You might also like
- A Leader in Me UK - Big Life JournalDocument7 pagesA Leader in Me UK - Big Life Journalntam100% (1)
- 11.r Health InformaticsDocument107 pages11.r Health InformaticsSingla Ashish100% (1)
- SUMMARY of The Electronic Health RecordDocument3 pagesSUMMARY of The Electronic Health RecordkexonlagodNo ratings yet
- Unit 5-Health Management Information System (HMIS)Document47 pagesUnit 5-Health Management Information System (HMIS)Minlik-alew Dejenie91% (69)
- Health informatics: Improving patient careFrom EverandHealth informatics: Improving patient careBCS, The Chartered Institute for ITRating: 3 out of 5 stars3/5 (1)
- 'To The Hungry Soul Every Bitter Thing Is Sweet.'soldiers' Food and Cooking in The War For IndependenceDocument91 pages'To The Hungry Soul Every Bitter Thing Is Sweet.'soldiers' Food and Cooking in The War For IndependenceJohn U. Rees90% (10)
- Electronic Health Records: A Guide For Clinicians and AdministratorsDocument17 pagesElectronic Health Records: A Guide For Clinicians and AdministratorsLIS_141No ratings yet
- 6852 Community Health Information and Tracking System Chits Lessons From Eight Years Implementation of A Pioneer Electronic Medical Record System in The Philippines PDFDocument16 pages6852 Community Health Information and Tracking System Chits Lessons From Eight Years Implementation of A Pioneer Electronic Medical Record System in The Philippines PDFSMNo ratings yet
- The Field: Health Services InformationDocument34 pagesThe Field: Health Services InformationRyan Michael Oducado100% (4)
- TFN Resource UnitDocument80 pagesTFN Resource UnitAira Alaro50% (2)
- Health Information SystemDocument11 pagesHealth Information SystemVineeta Jose100% (1)
- FHSISDocument31 pagesFHSISNezer SorianoNo ratings yet
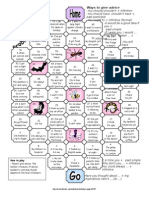
- ESL Board Game Advice NeededDocument3 pagesESL Board Game Advice NeededTrill_Mo0% (1)
- Humko Man Ki Shakti DenaDocument1 pageHumko Man Ki Shakti DenaAnka AV100% (2)
- Online Resume Builder-ReportDocument32 pagesOnline Resume Builder-ReportSakshi Arora76% (17)
- W J T Mitchell Landscape and Power PDFDocument44 pagesW J T Mitchell Landscape and Power PDFgregmoooo100% (1)
- SWRB Social Work Practice Competencies 2Document3 pagesSWRB Social Work Practice Competencies 2api-291442969No ratings yet
- The Hospital Operations and Management Information System Is A ComputerDocument29 pagesThe Hospital Operations and Management Information System Is A ComputerMacaRonie PepeRownie del Rio86% (7)
- HMIS PakistanDocument10 pagesHMIS PakistanHasan HanifNo ratings yet
- Review of Related LiteratureDocument6 pagesReview of Related LiteratureSkyla FiestaNo ratings yet
- 176 Schwefel Marte MIS PhilippinesDocument8 pages176 Schwefel Marte MIS Philippinesserainie maiNo ratings yet
- CHN Lec - Records in Family Health Nursing PracticeDocument6 pagesCHN Lec - Records in Family Health Nursing PracticeArevalo, Denisse S.No ratings yet
- 775-Article Text-3091-1-10-20200106Document15 pages775-Article Text-3091-1-10-20200106ANGEL MARIE GONZAGANo ratings yet
- Deraco, ASA New Technologies To Public HealthDocument2 pagesDeraco, ASA New Technologies To Public HealthAdrea DeracoNo ratings yet
- His Module 5 Activity 2Document1 pageHis Module 5 Activity 2Fharhaina JulkipliNo ratings yet
- 8 Health Sector Information StrategyDocument38 pages8 Health Sector Information StrategyMaheshNo ratings yet
- Ao2023 0005Document15 pagesAo2023 0005Joelean Zephanie Ecleo EscoteNo ratings yet
- Community Health Information Tracking System: Submitted By: Gerna Maie Anne CabilingDocument5 pagesCommunity Health Information Tracking System: Submitted By: Gerna Maie Anne CabilingRammiel Saylo CarlosNo ratings yet
- His Topic 4 Reporting 1Document37 pagesHis Topic 4 Reporting 1Jean Marie FelipeNo ratings yet
