You might also like
- UW Notes - 5 - PharmacologyDocument12 pagesUW Notes - 5 - PharmacologyDarshi BNo ratings yet
- 2ND To The Last SeshDocument25 pages2ND To The Last SeshnivraeNo ratings yet
- EPOPROSTENOLDocument6 pagesEPOPROSTENOLMavy CantonNo ratings yet
- Drug Study Arthritis DrugDocument9 pagesDrug Study Arthritis DrugIrene Grace BalcuevaNo ratings yet
- LiverTox: Clinical and Research Information On Drug-Induced Liver Injury - AcetaminophenDocument41 pagesLiverTox: Clinical and Research Information On Drug-Induced Liver Injury - AcetaminophenJessica AristaNo ratings yet
- Analgesic Agents: Maya Ganda Ratna Department of Pharmacology and Pharmacy Faculty of Medicine - Lampung UniversityDocument46 pagesAnalgesic Agents: Maya Ganda Ratna Department of Pharmacology and Pharmacy Faculty of Medicine - Lampung UniversityMuhammad GilangNo ratings yet
- Drug FormularyDocument16 pagesDrug FormularySunil BasnetNo ratings yet
- Musculoskeletal PharmacologyDocument18 pagesMusculoskeletal PharmacologyBLEEMAGE100% (2)
- Nursing Drug CardsDocument32 pagesNursing Drug CardsJenna Rasmussen100% (3)
- Drug StudyDocument8 pagesDrug StudyMike Faustino SolangonNo ratings yet
- AKI Slide Share Harrison UsedDocument47 pagesAKI Slide Share Harrison UsedHesbon MomanyiNo ratings yet
- Med Cards Starting With A PDFDocument7 pagesMed Cards Starting With A PDFDonn Patrick AlegreNo ratings yet
- DRUG STUDY - AcetamenophinDocument3 pagesDRUG STUDY - AcetamenophinChenime AñanaNo ratings yet
- Drug StudyDocument5 pagesDrug StudyJann Zaniel Allayne RiNo ratings yet
- Camuso OtcDocument15 pagesCamuso Otcapi-548307464No ratings yet
- Nephrotoxic DrugsDocument43 pagesNephrotoxic DrugsAnnisa Mulyandini100% (1)
- Paracetamol Overdose and Management IIIDocument10 pagesParacetamol Overdose and Management IIIعلي حسين عودة العلياويNo ratings yet
- Drug StudyDocument10 pagesDrug StudyRye IbarraNo ratings yet
- Drug Induced DiseasesDocument8 pagesDrug Induced DiseasesB.pharm 16th BatchNo ratings yet
- AntiepilepticsDocument25 pagesAntiepilepticsMurali Krishna Kumar MuthyalaNo ratings yet
- Fluimucil TabletDocument21 pagesFluimucil TabletJammilaKateDakayNo ratings yet
- Obat-Obat NefrotoksikDocument43 pagesObat-Obat Nefrotoksiknursidiq10100% (1)
- Anesthesia DrugsDocument3 pagesAnesthesia DrugsLeon BeaulieuNo ratings yet
- Effects On Lab Test ResultsDocument18 pagesEffects On Lab Test Resultsjay5ar5jamorabon5torNo ratings yet
- 2.5. Drugs Interaction (Dr. Kinanti)Document135 pages2.5. Drugs Interaction (Dr. Kinanti)dikri pangersaNo ratings yet
- Medications NHBDocument40 pagesMedications NHBAnonymous 7hJgATNo ratings yet
- NCM 106 Nsaid'sDocument6 pagesNCM 106 Nsaid'sLi mNo ratings yet
- 5 - Drugs Used For Treatment of Gout EditedDocument35 pages5 - Drugs Used For Treatment of Gout EditedSakariye hasanNo ratings yet
- Drugs Affecting The Adrenergic Nervous SystemDocument37 pagesDrugs Affecting The Adrenergic Nervous SystemJah SuNo ratings yet
- Respiratory Tract PharmacologyDocument68 pagesRespiratory Tract PharmacologyRohaan SharmaNo ratings yet
- Pharma Drug Tables - 1st ShiftingDocument29 pagesPharma Drug Tables - 1st ShiftingHei LeeNo ratings yet
- EsomeprazoleDocument2 pagesEsomeprazoleitsmeaya50% (2)
- DrugsDocument155 pagesDrugsAkankshaNo ratings yet
- Pharmacology: Teratogenic CarcinogenicDocument13 pagesPharmacology: Teratogenic CarcinogenicSherlock HolmesNo ratings yet
- Drugs Med-SurgTest 3Document6 pagesDrugs Med-SurgTest 3Sarah PlunkettNo ratings yet
- Coxib 2Document4 pagesCoxib 2ras emil sazuraNo ratings yet
- Lec9 د ذو الفقارDocument4 pagesLec9 د ذو الفقارMohammed JaberNo ratings yet
- 9 AntiinflammatoryDocument21 pages9 AntiinflammatoryAmr SalemNo ratings yet
