You might also like
- Global Acne Grading ScoreDocument5 pagesGlobal Acne Grading ScoreMaab MurshidNo ratings yet
- Acmen 4Document8 pagesAcmen 4Fadhila NurrahmaNo ratings yet
- Ficha 1.2 ACNE Severe Acne and Its VariantsDocument3 pagesFicha 1.2 ACNE Severe Acne and Its VariantsArianny SilvaNo ratings yet
- Acne and DiabetesDocument5 pagesAcne and DiabetesMuhammad Nur ArifinNo ratings yet
- Adult Acne Versus Adolescent AcneDocument5 pagesAdult Acne Versus Adolescent AcneVania Andhika PutriNo ratings yet
- Treating Facial Acne in Adolescents and Young Adults With Auriculoacupuncture and AuriculotherapyDocument16 pagesTreating Facial Acne in Adolescents and Young Adults With Auriculoacupuncture and AuriculotherapyPedro MaiaNo ratings yet
- Effectiveness of Oral Albendazole As A Treatment For Pediculosis CapitisDocument6 pagesEffectiveness of Oral Albendazole As A Treatment For Pediculosis CapitisAlmuizzu NurjannahNo ratings yet
- Research Letter: Risk of Depression Among Patients With Acne in The U.K.: A Population-Based Cohort StudyDocument2 pagesResearch Letter: Risk of Depression Among Patients With Acne in The U.K.: A Population-Based Cohort StudyadhastriNo ratings yet
- All 13401Document10 pagesAll 13401hahihouNo ratings yet
- Advance Epi & Direct Acyclic GraphDocument14 pagesAdvance Epi & Direct Acyclic GraphPurnima VermaNo ratings yet
- Sertaconazole For TreatmentDocument5 pagesSertaconazole For TreatmentNanny HerwantoNo ratings yet
- Crisaborole RCTDocument6 pagesCrisaborole RCTNotfor TaoNo ratings yet
- Jurnal Primer - Fluconazole Versus Itraconazole in The Treatment of Tinea VersicolorDocument8 pagesJurnal Primer - Fluconazole Versus Itraconazole in The Treatment of Tinea VersicolorKopitesNo ratings yet
- Jcad 8 4 21Document5 pagesJcad 8 4 21Rosyid PrasetyoNo ratings yet
- Profile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyDocument6 pagesProfile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyRose ParkNo ratings yet
- Profile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyDocument6 pagesProfile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyMarwiyahNo ratings yet
- 2014 Dermatological EmergenciesDocument7 pages2014 Dermatological EmergenciesSejal ThakkarNo ratings yet
- Quality of Life of Patients With Scabies: Original ArticleDocument5 pagesQuality of Life of Patients With Scabies: Original ArticlekenNo ratings yet
- Associated Factors of Widespread Pattern of Dermatitis Among Patch Test Population: 12-Year Retrospective StudyDocument6 pagesAssociated Factors of Widespread Pattern of Dermatitis Among Patch Test Population: 12-Year Retrospective StudyDerryAryaPratamaNo ratings yet
- Research: Clinical and Epidemiological Profile of Herpes Zoster A Cross-Sectional Study From Tertiary HospitalDocument6 pagesResearch: Clinical and Epidemiological Profile of Herpes Zoster A Cross-Sectional Study From Tertiary HospitalIntan MirandaNo ratings yet
- Acné Vulgar 2022Document4 pagesAcné Vulgar 2022mirandad784No ratings yet
- CHSJ 46 01 01Document6 pagesCHSJ 46 01 01Dragos AlexandruNo ratings yet