- The Ethiopian Health Information System: Where Are We? and Where Are We Going?Document4 pagesThe Ethiopian Health Information System: Where Are We? and Where Are We Going?Wonde GebeyehuNo ratings yet
- Nick POLESTICO (MT 102 HIS LAB. PTSK.)Document4 pagesNick POLESTICO (MT 102 HIS LAB. PTSK.)Nick PolesticoNo ratings yet
- Lesson 6Document1 pageLesson 6Bai Mohannie abdulaNo ratings yet
- Community Health SurveillanceDocument5 pagesCommunity Health SurveillanceNamayanja SumayiyahNo ratings yet
- Diary 5Document1 pageDiary 5Eunicah MandiNo ratings yet
- A Descriptive AnalyticsDocument18 pagesA Descriptive AnalyticsCristy ArellanoNo ratings yet
- UHC Tech BriefDocument4 pagesUHC Tech BrieffitaNo ratings yet
- Health Policy Notes: Harmonize and Strengthen Health Information SystemsDocument6 pagesHealth Policy Notes: Harmonize and Strengthen Health Information SystemsJeffrey AngNo ratings yet
- Field Health Information SystemDocument216 pagesField Health Information SystemnitotalibNo ratings yet
- CHITSDocument17 pagesCHITSJane RosalejosNo ratings yet
- Mls 050 NotesDocument24 pagesMls 050 NotesJulianneNo ratings yet
- Principles Based Medical Informatics For Success NTDocument4 pagesPrinciples Based Medical Informatics For Success NTSvlader Reitef VanquisherNo ratings yet
- District Health Management Information System (Dhmis) PolicyDocument38 pagesDistrict Health Management Information System (Dhmis) PolicySiti AlfianaNo ratings yet
- CSC 222 Course WorkDocument12 pagesCSC 222 Course Workjohn peterNo ratings yet
- Lesson 1 Overview of Health InformaticsDocument5 pagesLesson 1 Overview of Health InformaticsDOMILE, SAMANTHA RIANNENo ratings yet
- Health Information Systems in EthiopiaDocument10 pagesHealth Information Systems in EthiopiaEsayas Ahmed100% (1)
- Healthinformationsystempresentation 140423234415 Phpapp01Document18 pagesHealthinformationsystempresentation 140423234415 Phpapp01Pankaj KumarNo ratings yet
- Unified Health Management Information SystemDocument4 pagesUnified Health Management Information Systemgg22santosNo ratings yet
- Patient Information Systems in The LiteratureDocument6 pagesPatient Information Systems in The LiteratureJohn MunaonyediNo ratings yet
- Acceptability of Information Technology Systems Developed For Distant Philippine Communitiesamong Local Health ProvidersDocument8 pagesAcceptability of Information Technology Systems Developed For Distant Philippine Communitiesamong Local Health ProvidersAr-jay PorrasNo ratings yet
- Sensitization On Current Best Practices in Medical Record & Health Information Management System (HIMS) Health Information Management (Him)Document2 pagesSensitization On Current Best Practices in Medical Record & Health Information Management System (HIMS) Health Information Management (Him)VinithaNo ratings yet
- Chapter 12Document15 pagesChapter 12kk5522No ratings yet
- Ehr Chapter 1 CarterDocument17 pagesEhr Chapter 1 Carterapi-298340093No ratings yet
- Health Information Systems (HIS)Document34 pagesHealth Information Systems (HIS)Abdirahman A. OsmanNo ratings yet
- CHN ReviewerDocument6 pagesCHN ReviewerCherry Ann Cagayat MadrigalNo ratings yet
- p1w4 - His Module 6Document47 pagesp1w4 - His Module 6Joshua Richard Jr Tubiano PayopaninNo ratings yet
- EHealth in The Community SettingDocument22 pagesEHealth in The Community Settingbryanmaranan173No ratings yet
- Field Health Service Information SystemDocument3 pagesField Health Service Information SystemIzelwyn DaguioNo ratings yet
- NCM 110 LEC Trans 1Document39 pagesNCM 110 LEC Trans 1tumabotaboarianeNo ratings yet
- Community Health Nursing Also Called Public Health Nursing or Community NursingDocument2 pagesCommunity Health Nursing Also Called Public Health Nursing or Community NursingZanie CruzNo ratings yet
- Fhsis CHNDocument35 pagesFhsis CHNJocyl Faith SumagaysayNo ratings yet
- DOH ICT SytemDocument19 pagesDOH ICT Sytemricohizon99No ratings yet
