You might also like
- Caries ProfundaDocument8 pagesCaries ProfundacyntiamalikfaNo ratings yet
- A Simple Guide to Bad Breath and Mouth DiseasesFrom EverandA Simple Guide to Bad Breath and Mouth DiseasesRating: 5 out of 5 stars5/5 (3)
- Dental Caries Bahasa InggrisDocument4 pagesDental Caries Bahasa InggrisNOVIANA D4 2017No ratings yet
- Dental Caries Causes, Types & PreventionDocument4 pagesDental Caries Causes, Types & PreventionChana 'eLecter' ChuLumNo ratings yet
- Tipus Modul 7Document48 pagesTipus Modul 7cyntiamalikfaNo ratings yet
- Dental Plaque PresentationDocument10 pagesDental Plaque PresentationHeshamNo ratings yet
- Dental Caries Etiology and MicrobiologyDocument18 pagesDental Caries Etiology and MicrobiologytapovijaymNo ratings yet
- Dental Caries: Defination Etiology MicrobiologyDocument18 pagesDental Caries: Defination Etiology MicrobiologyRbk FairladyNo ratings yet
- Dental Plaque PresentationDocument10 pagesDental Plaque PresentationHesham100% (1)
- Referat EnglezaDocument6 pagesReferat EnglezaCorinaNo ratings yet
- Dental Caries DevelopmentDocument8 pagesDental Caries Developmentريام الموسويNo ratings yet
- Preven Lec 2Document7 pagesPreven Lec 2ريام الموسويNo ratings yet
- Dental CariesDocument25 pagesDental CariesFemi100% (1)
- Caries 16888Document9 pagesCaries 16888Ion PopovNo ratings yet
- Lec 11 Dental CariesDocument8 pagesLec 11 Dental Cariesاحمد حسن جاسم كاظمNo ratings yet
- Dental CariesDocument3 pagesDental CariesrezabahidaNo ratings yet
- Dental PlaqueDocument10 pagesDental PlaqueAnonymous 4FVm26mbcONo ratings yet
- Cause of Dental Caries: BacteriaDocument1 pageCause of Dental Caries: Bacteriatirsaaa1No ratings yet
- Group ADocument34 pagesGroup AMahmodol HasanNo ratings yet
- Prevention of Dental CariesDocument6 pagesPrevention of Dental CariesRadhwan Hameed AsadNo ratings yet
- Dental Caries: Signs and SymptomsDocument13 pagesDental Caries: Signs and SymptomsGeorgiana IlincaNo ratings yet
- Unknown (3) 31 89Document59 pagesUnknown (3) 31 89Daniah MNo ratings yet
- Dental Plaque 2017Document11 pagesDental Plaque 2017MrWolf23No ratings yet
- Dental caries prevention and managementDocument9 pagesDental caries prevention and managementGaby Araya AlvarezNo ratings yet
- Dental CariesDocument19 pagesDental CariesTesisTraduccionesRuzel100% (5)
- Research PaperDocument8 pagesResearch Paperapi-508053077No ratings yet
- 40653_2019_Article_247Document5 pages40653_2019_Article_247faridoon7766No ratings yet
- What Is Dental PlaqueDocument9 pagesWhat Is Dental PlaqueHesham100% (1)
- Dental Caries MSCDocument137 pagesDental Caries MSCNahla OthmanNo ratings yet
- Etiology of Periodontal Diseases: Dental Plaque (Microorganisms)Document9 pagesEtiology of Periodontal Diseases: Dental Plaque (Microorganisms)محمد محمود القحيفNo ratings yet
- Dental Plaque: Dental Diseases and Risk of Coronary Heart Disease and MortalityDocument54 pagesDental Plaque: Dental Diseases and Risk of Coronary Heart Disease and MortalityNabilah ZulkiflyNo ratings yet
- Pathology of Teeth and Supporting StructuresDocument45 pagesPathology of Teeth and Supporting StructuresIsak ShatikaNo ratings yet
- Carious Cavities Classification by Black. Features of Carious Cavities Preparation of The 1-st and 5-th Black's ClassesDocument24 pagesCarious Cavities Classification by Black. Features of Carious Cavities Preparation of The 1-st and 5-th Black's ClassesmanarchikNo ratings yet
- Research Paper - Bacterial Plaque and Relationship To Dental DiseaseDocument8 pagesResearch Paper - Bacterial Plaque and Relationship To Dental Diseaseapi-313829416No ratings yet
