You might also like
- List of Laws, EOs, AOs, MCS, and BCsDocument1 pageList of Laws, EOs, AOs, MCS, and BCsJarena Ria Zolina100% (2)
- USUHS Anesthesia Pharmacology NotesetDocument247 pagesUSUHS Anesthesia Pharmacology NotesetSean Bancroft100% (3)
- Pre Medications AnaesthesiaDocument34 pagesPre Medications AnaesthesiastadolinNo ratings yet
- Pharmacology For Nurses: A Pathophysiologic Approach: Fifth EditionDocument51 pagesPharmacology For Nurses: A Pathophysiologic Approach: Fifth Editionadni_wgNo ratings yet
- Guidelines For RituximabDocument9 pagesGuidelines For RituximabMonica MonikaNo ratings yet
- Enoxaparin Drug StudyDocument2 pagesEnoxaparin Drug StudyRohannah D. MalawadNo ratings yet
- Guidelines For The Advertisement of Drugs, Herbal Medicines, Cosmetics, Medical Devices & Household ChemicalsDocument8 pagesGuidelines For The Advertisement of Drugs, Herbal Medicines, Cosmetics, Medical Devices & Household ChemicalssboaduappiahNo ratings yet
- 2 - Introduction To PharmacovigilanceDocument28 pages2 - Introduction To PharmacovigilanceHanan AhmedNo ratings yet
- Perencaan Anggaran BMHP Dan Obat Di RSPK 2022 FixDocument51 pagesPerencaan Anggaran BMHP Dan Obat Di RSPK 2022 FixlaelaNo ratings yet
- Diagnosis and Management of Treatment Refractory HypothyroidismDocument17 pagesDiagnosis and Management of Treatment Refractory HypothyroidismMerlyn AngelinaNo ratings yet
- TROPiCS-02 - JCO 2022Document16 pagesTROPiCS-02 - JCO 2022Nicola CrestiNo ratings yet
- Developing A Clinically Important Class of Glycan-Targeted Biologics With Unprecedented Tumor Specificity Funding First Human DataDocument17 pagesDeveloping A Clinically Important Class of Glycan-Targeted Biologics With Unprecedented Tumor Specificity Funding First Human DataNuno Prego RamosNo ratings yet
- The Clinical Impacts of Molecular Subtyping by Multigene Assay On Hormone Receptor-Positive Breast CancersDocument7 pagesThe Clinical Impacts of Molecular Subtyping by Multigene Assay On Hormone Receptor-Positive Breast Cancers郭竹瑩No ratings yet
- Trastuzumab Deruxtecan in Previously Treated HER2-Positive Breast CancerDocument12 pagesTrastuzumab Deruxtecan in Previously Treated HER2-Positive Breast CancerRocio SolervicensNo ratings yet
- 1758834016665077Document21 pages1758834016665077Yohanes AdinugrohoNo ratings yet
- The Breast: SciencedirectDocument9 pagesThe Breast: SciencedirectFrengky MaweaNo ratings yet
- Keynote 355Document10 pagesKeynote 355Rocio SolervicensNo ratings yet
- Triple Negative Breast Cancer Current PerspectiveDocument7 pagesTriple Negative Breast Cancer Current PerspectivenagarajharishNo ratings yet
- Bi Omar CadresDocument33 pagesBi Omar CadresNataly Butrón BustamanteNo ratings yet
- New England Journal Medicine: The ofDocument9 pagesNew England Journal Medicine: The ofAndersson SaenzNo ratings yet
- 10 1200@jco 20 00184Document13 pages10 1200@jco 20 00184faris nagibNo ratings yet
- BCTT 287320 Triple Negative Breast Cancer Assessing The Role of ImmunohDocument14 pagesBCTT 287320 Triple Negative Breast Cancer Assessing The Role of ImmunohAparicio Aguilar ValesNo ratings yet
- Cytoplasmic Maspin Expression Predicts Poor Prognosis of Patients With Soft Tissue SarcomasDocument7 pagesCytoplasmic Maspin Expression Predicts Poor Prognosis of Patients With Soft Tissue SarcomasAndreea RelenschiNo ratings yet