- Keratosis Pilaris and Prevalence of Acne Vulgaris: A Cross-Sectional StudyDocument5 pagesKeratosis Pilaris and Prevalence of Acne Vulgaris: A Cross-Sectional StudyfishalNo ratings yet
- A New Proposed Severity Score For Seborrheic Dermatitis of The F 2017Document1 pageA New Proposed Severity Score For Seborrheic Dermatitis of The F 2017koasspyNo ratings yet
- JCDR 10 WC06Document3 pagesJCDR 10 WC06كنNo ratings yet
- Skin Diseases Among Elderly Attending Out-Patient Dermatologic Clinic, Siriraj HospitalDocument6 pagesSkin Diseases Among Elderly Attending Out-Patient Dermatologic Clinic, Siriraj HospitalenrionickolasNo ratings yet
- ZZZZZZZZZZZZZZDocument8 pagesZZZZZZZZZZZZZZchloramphenicolNo ratings yet
- Mockenhaupt Eemm Sjs TenDocument6 pagesMockenhaupt Eemm Sjs TengratianusbNo ratings yet
- Adjuvant Treatment of Chronic Plaque Psoriasis in Adults by A Herbal Combination: Open German Trial and Review of The LiteratureDocument5 pagesAdjuvant Treatment of Chronic Plaque Psoriasis in Adults by A Herbal Combination: Open German Trial and Review of The LiteratureMini LaksmiNo ratings yet
- Int J Dermatology - 2020 - Araujo - Zika Chikungunya and Dengue Infections As Exacerbating Factors of Psoriasis inDocument3 pagesInt J Dermatology - 2020 - Araujo - Zika Chikungunya and Dengue Infections As Exacerbating Factors of Psoriasis inevelyn.minichNo ratings yet
- Prospective Aetiological Study of Diaper Dermatitis in The ElderlyDocument6 pagesProspective Aetiological Study of Diaper Dermatitis in The ElderlySamuel SammyNo ratings yet
- Large Scale Women AcneDocument11 pagesLarge Scale Women Acneputri.SpANo ratings yet
- Myths, Perceptions and Practices in Acne: A Study On Adolescents and Young AdultsDocument11 pagesMyths, Perceptions and Practices in Acne: A Study On Adolescents and Young AdultsMarie Antoinette VillanuevaNo ratings yet
- Abstracts 853 125: 4 OCTOBER 2005: BackgroundDocument1 pageAbstracts 853 125: 4 OCTOBER 2005: BackgroundkelbmutsNo ratings yet
- Dermatology: Continuing Medical EducationDocument22 pagesDermatology: Continuing Medical EducationCynthia FloraNo ratings yet
- Jamadermatology Kridin 2021 Oi 210045 1634154542.6481Document9 pagesJamadermatology Kridin 2021 Oi 210045 1634154542.6481Nandha KumarNo ratings yet
- Psoriasis FixDocument4 pagesPsoriasis FixDicky SaputraNo ratings yet
- Discoid Lupus Erythematosus: A Profile: Original ArticleDocument4 pagesDiscoid Lupus Erythematosus: A Profile: Original ArticleAngelin LigiantoNo ratings yet
- Knowledge, Attitudes and Practices of The Medical Personnel Regarding Atopic Dermatitis in Yaoundé, CameroonDocument7 pagesKnowledge, Attitudes and Practices of The Medical Personnel Regarding Atopic Dermatitis in Yaoundé, CameroonNadira Juanti PratiwiNo ratings yet
- Jurnal Kortikosteroid Topikal PD WajahDocument4 pagesJurnal Kortikosteroid Topikal PD WajahAnonymous emqfcjJNo ratings yet
- Epidemiology - AK - FinalDocument115 pagesEpidemiology - AK - FinalkarthikNo ratings yet
- Efficacy of Steroidal Vs Non-Steroidal Agents in Oral Lichen Planus: A Randomised, Open-Label StudyDocument9 pagesEfficacy of Steroidal Vs Non-Steroidal Agents in Oral Lichen Planus: A Randomised, Open-Label StudyRetno ManggalihNo ratings yet
