You might also like
- Medical Certificate of Fitness: Section 1: Candidate's Personal DetailsDocument2 pagesMedical Certificate of Fitness: Section 1: Candidate's Personal DetailsSwastik Trading AgenciesNo ratings yet
- COVID1981 Ebook PDFDocument105 pagesCOVID1981 Ebook PDFMexico English100% (2)
- COVID1981 Ebook PDFDocument105 pagesCOVID1981 Ebook PDFMexico English100% (2)
- Acknowledging Support and Guidance for an Ayurvedic ThesisDocument270 pagesAcknowledging Support and Guidance for an Ayurvedic ThesislekhishvardhanNo ratings yet
- Client Intake FormDocument2 pagesClient Intake FormPeter Sosa100% (1)
- EMS003 Fundamentals of Hot Stone MassageDocument102 pagesEMS003 Fundamentals of Hot Stone Massagemanole voichita ana100% (1)
- Usa PDFDocument156 pagesUsa PDFMexico EnglishNo ratings yet
- Mus Culo SkeletalDocument16 pagesMus Culo Skeletalshenric16100% (2)
- Client Info FormDocument2 pagesClient Info FormkamalsalmanNo ratings yet
- Orthopedics Focus - Emerging Companies To Watch - OneMedPlaceDocument60 pagesOrthopedics Focus - Emerging Companies To Watch - OneMedPlaceDoug100% (7)
- MediSpa Intake FormsDocument9 pagesMediSpa Intake FormsUtopiaawaitsNo ratings yet
- Max Life Insurance Company LimitedDocument1 pageMax Life Insurance Company LimitedRavindranathNo ratings yet
- Kidney and Urinary Disorder QuestionnaireDocument2 pagesKidney and Urinary Disorder Questionnairejeevan820No ratings yet
- Max Life Insurance Company Limited Respiratory QuestionnaireDocument2 pagesMax Life Insurance Company Limited Respiratory QuestionnaireJanakiRamanNo ratings yet
- Advance Referral Form 1Document1 pageAdvance Referral Form 1Khairul ScNo ratings yet
- Health History Assessment ToolDocument3 pagesHealth History Assessment ToolDaniela Suarez NimNo ratings yet
- EMG Patient Registration & Health HistoryDocument8 pagesEMG Patient Registration & Health HistoryBakenaz MostafaNo ratings yet
- Consent FormsDocument2 pagesConsent FormsKristeline MedelNo ratings yet
- Cardiovascular Module2Document27 pagesCardiovascular Module2Gracia MayaNo ratings yet
- Headaches Residual Functional Capacity QuestionnaireDocument3 pagesHeadaches Residual Functional Capacity QuestionnaireDellComputer99No ratings yet
- DOAC QuestionnaireDocument2 pagesDOAC QuestionnaireMuniba NasimNo ratings yet
- DENR Health Survey Form and Contact Person Form Page 2Document2 pagesDENR Health Survey Form and Contact Person Form Page 2Mary Jane BarrientosNo ratings yet
- Chnursing NotesDocument21 pagesChnursing Notesjimmy boy canlas jrNo ratings yet
- MiniCEX-Clinical-Reasoning 2Document3 pagesMiniCEX-Clinical-Reasoning 2Guillana Mae CastellonNo ratings yet
- 2019-ShadowerObserver-Application 191003 195038Document9 pages2019-ShadowerObserver-Application 191003 195038omer khanNo ratings yet
- RFC 2 PAGE Physical 2010 With OnsetDocument2 pagesRFC 2 PAGE Physical 2010 With OnsetghobbieNo ratings yet
- Halitosis QuestionnaireDocument3 pagesHalitosis Questionnairealumera50% (2)
- PE and Health ModuleDocument17 pagesPE and Health ModuleTessaKaye AlfaroNo ratings yet
- Bpi Philam Aph Attending Physician Hypertension QuestionnaireDocument2 pagesBpi Philam Aph Attending Physician Hypertension Questionnairekimberlycompetente24No ratings yet