- Molecular Immunology: in Silico Analysis of Transmembrane Protein 31 (TMEM31) Antigen To DesignDocument10 pagesMolecular Immunology: in Silico Analysis of Transmembrane Protein 31 (TMEM31) Antigen To DesignDr. Kaushal Kishor SharmaNo ratings yet
- Cancers 1316412Document21 pagesCancers 1316412antoinegoisnardNo ratings yet
- Current Therapies For Human Epidermal Growth Factor Receptor 2-Positive Metastatic Breast Cancer PatientsDocument17 pagesCurrent Therapies For Human Epidermal Growth Factor Receptor 2-Positive Metastatic Breast Cancer PatientsmrsilNo ratings yet
- Jurnal 1 Kelompok 9Document17 pagesJurnal 1 Kelompok 9hy brezzleNo ratings yet
- Ijwh 178349 Triple Negative Breast Cancer Current Perspective On The EvDocument7 pagesIjwh 178349 Triple Negative Breast Cancer Current Perspective On The EvMuhammad FauzanNo ratings yet
- Synchronous Bilateral Breast Cancer Right Her 2 Positive and Left Her 2 Negetive - A Case ReportDocument6 pagesSynchronous Bilateral Breast Cancer Right Her 2 Positive and Left Her 2 Negetive - A Case ReportIJAR JOURNALNo ratings yet
- CLM94, A Novel Cyclic Amide With Anti-VEGFR-2 and Antiangiogenic Properties, Is Active Against Primary Anaplastic Thyroid Cancer in Vitro and in VivoDocument9 pagesCLM94, A Novel Cyclic Amide With Anti-VEGFR-2 and Antiangiogenic Properties, Is Active Against Primary Anaplastic Thyroid Cancer in Vitro and in VivoAndreas KrishnaputraNo ratings yet
- Annals of Diagnostic Pathology: Gerard Nuovo, MDDocument6 pagesAnnals of Diagnostic Pathology: Gerard Nuovo, MDamelia zettaNo ratings yet
- The Examiner of Alternative MedicineDocument4 pagesThe Examiner of Alternative MedicineLee Ming HinNo ratings yet
- Pembrolizumab For Persistent, Recurrent, or Metastatic Carvical CancerDocument12 pagesPembrolizumab For Persistent, Recurrent, or Metastatic Carvical CancerluizaNo ratings yet
- Spatial Phenotypic Signatures:: Novel Biomarker Class For Predicting Immunotherapy OutcomesDocument7 pagesSpatial Phenotypic Signatures:: Novel Biomarker Class For Predicting Immunotherapy Outcomeseri yantoNo ratings yet
- The Evolving Role of Immunotherapy As A Component of Multimodal Therapy in Earlier Stages of Lung CancerDocument59 pagesThe Evolving Role of Immunotherapy As A Component of Multimodal Therapy in Earlier Stages of Lung CancerRiya ChaturvediNo ratings yet
- A Novel Triple Therapy For ITP Using Hgh-Dose Dexamethasone, Low Dose Rituximab, and Cyclosporine (TT4)Document5 pagesA Novel Triple Therapy For ITP Using Hgh-Dose Dexamethasone, Low Dose Rituximab, and Cyclosporine (TT4)AdiNo ratings yet
- Luthra2021 Article RoleOfDifferentPeptidesForCancDocument17 pagesLuthra2021 Article RoleOfDifferentPeptidesForCancAkdicmsNo ratings yet
- Advancing Rare Disease Treatment EMAs Decade-LongDocument13 pagesAdvancing Rare Disease Treatment EMAs Decade-Longilum.rononNo ratings yet
- Destiny O4Document12 pagesDestiny O4ΒΑΣΙΛΗΣ ΚΟΛΙΝΤΖΙΚΗΣNo ratings yet
- Biomarkers HER2+ MBCDocument30 pagesBiomarkers HER2+ MBChiroshima123No ratings yet
- Keynote 048Document14 pagesKeynote 048brenomendespNo ratings yet
- 20-07-2020 025934231 - Bcl-2Document11 pages20-07-2020 025934231 - Bcl-2Mohammad Ahmad SharroufNo ratings yet
- Biologia Futura Emerging Antigen-Specific Therapies For Autoimmune DiseasesDocument10 pagesBiologia Futura Emerging Antigen-Specific Therapies For Autoimmune DiseasesAleksandar MilanovicNo ratings yet