- Mall On 2000Document5 pagesMall On 2000Meta SakinaNo ratings yet
- Treatment of Erythrasma: A Double-Blinded Randomized Controlled Trial On The Clinical Application of Clotrimazole and SertaconazoleDocument7 pagesTreatment of Erythrasma: A Double-Blinded Randomized Controlled Trial On The Clinical Application of Clotrimazole and SertaconazoleYuhuu..No ratings yet
- High-Dose Spironolactone For Acne in Patients With Polycystic Ovarian Syndrome - A Single-Institution Retrospective StudyDocument2 pagesHigh-Dose Spironolactone For Acne in Patients With Polycystic Ovarian Syndrome - A Single-Institution Retrospective StudyDaniella TruffelloNo ratings yet
- Characterization of Acne Associated With UpadacitiDocument8 pagesCharacterization of Acne Associated With UpadacitiDo u know BTS?No ratings yet
- Review: Management of AcneDocument4 pagesReview: Management of AcneAldaniaNo ratings yet
- 32 01 09 GrazinaDocument16 pages32 01 09 GrazinaDisty ANo ratings yet
- Jurnal Kulit PDFDocument4 pagesJurnal Kulit PDFAidarnaWanSariNo ratings yet
- Class 1 - 032024Document98 pagesClass 1 - 032024Viet HungNo ratings yet
- Acne Vulgaris: Clinical PracticeDocument18 pagesAcne Vulgaris: Clinical PracticeSonia Dwi Reina TumanggorNo ratings yet
- Jurnal AcneDocument7 pagesJurnal AcneChairizal Meiristica YanhaNo ratings yet
- Treatment of Scabies: Comparison of Permethrin 5% Versus IvermectinDocument4 pagesTreatment of Scabies: Comparison of Permethrin 5% Versus IvermectinWilliam WijayaNo ratings yet
- Comparative Study of Two Topical Therapies in Acne - Benzoyl Peroxide (2.5%) & Retinoic Acid (0.025%)Document4 pagesComparative Study of Two Topical Therapies in Acne - Benzoyl Peroxide (2.5%) & Retinoic Acid (0.025%)manish agrawalNo ratings yet
- Clinical Features of Thyroid Cancer in Paediatric Age Experience of A Tertiary Centre in The 2000 2020 PeriodDocument8 pagesClinical Features of Thyroid Cancer in Paediatric Age Experience of A Tertiary Centre in The 2000 2020 PeriodAlin VázquezNo ratings yet
- Kalb 2009Document5 pagesKalb 2009Sajid Hussain ShahNo ratings yet
- Risk Factor TaiwanDocument5 pagesRisk Factor TaiwanMira ApriliaNo ratings yet
- Analysis of Clinical Efficacy, Sideeffects, and Laboratory Changesamong Patients With Acnevulgaris Receiving Single Versustwice Daily Dose Oforal IsotretinoinDocument7 pagesAnalysis of Clinical Efficacy, Sideeffects, and Laboratory Changesamong Patients With Acnevulgaris Receiving Single Versustwice Daily Dose Oforal IsotretinoinKadir KUCUKNo ratings yet
- Hodgkin Lymphoma: A Comprehensive OverviewFrom EverandHodgkin Lymphoma: A Comprehensive OverviewAndreas EngertNo ratings yet
- Jurnal Pcos InternationalDocument5 pagesJurnal Pcos InternationalPuput Anistiya Hariani100% (1)
- 6 - Contemporary Management of Polycystic Ovarian Syndrome - 2019Document11 pages6 - Contemporary Management of Polycystic Ovarian Syndrome - 2019Johanna Bustos NutricionistaNo ratings yet
