney B. PopeNo ratings yet
- (Paper) Obesity May Impair The Early Outcome of Total Knee ArthroplastyDocument5 pages(Paper) Obesity May Impair The Early Outcome of Total Knee ArthroplastyQariahMaulidiahAminNo ratings yet
- 2020 Article 3188Document9 pages2020 Article 3188Abril SantiagoNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 17: OncologyFrom EverandComplementary and Alternative Medical Lab Testing Part 17: OncologyNo ratings yet
- Poster Viewing I Tuesday 1 May 2018 Iii75Document2 pagesPoster Viewing I Tuesday 1 May 2018 Iii75Firdaus Septhy ArdhyanNo ratings yet
- Ef Ficacy and Safety of Stereotactic Body Radiation Therapy For Pediatric Malignancies: The LITE-SABR Systematic Review and Meta-AnalysisDocument12 pagesEf Ficacy and Safety of Stereotactic Body Radiation Therapy For Pediatric Malignancies: The LITE-SABR Systematic Review and Meta-AnalysisRaul Matute MartinNo ratings yet
- Pancreatic Duct TextureDocument9 pagesPancreatic Duct TextureAdarsh GhoshNo ratings yet
- Sarcopenia TacDocument5 pagesSarcopenia TacIvan ChavezNo ratings yet
- 10 1016@j Critrevonc 2020 102962Document16 pages10 1016@j Critrevonc 2020 102962bouh aichetouNo ratings yet
- Sarcopenia Predicts Reduced Survival in Patients With Hepatocellular Carcinoma at First DiagnosisDocument8 pagesSarcopenia Predicts Reduced Survival in Patients With Hepatocellular Carcinoma at First DiagnosisHendra KoncoroNo ratings yet
- S1359634912X00028 S1359634912700253 MainDocument7 pagesS1359634912X00028 S1359634912700253 MainindracuangNo ratings yet
- Who Are The Best Candidates For DecompressiveDocument8 pagesWho Are The Best Candidates For DecompressiverecolenciNo ratings yet
- ClinicalprotocolpdfDocument3 pagesClinicalprotocolpdfapi-631736561No ratings yet
- IdentifyinggapsDocument6 pagesIdentifyinggapsapi-426094285No ratings yet
- Resumen Expo Articulo de InglesDocument7 pagesResumen Expo Articulo de Inglesjosue manuel rivera carrionNo ratings yet
- 2022 48 3 3675 EnglishDocument10 pages2022 48 3 3675 EnglishRaul Matute MartinNo ratings yet
- 1 s2.0 S1836955320300217 MainDocument3 pages1 s2.0 S1836955320300217 Mainjaxad78743No ratings yet
- Low Skeletal Muscle Is Associatd With ToxicityDocument6 pagesLow Skeletal Muscle Is Associatd With ToxicityAna Leticia RibeiroNo ratings yet
- Zhang2018Document9 pagesZhang2018Rodrigo CarvachoNo ratings yet
- Populasi 18Document8 pagesPopulasi 18Resky Ika Sah PutriNo ratings yet
- Simanjuntak 2018 J. Phys. Conf. Ser. 1073 042021 PDFDocument8 pagesSimanjuntak 2018 J. Phys. Conf. Ser. 1073 042021 PDFEko RistiyantoNo ratings yet
- Correlation of NK Cell Activity and Clinical Parameters With Survival in Breast Cancer PatientsDocument15 pagesCorrelation of NK Cell Activity and Clinical Parameters With Survival in Breast Cancer Patientshoangphuong08101992No ratings yet
- Precision Medicine Oncology: A PrimerFrom EverandPrecision Medicine Oncology: A PrimerLorna Rodriguez-RodriguezNo ratings yet
- Exercises MMDocument11 pagesExercises MMAna Luiza ToldoNo ratings yet
- Effects of Glucosamine and Chondroitin Sulfate Supplementation in Addition To Resistance Exercise Training and Manual Therapy in Patients With Knee Osteoarthritis A Randomized Controlled TrialDocument6 pagesEffects of Glucosamine and Chondroitin Sulfate Supplementation in Addition To Resistance Exercise Training and Manual Therapy in Patients With Knee Osteoarthritis A Randomized Controlled TrialalonsoNo ratings yet
- Direk 2013Document13 pagesDirek 2013Rafaela VeigaNo ratings yet
- Escamoso de Esofago Cervical Metaanalisis, Guler 2022Document2 pagesEscamoso de Esofago Cervical Metaanalisis, Guler 2022Carlos N. Rojas PuyolNo ratings yet
- The Physics of Radioembolization - 230807 - 113550Document27 pagesThe Physics of Radioembolization - 230807 - 113550seba gNo ratings yet
- Cancer ScreeningDocument8 pagesCancer Screeninglakshminivas PingaliNo ratings yet