- Bad Oral HygieneDocument45 pagesBad Oral HygieneMohsin HabibNo ratings yet
- Lec2/ Epidemiology of Dental CariesDocument7 pagesLec2/ Epidemiology of Dental Cariesمحمد العراقيNo ratings yet
- Lec2/ Epidemiology of Dental CariesDocument7 pagesLec2/ Epidemiology of Dental Cariesمحمد العراقيNo ratings yet
- 61.shamita SivarajooDocument19 pages61.shamita Sivarajoobdsaimstb17No ratings yet
- Prevention of Dental Caries: Name:Huda Khan ROLL #: 753Document33 pagesPrevention of Dental Caries: Name:Huda Khan ROLL #: 753Hudh HudNo ratings yet
- Eb 79Document5 pagesEb 79mohammad naufalNo ratings yet
- Dental PlaqueDocument6 pagesDental PlaqueZartasha Amaid ButtNo ratings yet
- Mutans and Lactobacilli. Cavity or Decay of A Tooth Is A Localized DiseaseDocument12 pagesMutans and Lactobacilli. Cavity or Decay of A Tooth Is A Localized Diseasegie_gie123No ratings yet
- The Effect Apis Mellifera Honey On The Growth of Bacteria Cause Periodontal DiseaseDocument6 pagesThe Effect Apis Mellifera Honey On The Growth of Bacteria Cause Periodontal DiseaseNadiyah Rizqi ANo ratings yet
- InTech-Molar Incisor Hypomineralization Morphological Aetiological Epidemiological and Clinical ConsiderationsDocument25 pagesInTech-Molar Incisor Hypomineralization Morphological Aetiological Epidemiological and Clinical ConsiderationsNeagu EmaNo ratings yet
- Research PaperDocument7 pagesResearch Paperapi-454004347No ratings yet
- Dental Health Knowledge and Incidence of Dental CariesDocument10 pagesDental Health Knowledge and Incidence of Dental Cariesdhea wirantiNo ratings yet
- Development of Dental Caries and TheoriesDocument6 pagesDevelopment of Dental Caries and TheoriesHaider F YehyaNo ratings yet
- Etiology of Dental CariesDocument35 pagesEtiology of Dental Cariesayshil mary sajiNo ratings yet
- Task - 5Document5 pagesTask - 5ZC47No ratings yet
- Dental Caries: by DR: Hanan Eid GamalDocument107 pagesDental Caries: by DR: Hanan Eid Gamalruchika100% (1)
- Microbiology Evaluation of Bristles of Frequently Used ToothbrushesDocument6 pagesMicrobiology Evaluation of Bristles of Frequently Used ToothbrushesAderayo DosunmuNo ratings yet
- Dental DiseaseDocument15 pagesDental Diseasetien280917No ratings yet
- Dental Plaque and Dental Caries: Lect. 23Document5 pagesDental Plaque and Dental Caries: Lect. 23Brandon AviciiNo ratings yet
- Preventive DentsDocument12 pagesPreventive DentsMyra N SupriadiNo ratings yet
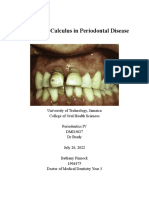
- Role of Calculus in Periodontal DiseaseDocument4 pagesRole of Calculus in Periodontal DiseaseBethany PinnockNo ratings yet
- Introduction To Restorative Dental Materials: ObjectivesDocument13 pagesIntroduction To Restorative Dental Materials: ObjectivessamiyaNo ratings yet
- Dental Plaque and CalculusDocument20 pagesDental Plaque and CalculusjonadoctorNo ratings yet
- Git DisordersnewDocument401 pagesGit DisordersnewstaceyatienoomaNo ratings yet
- Dental Caries Definition and StagesDocument11 pagesDental Caries Definition and StagescartoonNo ratings yet
- Aim Global TieupsDocument84 pagesAim Global Tieupsjhorgecruz18No ratings yet
- Full Veneer Versus Traditional Veneer Preparation - A Discussion of Interproximal ExtensionDocument5 pagesFull Veneer Versus Traditional Veneer Preparation - A Discussion of Interproximal ExtensionDr. Zardasht N. BradostyNo ratings yet
- Developmental Anomalies-DentalDocument16 pagesDevelopmental Anomalies-DentalMvNo ratings yet
- NASPUB Anha FixDocument5 pagesNASPUB Anha FixAditya AlamsyahNo ratings yet
