You might also like
- Application For Admission: Please Note: This Entire Form Is To Be Completed by The Applicant. Please Print ClearlyDocument3 pagesApplication For Admission: Please Note: This Entire Form Is To Be Completed by The Applicant. Please Print ClearlyJanuhu ZakaryNo ratings yet
- Complete This Form and Submit To: UNCSA, Office of Student Financial Aid, 1533 South Main Street, Winston-Salem, NC 27127Document1 pageComplete This Form and Submit To: UNCSA, Office of Student Financial Aid, 1533 South Main Street, Winston-Salem, NC 27127Diego Vazquez-GomezNo ratings yet
- FmRteO-Self Declaration Fillable Form - FINAL For WebsiteDocument2 pagesFmRteO-Self Declaration Fillable Form - FINAL For Websitejqyzgbyq2nNo ratings yet
- How To Request Your Covid - 19 Lab Report: Complete The Consent To Disclose Phi FormDocument3 pagesHow To Request Your Covid - 19 Lab Report: Complete The Consent To Disclose Phi FormAnithasree SrinivasanNo ratings yet
- CHU Application FormDocument4 pagesCHU Application FormJumie SamsudinNo ratings yet
- Secondary Application Form Fall 2013 Entering Class: Mahmood MadihaDocument2 pagesSecondary Application Form Fall 2013 Entering Class: Mahmood MadihaSumaya MahmoodNo ratings yet
- Authorization Form For Researchers The Use and Disclosure of PHIDocument2 pagesAuthorization Form For Researchers The Use and Disclosure of PHImatiushynsNo ratings yet
- Exemption From Immunizations Form 3-23-23Document2 pagesExemption From Immunizations Form 3-23-23Safeer UllahNo ratings yet
- Aimhighapp 2015Document5 pagesAimhighapp 2015api-290166419No ratings yet
- JJHI Enrollment ApplicationDocument1 pageJJHI Enrollment ApplicationLyric LoveNo ratings yet
- F-1 International Student Advisor Report Form: (Please Print)Document1 pageF-1 International Student Advisor Report Form: (Please Print)huynhnhuthuy181No ratings yet
- Andy Anderson, M.A., PLPC 2850 West Clay, Suite 255 Saint Charles, MO 63301 Phone: (636) 699-0872 FAX: (636) 625-0839Document1 pageAndy Anderson, M.A., PLPC 2850 West Clay, Suite 255 Saint Charles, MO 63301 Phone: (636) 699-0872 FAX: (636) 625-0839api-55970082No ratings yet
- ED - Cert.formDocument1 pageED - Cert.formNaura Aisy MardianaNo ratings yet
- Dube Trade Port Application FormDocument7 pagesDube Trade Port Application FormNcediswaNo ratings yet
- Scholarship Application Updated 120813Document4 pagesScholarship Application Updated 120813api-221470498No ratings yet
- JDLLM Fall 2022 ApplicationDocument2 pagesJDLLM Fall 2022 Applicationsonukakandhe007No ratings yet
- The College of Saint Rose Housing Accommodation and Meal Plan Waiver Request FormDocument3 pagesThe College of Saint Rose Housing Accommodation and Meal Plan Waiver Request FormsaintrosechronicleNo ratings yet
- Authorisation Form: To Be Picked Up: - )Document1 pageAuthorisation Form: To Be Picked Up: - )Amir MohammedNo ratings yet
- NMTC Application Form FinalDocument5 pagesNMTC Application Form FinalicttumainiNo ratings yet
- Patient Demographics 12-12-12Document4 pagesPatient Demographics 12-12-12api-233056868No ratings yet
- Griffin Observership ApplicationDocument7 pagesGriffin Observership Applicationসোমনাথ মহাপাত্রNo ratings yet
- The Almighty Latin King & Queen Nation: College Application Fee Waver Letter of RecommendationDocument4 pagesThe Almighty Latin King & Queen Nation: College Application Fee Waver Letter of RecommendationNicolas PerezNo ratings yet
- Clinical Volunteer ApplicationDocument3 pagesClinical Volunteer ApplicationAnonymous tS0WWCCNo ratings yet
- Application Deferral Request FormDocument1 pageApplication Deferral Request FormYasir AyubNo ratings yet
- The Guy and Gloria Muto: Memorial Scholarship Foundation, IncDocument3 pagesThe Guy and Gloria Muto: Memorial Scholarship Foundation, IncLeo HarmonNo ratings yet
- Juvenile Justice Corps 2010-2011 ApplicationDocument4 pagesJuvenile Justice Corps 2010-2011 ApplicationCHCMCblog4085No ratings yet
- Greenleaf Application English 2024-2025Document5 pagesGreenleaf Application English 2024-2025Andre PagliariniNo ratings yet
- Certification Application Via Institutional RecommendationDocument1 pageCertification Application Via Institutional RecommendationBilal SalaamNo ratings yet