- Does Sarcopenia Predict Change in Mobility After Hip Fracture? A Multicenter Observational Study With One-Year Follow-UpDocument10 pagesDoes Sarcopenia Predict Change in Mobility After Hip Fracture? A Multicenter Observational Study With One-Year Follow-UpliantariNo ratings yet
- Xi, 2021 Tumor Associated Collagen SignaturesDocument15 pagesXi, 2021 Tumor Associated Collagen Signaturesevahendrickx03No ratings yet
- Lamarca 2014Document8 pagesLamarca 2014Ihdinal MuktiNo ratings yet
- PancreatitisDocument13 pagesPancreatitissebas2008No ratings yet
- Armijo 2020Document7 pagesArmijo 2020Yeudiel SuroNo ratings yet
- 10.1007@s11695 020 05012 2Document9 pages10.1007@s11695 020 05012 2Andrés MaldonadoNo ratings yet
- Pharmacogenomic Landscape of Patient-Derived Tumor Cells Informs Precision Oncology TherapyDocument19 pagesPharmacogenomic Landscape of Patient-Derived Tumor Cells Informs Precision Oncology TherapyDyahsekarayupudak wangiNo ratings yet
- Machann2005 PDFDocument8 pagesMachann2005 PDFOrto MespNo ratings yet
- Exercise As An Intervention in Preventing and Reducing Chemotherapy-Induced Cardiotoxicity Among Breast Cancer Survivors - Protocol For A Scoping ReviewDocument4 pagesExercise As An Intervention in Preventing and Reducing Chemotherapy-Induced Cardiotoxicity Among Breast Cancer Survivors - Protocol For A Scoping ReviewdrpraveenkumarNo ratings yet
- Comparison Between Four Modalities of Radiotherapy of Prostate CancerDocument5 pagesComparison Between Four Modalities of Radiotherapy of Prostate CancerEdis ĐedovićNo ratings yet
- Cao Et Al 2021 - The Prevalence of Sarcopenia and Relationships Between Dietary Intake and Muscle Mass in Neck and Head CancerDocument8 pagesCao Et Al 2021 - The Prevalence of Sarcopenia and Relationships Between Dietary Intake and Muscle Mass in Neck and Head Cancerbouh aichetouNo ratings yet
- 1982 4378 Rbort 54 06 0636Document8 pages1982 4378 Rbort 54 06 0636azevedoNo ratings yet
- Role of Carbohydrate Antigen (Ca19-9) and Carcinoembryonic Antigen (Cea) As A Prognostic Factors in Pancreatic CarcinomaDocument6 pagesRole of Carbohydrate Antigen (Ca19-9) and Carcinoembryonic Antigen (Cea) As A Prognostic Factors in Pancreatic CarcinomaIJAR JOURNALNo ratings yet
- Short-Term Surgical and Long-Term Survival Outcomes After Laparoscopic Distal Gastrectomy With D Lymphadenectomy For Gastric CancerDocument7 pagesShort-Term Surgical and Long-Term Survival Outcomes After Laparoscopic Distal Gastrectomy With D Lymphadenectomy For Gastric CancerThế VũNo ratings yet
- Mid-Upper Arm Circumference As An Indicator of UnderweightDocument7 pagesMid-Upper Arm Circumference As An Indicator of UnderweightgianellaNo ratings yet
- Matsuda 2014Document8 pagesMatsuda 2014Adrian SilaghiNo ratings yet
- Article 4Document10 pagesArticle 4umair muqriNo ratings yet
- Tiroides ArticuloDocument9 pagesTiroides Articulojuan sebaastianNo ratings yet
- Ibuprofen: 3) CV of BPPV. Management?Document8 pagesIbuprofen: 3) CV of BPPV. Management?Rushi Shah100% (4)
- Most Common Pathogen in Artificial Rupture of MembranesDocument3 pagesMost Common Pathogen in Artificial Rupture of MembranesRushi Shah100% (1)
- Good Girl Gone Bad - Scene Guide v1 2r2Document80 pagesGood Girl Gone Bad - Scene Guide v1 2r2Rushi Shah0% (1)
- March 2021 USMLE Recalls Actual Exam Questions: Click To Get MoreDocument8 pagesMarch 2021 USMLE Recalls Actual Exam Questions: Click To Get MoreRushi Shah75% (4)
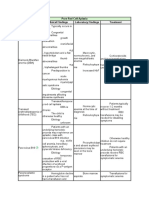
- Pure Red Cell Aplasia Cause Clinical Findings Laboratory Findings TreatmentDocument2 pagesPure Red Cell Aplasia Cause Clinical Findings Laboratory Findings TreatmentRushi ShahNo ratings yet
- 2015 Usmle Review Lecture Histology and Cell Biology I Rhys BrooksDocument25 pages2015 Usmle Review Lecture Histology and Cell Biology I Rhys BrooksRushi ShahNo ratings yet
- Presentation Compulsory Licensing 1Document28 pagesPresentation Compulsory Licensing 1preeti kumariNo ratings yet