- Jones Furukawa 2017 Adoption and Use of Electronic Health Records Among Federally Qualified Health Centers GrewDocument8 pagesJones Furukawa 2017 Adoption and Use of Electronic Health Records Among Federally Qualified Health Centers Grewtylermichael912No ratings yet
- Integration Context NRHMDocument34 pagesIntegration Context NRHMSanchita MondalNo ratings yet
- WHO - The Need For Strong Health Information Systems - Rationale For The HMN FrameworkDocument4 pagesWHO - The Need For Strong Health Information Systems - Rationale For The HMN FrameworkHarumNo ratings yet
- HMIS Group 3Document31 pagesHMIS Group 3TayeNo ratings yet
- His AssDocument4 pagesHis AssRicanie Cadorna0% (1)
- Answers Only - OBE Diary OutputDocument4 pagesAnswers Only - OBE Diary OutputAlliah Jasmine AlcalaNo ratings yet
- Cognitive Informatics: Reengineering Clinical Workflow for Safer and More Efficient CareFrom EverandCognitive Informatics: Reengineering Clinical Workflow for Safer and More Efficient CareKai ZhengNo ratings yet
- TT Emea Xarios EngDocument2 pagesTT Emea Xarios EngDua DoiNo ratings yet
- Solis 1 5k 2g Manual v2 2Document20 pagesSolis 1 5k 2g Manual v2 2Luz Mariel Serrano CastilloNo ratings yet
- Art Appreciation Lesson 1Document11 pagesArt Appreciation Lesson 1Dhiz Adjarain MajindiNo ratings yet
- Supplier Relationship Managemen Peter KraljicDocument4 pagesSupplier Relationship Managemen Peter KraljicSeemaNo ratings yet
- Photoelectrics Amplifier Type S142A.Document4 pagesPhotoelectrics Amplifier Type S142A.shawn hagerichNo ratings yet
- Relationship Between Emotional Intelligence and Students Academic Performance - Role of Ethnic FactorDocument13 pagesRelationship Between Emotional Intelligence and Students Academic Performance - Role of Ethnic Factorمعن الفاعوريNo ratings yet
- Total Station +leicaDocument17 pagesTotal Station +leicaDaro EngineerNo ratings yet
- List Besaran Diskon Maksimal Per Produk: NO Kode Produk Komposisi Kemasan HNADocument10 pagesList Besaran Diskon Maksimal Per Produk: NO Kode Produk Komposisi Kemasan HNAapotekerNo ratings yet
- AnswersPractice Problems - Unit 3 - Open Up ResourcesDocument32 pagesAnswersPractice Problems - Unit 3 - Open Up ResourcesJa'Kyah Allen Student - WakeForestMSNo ratings yet
- Artículo - Assessment of Vitamin D Status - A Changing LandscapeDocument24 pagesArtículo - Assessment of Vitamin D Status - A Changing LandscapePaoloNo ratings yet
- 2018 Vital Signs ReportDocument8 pages2018 Vital Signs ReportAnonymous 7cIsCCnNo ratings yet
- A Textbook of Veterinary General PathologyDocument600 pagesA Textbook of Veterinary General PathologyMachira MuturiNo ratings yet
- 10 55290-Steam 1349238-3359324Document29 pages10 55290-Steam 1349238-3359324g-ipgp29205499No ratings yet
- Lesson 4 SocialisationDocument19 pagesLesson 4 Socialisationtường caoNo ratings yet
- Ampatop Aero (Plus) : Roof and Wall MembraneDocument2 pagesAmpatop Aero (Plus) : Roof and Wall MembraneTimmyNo ratings yet
- Resume Chandni Bansal 2013Document1 pageResume Chandni Bansal 2013api-241251217No ratings yet
- Om l5 Capacity ManagementDocument31 pagesOm l5 Capacity ManagementAthahNo ratings yet
- Year 11 Persepolis Learning PackDocument32 pagesYear 11 Persepolis Learning PackNAKIPEHKSNo ratings yet
- All PHSH BookDocument7 pagesAll PHSH BookArjun BiswasNo ratings yet
- Literature Review For Action Research PaperDocument5 pagesLiterature Review For Action Research Paperea3h1c1p100% (1)
- The Implementation of A Data-Accessing Platform Built From Big Data Warehouse of Electric LoadsDocument6 pagesThe Implementation of A Data-Accessing Platform Built From Big Data Warehouse of Electric LoadsEttaoufik AbdelazizNo ratings yet
- Community in Paraguay - A Visit To The BruderhofDocument106 pagesCommunity in Paraguay - A Visit To The BruderhofBruderhof100% (2)