- Walton Student Application FormDocument7 pagesWalton Student Application FormRicardo Luis Salgado AraujoNo ratings yet
- Willits Otters Swim Team ApplicationDocument2 pagesWillits Otters Swim Team Applicationapi-423839129No ratings yet
- Phlebotomy Tech FormDocument4 pagesPhlebotomy Tech FormHawaiiHealthCareNo ratings yet
- Confirmation of Resources - New FormatDocument1 pageConfirmation of Resources - New FormatNagendra SettyNo ratings yet
- Intensive English Program: IEP Admission FormDocument1 pageIntensive English Program: IEP Admission FormwesamNo ratings yet
- Common App Secondary School ReportDocument5 pagesCommon App Secondary School Reportelica81topsNo ratings yet
- Brother and Sister:: Scholarships and Financial Assistance Division Office of Student Affairs UPLB, College, LagunaDocument2 pagesBrother and Sister:: Scholarships and Financial Assistance Division Office of Student Affairs UPLB, College, LagunaAnnabella LacunaNo ratings yet
- UNL Financial ResourceDocument2 pagesUNL Financial ResourceKofi AmoakoNo ratings yet
- Long Course RegistrationDocument1 pageLong Course RegistrationCFYN TigersharksNo ratings yet
- F-ADM-001 Rev.1 (11!10!2023) Application For Admission FormDocument3 pagesF-ADM-001 Rev.1 (11!10!2023) Application For Admission Formsuyojhonlester15No ratings yet
- Kundalini Research Institute: The Aquarian Teacher™Document3 pagesKundalini Research Institute: The Aquarian Teacher™Diana TrNo ratings yet
- 查證學歷授權書 美國學歷Document1 page查證學歷授權書 美國學歷Lan SoNo ratings yet
- Free Job Application Form - Standard TemplateDocument3 pagesFree Job Application Form - Standard TemplateMark MartinezNo ratings yet
- Verification-Adhd-Psych-2020 (1) - 211108 - 095107Document3 pagesVerification-Adhd-Psych-2020 (1) - 211108 - 095107Stephan ChiariniNo ratings yet
- Applicationb IIDocument7 pagesApplicationb IIreload99No ratings yet
- Subject: Application For Appointment As CtiDocument1 pageSubject: Application For Appointment As CtiTahir MehmoodNo ratings yet
- 2011-2012 ACE ScholarshipDocument6 pages2011-2012 ACE ScholarshipNakhtet Netchemu SekhetetNo ratings yet
- Hipaa Journal Hipaa Release Form v1Document3 pagesHipaa Journal Hipaa Release Form v1pialee royNo ratings yet
- Native Vision Scholarship: Applications Must Be Received To Ms. Hammen by May 7, 2010 at 5pm (EDT)Document5 pagesNative Vision Scholarship: Applications Must Be Received To Ms. Hammen by May 7, 2010 at 5pm (EDT)api-25945993No ratings yet
- SSC Admision Form 2021 2022Document1 pageSSC Admision Form 2021 2022Duedate AgapitoNo ratings yet
- SwimmingPool Membership FormDocument1 pageSwimmingPool Membership FormSrujana MohantyNo ratings yet
- Application For Admission: Virginia State PoliceDocument5 pagesApplication For Admission: Virginia State PoliceRoiji MaripNo ratings yet
- Mifflintown Hose Co. #1: Volunteer ApplicationDocument8 pagesMifflintown Hose Co. #1: Volunteer ApplicationKeith H. BoremanNo ratings yet
- Last First Middle InitialDocument3 pagesLast First Middle InitialAsjsjsjsNo ratings yet
- CSH - Patient Access To Their Protected Health Information Form 5.28.21 2Document2 pagesCSH - Patient Access To Their Protected Health Information Form 5.28.21 2staciejason538No ratings yet
- Uprising Medical Release FormDocument1 pageUprising Medical Release Formone dollar youth ministryNo ratings yet
- Authoriazation FormDocument2 pagesAuthoriazation FormQianchen ChenNo ratings yet
- TUE - WADA Version 2016-EnDocument4 pagesTUE - WADA Version 2016-EnYannick MOSSUSNo ratings yet
- ADEN - EP Student Evaluation Request 2021 Student LifeDocument2 pagesADEN - EP Student Evaluation Request 2021 Student LifeAll CastilloNo ratings yet
- Teen MedicalDocument1 pageTeen MedicalJohn C StarkNo ratings yet
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- Nondegree-Student-Application-Instructions 2023-2024 - For-WebDocument4 pagesNondegree-Student-Application-Instructions 2023-2024 - For-WebMoushumNo ratings yet
- Domestic Application 23-24 508Document13 pagesDomestic Application 23-24 508MoushumNo ratings yet
- International Student Financial Sponsor FormDocument1 pageInternational Student Financial Sponsor FormMoushumNo ratings yet