- NsaidsDocument3 pagesNsaidsKate CortinaNo ratings yet
- Drug Ana Surgery WardDocument11 pagesDrug Ana Surgery WardJames QuilingNo ratings yet
- Doms DrugsDocument5 pagesDoms DrugsMikz JocomNo ratings yet
- Drug StudyDocument14 pagesDrug StudyHannah Philene D. CalubNo ratings yet
- Pain Medications: Dr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik UnjaDocument49 pagesPain Medications: Dr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik UnjaHawa Ambarwati100% (1)
- Pharmacology of NSAIDS: Mustafa .DsDocument49 pagesPharmacology of NSAIDS: Mustafa .DsMarhaban WienNo ratings yet
- ZolfinDocument3 pagesZolfinKhaled HasanNo ratings yet
- Drug ChartDocument20 pagesDrug Chartstarobin100% (1)
- Ma. Patricia R. de Leon Bsn-Iv: Drug Indications Contraindicatio Ns Action Adverse Effect Nursing ResponsibilitiesDocument6 pagesMa. Patricia R. de Leon Bsn-Iv: Drug Indications Contraindicatio Ns Action Adverse Effect Nursing ResponsibilitiesTricia_De_Leon_6494No ratings yet
- Of Angina Pectoris. Decreased Rate of Cardiovascular Mortality and Hospitalization in Patients With Heart FailureDocument31 pagesOf Angina Pectoris. Decreased Rate of Cardiovascular Mortality and Hospitalization in Patients With Heart Failurenaikram420No ratings yet
- Introduction CarbamazepineDocument4 pagesIntroduction Carbamazepineammaramaryam6463No ratings yet
- SympathomimeticDocument56 pagesSympathomimeticvarish0% (1)
- DrugsDocument5 pagesDrugsVal Ian Palmes SumampongNo ratings yet
- WEEK2 Course Task (ALFEREZ, DINIELA)Document4 pagesWEEK2 Course Task (ALFEREZ, DINIELA)DINIELA ALLAINE ALFEREZNo ratings yet
- MedSurg Medication Study Guide Test 1Document12 pagesMedSurg Medication Study Guide Test 1Sarah PlunkettNo ratings yet
- Acetaminophen: ClassificationDocument3 pagesAcetaminophen: ClassificationYosef OxinioNo ratings yet
- Nsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyDocument65 pagesNsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyYousef JafarNo ratings yet
- Interaksi Obat FarmakodinamikDocument33 pagesInteraksi Obat FarmakodinamikGurobha Al JawhiyNo ratings yet
- Chapter 4 Drug ProfileDocument5 pagesChapter 4 Drug ProfileSandeepNo ratings yet
- Antiepileptic DrugsDocument43 pagesAntiepileptic DrugsdrpraneethpremkumarNo ratings yet
- Non-Steroidal Anti-Inflammatory Drugs (Nsaids) : Analgesic, Anti-Pyretic and Anti-Inflammatory AgentsDocument45 pagesNon-Steroidal Anti-Inflammatory Drugs (Nsaids) : Analgesic, Anti-Pyretic and Anti-Inflammatory AgentsArvi KhanNo ratings yet
- Fast Facts: Acute and Recurrent Pancreatitis: Using evidence to support treatmentFrom EverandFast Facts: Acute and Recurrent Pancreatitis: Using evidence to support treatmentNo ratings yet
- Assisting With A Sitz BathDocument3 pagesAssisting With A Sitz BathAlano S. LimgasNo ratings yet
- C SectionDocument50 pagesC SectionAlano S. LimgasNo ratings yet
- PathosDocument2 pagesPathosAlano S. LimgasNo ratings yet
- Primitive Reflexes Cheat Sheet FinalDocument3 pagesPrimitive Reflexes Cheat Sheet FinalAlano S. LimgasNo ratings yet
- New DiscoveriesDocument1 pageNew DiscoveriesAlano S. LimgasNo ratings yet
- He LimDocument9 pagesHe LimAlano S. LimgasNo ratings yet
- Nonsteroidal Antiinflammatory DrugsDocument12 pagesNonsteroidal Antiinflammatory DrugsAlano S. LimgasNo ratings yet
- Anti HistaminesDocument16 pagesAnti HistaminesAlano S. LimgasNo ratings yet
- GlucocorticoidsDocument15 pagesGlucocorticoidsAlano S. LimgasNo ratings yet
- ImmunosuppressantsDocument29 pagesImmunosuppressantsAlano S. LimgasNo ratings yet
- UpcatDocument9 pagesUpcatAlano S. LimgasNo ratings yet
- GGGGGGGGGGGGGGGGGGDocument1 pageGGGGGGGGGGGGGGGGGGAlano S. LimgasNo ratings yet