- Hidradenitis Suppurativa: A Guide For The Practicing PhysicianDocument15 pagesHidradenitis Suppurativa: A Guide For The Practicing Physiciandavid carsNo ratings yet
- Sign of Hyperandrogenism PDFDocument6 pagesSign of Hyperandrogenism PDFmisbah_mdNo ratings yet
- Crash Course - General PharmacologyDocument62 pagesCrash Course - General PharmacologyDhanesh VijayaraghavanNo ratings yet
- The Management of Polycystic Ovary Syndrome: Vincenza Bruni, Metella Dei, Valentina Pontello, and Paolo VangelistiDocument15 pagesThe Management of Polycystic Ovary Syndrome: Vincenza Bruni, Metella Dei, Valentina Pontello, and Paolo VangelistiDaniela UrreaNo ratings yet
- Bp503t Pcol Unit-VDocument46 pagesBp503t Pcol Unit-VAakkkNo ratings yet
- CPM14th PCOS PDFDocument9 pagesCPM14th PCOS PDFJapheth SalvanNo ratings yet
- ProstateDocument42 pagesProstateMegawati Abubakar100% (1)
- Degarelix (SQ) : Flutamide, BicalutamideDocument5 pagesDegarelix (SQ) : Flutamide, BicalutamideGregNo ratings yet
- Drug List WordDocument33 pagesDrug List Wordd clarkeNo ratings yet
- Male Androgens PDFDocument17 pagesMale Androgens PDFGreg RalphNo ratings yet
- Banogon - Androgens and Anti-Androgens PDFDocument57 pagesBanogon - Androgens and Anti-Androgens PDFMary Angelique BanogonNo ratings yet
- Telephone ScatologiaDocument5 pagesTelephone ScatologiaEdaNo ratings yet
- 09 Prostate Cancer 2017 WebDocument146 pages09 Prostate Cancer 2017 WebDharmesh PatelNo ratings yet
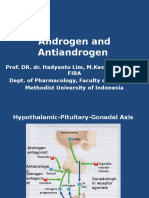
- Androgen and AntiandrogenDocument18 pagesAndrogen and AntiandrogenIrma MarianyNo ratings yet
- Metabolic & Endocrine Drugs: Dr. Gitau ChegeDocument29 pagesMetabolic & Endocrine Drugs: Dr. Gitau ChegeClexNo ratings yet
- 09 Prostate Cancer LRDocument137 pages09 Prostate Cancer LRDonna WilliamsNo ratings yet
- Sem 16 Lectura 1 AnticoncepcionDocument29 pagesSem 16 Lectura 1 AnticoncepcionEnrique Moncada MapelliNo ratings yet
- Journal of The Student National Medical Association-Winter 2012Document40 pagesJournal of The Student National Medical Association-Winter 2012Erin JoëlNo ratings yet
- Fpgee Study Guide GurudattaDocument31 pagesFpgee Study Guide GurudattaWINSOMETAB33% (3)
- Gonadal Hormones and InhibitorsDocument101 pagesGonadal Hormones and Inhibitors2012100% (4)
- Guidelines Acne VulgarisDocument14 pagesGuidelines Acne VulgarisKym DominguezNo ratings yet
- Endocrine UnlockedDocument30 pagesEndocrine Unlockedelsharkaoui211No ratings yet
- Pcol MidtermsDocument13 pagesPcol MidtermsJoyce VillanuevaNo ratings yet
- Eau Eanm Estro Esur Isup Siog Guidelines On Prostate CancerDocument212 pagesEau Eanm Estro Esur Isup Siog Guidelines On Prostate CancerZahraNo ratings yet
- CancerMPact 2023 TA US Prostate v1.1Document197 pagesCancerMPact 2023 TA US Prostate v1.1NIrmalya SenguptaNo ratings yet
- PCOSDocument15 pagesPCOSAndyan Adlu PrasetyajiNo ratings yet
- C40 The Gonadal Hormones & Inhibitors: Anita Q. Sangalang, MD, Mhped, Fpogs Faculty of Pharmacy University of Santo TomasDocument7 pagesC40 The Gonadal Hormones & Inhibitors: Anita Q. Sangalang, MD, Mhped, Fpogs Faculty of Pharmacy University of Santo TomasHydieNo ratings yet