- Dong Et Al 2022 - Nanoparticles (NPS) - Mediated Systemic mRNA Delivery To Reverse Trastuzumab Resistance For Effective Breast Cancer TherapyDocument12 pagesDong Et Al 2022 - Nanoparticles (NPS) - Mediated Systemic mRNA Delivery To Reverse Trastuzumab Resistance For Effective Breast Cancer TherapySazid AhmadNo ratings yet
- Effect of Oncoxin Oral Solution in HER2-Overexpressing Breast CancerDocument12 pagesEffect of Oncoxin Oral Solution in HER2-Overexpressing Breast Cancerleonaldy sintesahealthNo ratings yet
- In Vitro and in Vivo Study of The Effect of Osteogenic Pulsed Electromagnetic Fields On Breast and Lung Cancer CellsDocument13 pagesIn Vitro and in Vivo Study of The Effect of Osteogenic Pulsed Electromagnetic Fields On Breast and Lung Cancer CellsVictorNo ratings yet
- Hou 2019Document8 pagesHou 2019Carlita Cari CclNo ratings yet
- Tachira P Paper ADC Breast Cancer-1 PDFDocument17 pagesTachira P Paper ADC Breast Cancer-1 PDFZeddicus Zu'l ZoranderNo ratings yet
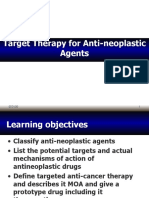
- 7.4 - Targeted Therapy - Anti-Neoplastic Agents Dec2013-Dec2015-1Document14 pages7.4 - Targeted Therapy - Anti-Neoplastic Agents Dec2013-Dec2015-1Gabrielle NnomoNo ratings yet
- cbl5 q9Document19 pagescbl5 q9洪嘉敏No ratings yet
- Fonc 08 00086Document14 pagesFonc 08 00086Siska HarapanNo ratings yet
- Ijms 24 02542Document3 pagesIjms 24 02542Frank MacíasNo ratings yet
- Swain2019 Article PathologicCompleteResponseAndODocument11 pagesSwain2019 Article PathologicCompleteResponseAndOJeevan SunaNo ratings yet
- 2021 LAT1 Is Associated With Chemoresistance in Breast Cancer Via The Promotion of Amino Acid MetabolismDocument11 pages2021 LAT1 Is Associated With Chemoresistance in Breast Cancer Via The Promotion of Amino Acid Metabolismarifudin_achmadNo ratings yet
- Pharmacokinetics and in Vitro/in Vivo Antitumor Efficacy of Aptamer-Targeted Ecoflex Nanoparticles For Docetaxel Delivery in Ovarian CancerDocument13 pagesPharmacokinetics and in Vitro/in Vivo Antitumor Efficacy of Aptamer-Targeted Ecoflex Nanoparticles For Docetaxel Delivery in Ovarian CancerFranc DechiaNo ratings yet
- CNS Met From HER2+ BCDocument27 pagesCNS Met From HER2+ BChiroshima123No ratings yet
- An Unbiased Oncology Compound Screen To Identify Novel Combination StrategiesDocument9 pagesAn Unbiased Oncology Compound Screen To Identify Novel Combination StrategiesBobNo ratings yet
- CDK Luminal ABCDocument85 pagesCDK Luminal ABCSusanto SalimNo ratings yet
- Callus 2017Document6 pagesCallus 2017chemistpl420No ratings yet
- Biomedicines: Recent Progress and Advances in HGF/MET-Targeted Therapeutic Agents For Cancer TreatmentDocument33 pagesBiomedicines: Recent Progress and Advances in HGF/MET-Targeted Therapeutic Agents For Cancer Treatmentanahh ramakNo ratings yet
- Cas 14835Document12 pagesCas 14835Sediki ZakariaNo ratings yet
- Abstracts: Annals of OncologyDocument1 pageAbstracts: Annals of OncologyAsaikkutti AnnamalaiNo ratings yet
- Tucatinib, Trastuzumab, and Capecitabine For HER2-Positive Metastatic Breast CancerDocument13 pagesTucatinib, Trastuzumab, and Capecitabine For HER2-Positive Metastatic Breast Cancertpatel0986No ratings yet
- Articles: BackgroundDocument11 pagesArticles: BackgroundOncología CdsNo ratings yet