- KCE - 332C - Antibiotics - in - Dental - Office - Short Report - 1Document30 pagesKCE - 332C - Antibiotics - in - Dental - Office - Short Report - 1Evelyn SosaNo ratings yet
- Class 2 Division 2 by AlmuzianDocument16 pagesClass 2 Division 2 by AlmuzianAya ElsayedNo ratings yet
- 2 Interim and Temporary Restoration of Teeth During Endodontic Treatment PDFDocument17 pages2 Interim and Temporary Restoration of Teeth During Endodontic Treatment PDFjhon HanselNo ratings yet
- Fixed Ortho Retainers Long TermDocument2 pagesFixed Ortho Retainers Long TermMaria Fernanda Garcia PucheNo ratings yet
- DENTAL EXAM SAMPLE QUESTIONSDocument8 pagesDENTAL EXAM SAMPLE QUESTIONSHabeeb AL-AbsiNo ratings yet
- Unit 11 A 12Document4 pagesUnit 11 A 12Susana ʕ•́ᴥ•̀ʔっNo ratings yet
- Ca. Ca.: - .,.1b1h1tlesDocument179 pagesCa. Ca.: - .,.1b1h1tleshNo ratings yet
- Ultimate Performance and Handling: Pre-Hydrated Collagenated Heterologous Cortico-Cancellous Bone MixDocument6 pagesUltimate Performance and Handling: Pre-Hydrated Collagenated Heterologous Cortico-Cancellous Bone MixFlorin CiudinNo ratings yet
- Extraction of Maxillary Teeth Using Articaine Without A Palatal InjectionDocument5 pagesExtraction of Maxillary Teeth Using Articaine Without A Palatal InjectionAhmadH.MahdiNo ratings yet
- A 3-Year Clinical Evaluation of Endodontically Treated Posterior Teeth Restored With Two Different Materials Using The CEREC AC Chair-Side SystemDocument6 pagesA 3-Year Clinical Evaluation of Endodontically Treated Posterior Teeth Restored With Two Different Materials Using The CEREC AC Chair-Side SystemMaria Fernanda ScarpettaNo ratings yet
- Pin Retained Restorations: DR Rakesh Kumar YadavDocument59 pagesPin Retained Restorations: DR Rakesh Kumar YadavShubham NaikNo ratings yet
- Prostho Set 1 ADocument15 pagesProstho Set 1 ABinayak UpadhyayaNo ratings yet
- Describing InstrumentDocument9 pagesDescribing InstrumentREFTA DEVINo ratings yet
- Periodoncia y ProstodonciaDocument5 pagesPeriodoncia y ProstodonciaTpz DiegoNo ratings yet
- Development of Salt Uoridation in The Americas: G M. G and R BDocument7 pagesDevelopment of Salt Uoridation in The Americas: G M. G and R BMahmoud SulimanNo ratings yet
- MCQs For PGs in Prosthodontics PDFDocument176 pagesMCQs For PGs in Prosthodontics PDFHanin AbukhiaraNo ratings yet
- Brasseler USA Dental Catalog 11Document468 pagesBrasseler USA Dental Catalog 11Payal JainNo ratings yet
- 350 Wordlist Form (1) 4Document90 pages350 Wordlist Form (1) 4VANNA ChanmolisaNo ratings yet
- Smile Characteristics in Orthodontics: A Concept ReviewDocument4 pagesSmile Characteristics in Orthodontics: A Concept Reviewjaganath venkatNo ratings yet
- AsplDocument9 pagesAsplCristinaNo ratings yet
- Growth and Development of Jaws - Complemenatry and Compensenatory GrowthDocument63 pagesGrowth and Development of Jaws - Complemenatry and Compensenatory GrowthvasabakaNo ratings yet
- Assessment of Validity of Pont’s Index in Nepalese PopulationDocument5 pagesAssessment of Validity of Pont’s Index in Nepalese PopulationAlaghen VespanathanNo ratings yet
- Single Visit Vs Multiple Visits - OldDocument19 pagesSingle Visit Vs Multiple Visits - OldJzNo ratings yet
- Comparison of Accuracy Between A Conventional and Two Digital Intraoral Impression TechniquesDocument7 pagesComparison of Accuracy Between A Conventional and Two Digital Intraoral Impression TechniquesDiego LopezNo ratings yet
- Vertical Maxillary ExcessDocument125 pagesVertical Maxillary ExcessYuvashreeNo ratings yet
- History of DentistryDocument58 pagesHistory of Dentistryrrq8cwk2gnNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)