- Undergraduate Degree Programs 2023 2024Document3 pagesUndergraduate Degree Programs 2023 2024MoushumNo ratings yet
- Fiverr Community LeaderDocument4 pagesFiverr Community LeaderMoushumNo ratings yet
- School Counselor FormDocument1 pageSchool Counselor FormMoushumNo ratings yet
- Pochettino Backs Messi To Rediscover Form in Front of GoalDocument5 pagesPochettino Backs Messi To Rediscover Form in Front of GoalMoushumNo ratings yet
- Juventus Say Prosecutors Looking Into Terms of Ronaldo SaleDocument5 pagesJuventus Say Prosecutors Looking Into Terms of Ronaldo SaleMoushumNo ratings yet
- Messi After Seventh Ballon D'or WinDocument5 pagesMessi After Seventh Ballon D'or WinMoushumNo ratings yet
- Solnchap 07Document48 pagesSolnchap 07api-3701823No ratings yet
- Affidavit of Co-OwnershipDocument2 pagesAffidavit of Co-OwnershipStarr Jularbal-Docena75% (12)
- The Justinian Law CorrectDocument4 pagesThe Justinian Law CorrectRajnish PrakashNo ratings yet
- Membership of School Council: NotificationDocument4 pagesMembership of School Council: NotificationAasif NawazNo ratings yet
- Moot Court ExerciseDocument34 pagesMoot Court ExercisePreeti ShuklaNo ratings yet
- How To Study LawDocument55 pagesHow To Study LawAnas AliNo ratings yet
- Automotive Industry Workers Alliance Vs RomuloDocument8 pagesAutomotive Industry Workers Alliance Vs RomuloRelmie TaasanNo ratings yet
- AOA Pragya ReadableDocument12 pagesAOA Pragya Readablerajesh KumarNo ratings yet
- Resolution No. 10717Document7 pagesResolution No. 10717Kat AtienzaNo ratings yet
- RIZAL-REVIEWER-finalDocument14 pagesRIZAL-REVIEWER-finalPrincessNo ratings yet
- Maritime CollisionDocument5 pagesMaritime CollisionSinh TranNo ratings yet
- NBCDO Memo Circular No.01 Series of 2005Document2 pagesNBCDO Memo Circular No.01 Series of 2005Roland CepedaNo ratings yet
- SDG&E Letter To City Attorney Saying No 1-Year Extension On Franchise AgreementDocument2 pagesSDG&E Letter To City Attorney Saying No 1-Year Extension On Franchise AgreementRob NikolewskiNo ratings yet
- Caltex (Philippines), Inc. v. Palomar, G.R. No. L-19650, (September 29, 1966), 124 PHIL 763-781Document6 pagesCaltex (Philippines), Inc. v. Palomar, G.R. No. L-19650, (September 29, 1966), 124 PHIL 763-781aisea patrickNo ratings yet
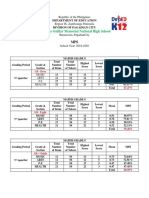
- Norberta Guillar Memorial National High School: Department of Education Division of Pagadian CityDocument3 pagesNorberta Guillar Memorial National High School: Department of Education Division of Pagadian CityJustice Gee SumampongNo ratings yet
- Subject: Family Law - Ii Subjct Code: HWJDocument2 pagesSubject: Family Law - Ii Subjct Code: HWJutkarsh gargNo ratings yet
- PRI'SDocument14 pagesPRI'SAbhidhaNo ratings yet
- Moot Diary oDocument17 pagesMoot Diary oHanu MittalNo ratings yet
- Constitution Comparison SheetDocument2 pagesConstitution Comparison SheetKileeshaNo ratings yet
- Eo Tanod BrigadeDocument7 pagesEo Tanod Brigadegines miagaoNo ratings yet
- Condonation of DelayDocument7 pagesCondonation of DelayMandla & Singh Law ChambersNo ratings yet
- Self Declaration of Surviving SpouseDocument1 pageSelf Declaration of Surviving SpouseSanchez ShekahNo ratings yet
- Statement of PurposeDocument3 pagesStatement of PurposeAnusha Nagavarapu100% (1)
- Curro PolicyDocument2 pagesCurro PolicySamson NherudzoNo ratings yet
- On-Line Application For Single Window Operator (Swo) : Registration #: 3146857 Full Name: Rahul Chandra KholiyaDocument3 pagesOn-Line Application For Single Window Operator (Swo) : Registration #: 3146857 Full Name: Rahul Chandra KholiyaRahul KholiyaNo ratings yet
- Guided Reading Activity - Nation Building in Latin AmericaDocument2 pagesGuided Reading Activity - Nation Building in Latin AmericaTomas MongeNo ratings yet
- Uy vs. Court of AppealsDocument4 pagesUy vs. Court of AppealsCarla DomingoNo ratings yet
- Sample Bequest ClausesDocument1 pageSample Bequest ClausesAlanNo ratings yet
- Contract - Case LawDocument9 pagesContract - Case Lawasain016No ratings yet
- Brief FactsDocument29 pagesBrief FactsBahadur AliNo ratings yet
- Usdaw Activist 120Document2 pagesUsdaw Activist 120USDAWactivistNo ratings yet