- Kinase Inhibitors Increase Individual Radiation Sensitivity in Normal Cells of Cancer PatientsDocument11 pagesKinase Inhibitors Increase Individual Radiation Sensitivity in Normal Cells of Cancer Patientsyuta titeNo ratings yet
- Impower 132Document12 pagesImpower 132linxiaNo ratings yet
- New Treatment Options For Metastatic Thyroid CancerDocument6 pagesNew Treatment Options For Metastatic Thyroid CancermarcelinaNo ratings yet
- (In Vivo) 6823520Document11 pages(In Vivo) 6823520ingelitaNo ratings yet
- Antiangiogenic and Antitumoral Effects Mediated by ADocument10 pagesAntiangiogenic and Antitumoral Effects Mediated by AMiss AmyNo ratings yet
- Tumor Immune Microenvironment in Cancer Progression and Cancer TherapyFrom EverandTumor Immune Microenvironment in Cancer Progression and Cancer TherapyPawel KalinskiNo ratings yet
- CNS Met From HER2+ BCDocument27 pagesCNS Met From HER2+ BChiroshima123No ratings yet
- CDK4 - 6i ResistanceDocument40 pagesCDK4 - 6i Resistancehiroshima123No ratings yet
- Biomarkers HER2+ MBCDocument30 pagesBiomarkers HER2+ MBChiroshima123No ratings yet
- Adj Anthral TNBCDocument35 pagesAdj Anthral TNBChiroshima123No ratings yet
- Oral Pharmacology - For The Dental HygienistDocument358 pagesOral Pharmacology - For The Dental HygienistIvan GeorgievNo ratings yet
- Janssen Latam: Ash 2023 Congress GuidebookDocument56 pagesJanssen Latam: Ash 2023 Congress GuidebookmelainehematoNo ratings yet
- BLS Healthcare Provider AlgorithmDocument7 pagesBLS Healthcare Provider AlgorithmyuniNo ratings yet
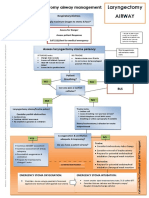
- Laryngectomy Airway: Emergency Tracheostomy Airway ManagementDocument1 pageLaryngectomy Airway: Emergency Tracheostomy Airway ManagementDana IlieNo ratings yet
- Safe Injection and Infusion Practices TraningDocument4 pagesSafe Injection and Infusion Practices TraningPRADIPNo ratings yet
- Data Obat HormonDocument74 pagesData Obat HormonWizzyAsklepiosNo ratings yet
- Pharmacology - Respiratory DrugsDocument3 pagesPharmacology - Respiratory DrugsTiffany AdriasNo ratings yet
- Times 2003Document222 pagesTimes 2003tazman123No ratings yet
- MARCH 23bills TALLY OUTSTANDING RECEIVABLE LIST 06.03.2023Document12 pagesMARCH 23bills TALLY OUTSTANDING RECEIVABLE LIST 06.03.2023radha gNo ratings yet
- Comparison of Acute Lethal Toxicity of CommonlyDocument11 pagesComparison of Acute Lethal Toxicity of Commonlybencleese100% (1)
- Principles of Drug ActionDocument42 pagesPrinciples of Drug ActionkjghlkdfjgNo ratings yet
- Definition of BiopharmaceuticsDocument3 pagesDefinition of BiopharmaceuticsvafaashkNo ratings yet
- PHL 313 Pharmacology 1st St. NEWDocument6 pagesPHL 313 Pharmacology 1st St. NEWALNAKINo ratings yet
- (P3) Perhitungan Resep KemoterapiDocument28 pages(P3) Perhitungan Resep KemoterapiRESI JULIANANo ratings yet
- Silberstein 2015Document17 pagesSilberstein 2015chrisantyNo ratings yet
- AsthmaDocument6 pagesAsthmaMicky SunnyrajNo ratings yet
- HRNBL1-ESIOP Protocol Anglais Amendement4 Juillet2009Document303 pagesHRNBL1-ESIOP Protocol Anglais Amendement4 Juillet2009Bianca Alexandra100% (1)
- Price ListDocument38 pagesPrice ListERVINTIANo ratings yet
- Copy of ALKES AKTIF DI LOGISTIK 20191104 - Item Movement CatDocument70 pagesCopy of ALKES AKTIF DI LOGISTIK 20191104 - Item Movement Catama tagiNo ratings yet
- Kelompok 10 - Metode Optimasi Senyawa PenuntunDocument36 pagesKelompok 10 - Metode Optimasi Senyawa Penuntunapr_aprililianti100% (1)