- Promoting Chinese Herbal Drugs Through Regulatory Globalisation 2015Document24 pagesPromoting Chinese Herbal Drugs Through Regulatory Globalisation 2015Hung Tsung JenNo ratings yet
- Ebook - Ebfl20120504 PDFDocument136 pagesEbook - Ebfl20120504 PDFayush pathakNo ratings yet
- Development and Novel Therapeutics in Hepatocellular Carcinoma A ReviewDocument11 pagesDevelopment and Novel Therapeutics in Hepatocellular Carcinoma A ReviewgrigmihNo ratings yet
- ONYX PHARMACEUTICALS INC 10-K (Annual Reports) 2009-02-25Document129 pagesONYX PHARMACEUTICALS INC 10-K (Annual Reports) 2009-02-25http://secwatch.comNo ratings yet
- Post Mid Term 2 PDFDocument67 pagesPost Mid Term 2 PDFKathiravan RajendranNo ratings yet
- HCC PresentationDocument37 pagesHCC PresentationnagdadNo ratings yet
- Cases On IprDocument31 pagesCases On IprShreekzNo ratings yet
- Investor Science Conference Call: American Society of Clinical Oncology Gastrointestinal (ASCO GI) Cancers Symposium 2022Document42 pagesInvestor Science Conference Call: American Society of Clinical Oncology Gastrointestinal (ASCO GI) Cancers Symposium 2022BradGourdoNo ratings yet
- IMUNOterapi HCCDocument12 pagesIMUNOterapi HCCAri Dwi PrasetyoNo ratings yet
- Compulsory Licensing of Patents in IndiaDocument4 pagesCompulsory Licensing of Patents in IndiaGauriNo ratings yet
- Investor Presentation (Company Update)Document23 pagesInvestor Presentation (Company Update)Shyam SunderNo ratings yet
- Treating Liver CancerDocument34 pagesTreating Liver Cancermohamed aliNo ratings yet
- About Thyroid Cancer: Overview and TypesDocument12 pagesAbout Thyroid Cancer: Overview and Typesumaima rizwanNo ratings yet
- Ago-Rip Sequencing Identifies New Microrna-449A-5P Target Genes Increasing Sorafenib Efficacy in Hepatocellular CarcinomaDocument14 pagesAgo-Rip Sequencing Identifies New Microrna-449A-5P Target Genes Increasing Sorafenib Efficacy in Hepatocellular Carcinomahasna muhadzibNo ratings yet
- 20IB314 Bayer Corporation Vs Union of IndiaDocument12 pages20IB314 Bayer Corporation Vs Union of IndiaApoorv TyagiNo ratings yet
- Analysis of NATCO Vs BAYER Pharma Case by Ankit SinghDocument18 pagesAnalysis of NATCO Vs BAYER Pharma Case by Ankit SinghAnkit Singh50% (4)
- Radiation Oncology ACR 2010 In-Service Exam RationalesDocument105 pagesRadiation Oncology ACR 2010 In-Service Exam Rationalesjoemudphud100% (3)
- Compulsory License Under Indian LawDocument4 pagesCompulsory License Under Indian LawVishal AnandNo ratings yet
- ESMO World Congress The Management of Hepatocellular Carcinoma 2023Document11 pagesESMO World Congress The Management of Hepatocellular Carcinoma 2023Mohamad MostafaNo ratings yet
- Ctri Data Base India IcmrDocument2,599 pagesCtri Data Base India Icmrdr sanjayNo ratings yet
- Natco Pharma LTD v. Bayer CorporationDocument13 pagesNatco Pharma LTD v. Bayer CorporationRajah RahimNo ratings yet
- Patent Case Brief - Bayer V Union of India - Notes For Free PDFDocument6 pagesPatent Case Brief - Bayer V Union of India - Notes For Free PDFjay1singheeNo ratings yet
- DR Hery Djagat - 2018 Glyzhrhizin in Liver DiseaseDocument41 pagesDR Hery Djagat - 2018 Glyzhrhizin in Liver DiseaseAulia Achmad Yudha PratamaNo ratings yet
- Yoon 2018Document9 pagesYoon 2018Muhammad Yusuf HanifNo ratings yet
- Multidisciplinary Management of Hepatocellular CarcinomaDocument45 pagesMultidisciplinary Management of Hepatocellular CarcinomaSalmanArifNo ratings yet
- Project Report ON "Compulsory Licensing of Patent": Hidayatullah National Law University RAIPUR (C.G.)Document16 pagesProject Report ON "Compulsory Licensing of Patent": Hidayatullah National Law University RAIPUR (C.G.)Devendra Dhruw100% (1)
- UpdateJul2007 3julDocument10 pagesUpdateJul2007 3julAnshul SinghNo ratings yet
- LICENSINGDocument5 pagesLICENSINGIshita AgarwalNo ratings yet
- Bayer Corporation vs. Union of India and Others IPAB 2013Document5 pagesBayer Corporation vs. Union of India and Others IPAB 2013Ginnu ManNo ratings yet