- Controlled Substances LawsDocument8 pagesControlled Substances LawsJames Lindon100% (1)
- Dokumen - Tips - List of Pharma Companies in GujaratDocument22 pagesDokumen - Tips - List of Pharma Companies in Gujaratbhavyapanchalv4No ratings yet
- 68922Document40 pages68922arnidaNo ratings yet
- Combinatorial Synthesis PDFDocument2 pagesCombinatorial Synthesis PDFMattNo ratings yet
- Lecture PharmacokineticsDocument55 pagesLecture Pharmacokineticssatya narayan100% (2)
- Flurbiprofen A Potent Pain Reliever jbb.1000214 PDFDocument3 pagesFlurbiprofen A Potent Pain Reliever jbb.1000214 PDFAbdus SamadNo ratings yet
- Module I The Pharmaceutical BusinessDocument64 pagesModule I The Pharmaceutical BusinessdanglingsNo ratings yet
- EndotoxinLimits SeanJH PR17 012Document7 pagesEndotoxinLimits SeanJH PR17 012sppNo ratings yet
- Hospital FormularyDocument18 pagesHospital FormularyNikki Chauhan75% (4)
- 2019 Guidelines ATC WebDocument283 pages2019 Guidelines ATC WebAnonymous W4wIVhA550% (1)
- Nepalese Pharmaceutical Industries & Who GMPDocument6 pagesNepalese Pharmaceutical Industries & Who GMPJaya Bir Karmacharya100% (1)
- European Union Herbal Monograph On Malva Sylvestris L. And/or Malva Neglecta Wallr., FoliumDocument7 pagesEuropean Union Herbal Monograph On Malva Sylvestris L. And/or Malva Neglecta Wallr., Foliumkimphung91090No ratings yet
- Medication ErrorsDocument3 pagesMedication ErrorsjamiemapanaoNo ratings yet
- Compounding and Dispensing 519 Lab Manual FinalDocument39 pagesCompounding and Dispensing 519 Lab Manual FinalAnonymous gSOBy38Y7100% (3)
- Puskesmas: Modo Kecamatan: Bukal Kab/Kota: Buol Propinsi: Sulawesi Tengah Bulan: JanuariDocument42 pagesPuskesmas: Modo Kecamatan: Bukal Kab/Kota: Buol Propinsi: Sulawesi Tengah Bulan: JanuariFransiskaNo ratings yet
- 743 VIRCHOW HEALTHCARE PVT. LTD. Company Brochure 20220810114919Document2 pages743 VIRCHOW HEALTHCARE PVT. LTD. Company Brochure 20220810114919amitNo ratings yet
- Lista para Observatorios de PreciosDocument6 pagesLista para Observatorios de PreciosJaime Palacios GonzalesNo ratings yet
- Medicines Checklist AuditDocument5 pagesMedicines Checklist AuditEvelyn CamposNo ratings yet
- Ch4 Cost-Minimization Analysis PDFDocument12 pagesCh4 Cost-Minimization Analysis PDFAhmad Makhlouf100% (1)
- Aplikasi Apotek Fadilah FarmaDocument75 pagesAplikasi Apotek Fadilah FarmaRama RakanataNo ratings yet
- Medication Dosage and CalculationsDocument32 pagesMedication Dosage and CalculationsGavinTLDNo ratings yet
- Ijipsrmnr 880Document13 pagesIjipsrmnr 880srirampharmNo ratings yet
- Pharmacokinetic of LevodopaDocument10 pagesPharmacokinetic of LevodopaMukesh GamiNo ratings yet
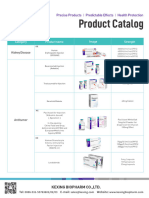
- 02-Kexing Product Catalogue (Index)Document2 pages02-Kexing Product Catalogue (Index)londonpharmauzNo ratings yet
- Dokumen - Tips General Pharmacology by DR BashirDocument21 pagesDokumen - Tips General Pharmacology by DR BashirMuhammad WaleedNo ratings yet
- 3015 - Prin. K.M. Kundnani College of Pharmacy, MumbaiDocument5 pages3015 - Prin. K.M. Kundnani College of Pharmacy, MumbaiChetana JadhavNo ratings yet
- Public Assessment Report Scientific DiscussionDocument19 pagesPublic Assessment Report Scientific DiscussionTaki JuveNo ratings yet
- Curriculum Vitae ToxicologyDocument6 pagesCurriculum Vitae Toxicologyvenkata gangadharNo ratings yet
- Preparation No. "04" "Castor Oil Capsule" A. Wrap-Up Guide QuestionsDocument4 pagesPreparation No. "04" "Castor Oil Capsule" A. Wrap-Up Guide QuestionsJames AzurinNo ratings yet
- What Is Route of Administration?Document4 pagesWhat Is Route of Administration?Quách Việt HoàngNo ratings yet