- Proposal Number / Nombor Cadangan: Soal Selidik Sakit BelakangDocument3 pagesProposal Number / Nombor Cadangan: Soal Selidik Sakit BelakangWan SaifulNo ratings yet
- UOI Medical FormDocument2 pagesUOI Medical FormHaason TzNo ratings yet
- TUE - WADA Version 2016-EnDocument4 pagesTUE - WADA Version 2016-EnYannick MOSSUSNo ratings yet
- Request Refund Transfer FormDocument2 pagesRequest Refund Transfer FormKendra FouetsopNo ratings yet
- Occupation Health AssessmentDocument2 pagesOccupation Health AssessmentemeraldmecaelNo ratings yet
- Example - Intake-Questionaire-2023Document7 pagesExample - Intake-Questionaire-2023Matthew ZaldinNo ratings yet
- CDC Data Collection Long FormDocument13 pagesCDC Data Collection Long FormBanzai Health Private LimitedNo ratings yet
- MksU/4 Student Medical Examination FormDocument4 pagesMksU/4 Student Medical Examination FormRichard OsumoNo ratings yet
- Medical Form.Document4 pagesMedical Form.victoremai76No ratings yet
- Date: - : (Last) (First) (Middle)Document5 pagesDate: - : (Last) (First) (Middle)KatieNo ratings yet
- Mental Health QuestionnaireDocument1 pageMental Health QuestionnaireNelly HNo ratings yet
- Enrolment FormDocument2 pagesEnrolment FormHiy GisingNo ratings yet
- Member Application ReinstatementDocument2 pagesMember Application ReinstatementAbhinav VermaNo ratings yet
- Student+Physician+Form (1)Document1 pageStudent+Physician+Form (1)Masr RedaNo ratings yet
- Medical Evaluation Form For PAPsDocument4 pagesMedical Evaluation Form For PAPsPrint Media Printing pressNo ratings yet
- Medical Attendants Certificate17062019Document2 pagesMedical Attendants Certificate17062019PrathameshNo ratings yet
- Respiratory QuestionnaireDocument2 pagesRespiratory QuestionnaireMadhu SudhanNo ratings yet
- Aor Reporting FormDocument2 pagesAor Reporting FormPaidiHasanNo ratings yet
- Allergy Test Part ADocument23 pagesAllergy Test Part AAnkushNo ratings yet
- PCS - Physician's Clinical Statement Form 2019 EtiqaDocument2 pagesPCS - Physician's Clinical Statement Form 2019 EtiqaRowena CallosNo ratings yet
- Gym Member Registration FormDocument2 pagesGym Member Registration FormChethan Sharma RNo ratings yet
- Referral SourceDocument10 pagesReferral SourceHumberto FuentesNo ratings yet
- General Medical Aesthetics Release Form / Hold HarmlessDocument4 pagesGeneral Medical Aesthetics Release Form / Hold HarmlessjenderNo ratings yet
- English Health Clearance FormDocument2 pagesEnglish Health Clearance FormGerard HungNo ratings yet
- Phone: ( - ) - Fax: ( - ) - : (Company Name) Outpatient Physical Therapy EvaluationDocument2 pagesPhone: ( - ) - Fax: ( - ) - : (Company Name) Outpatient Physical Therapy Evaluationpt.mahmoudNo ratings yet
- Daily Diet and Medication Form 72 Hrs-Residential Diabetes Tour (27th-29th April-2018)Document2 pagesDaily Diet and Medication Form 72 Hrs-Residential Diabetes Tour (27th-29th April-2018)ZindagiDeeNo ratings yet
- James Earl Surmieda Donato - HEALTH APPRAISAL RECORDDocument3 pagesJames Earl Surmieda Donato - HEALTH APPRAISAL RECORDJames Earl DonatoNo ratings yet
- Esthetics FormDocument1 pageEsthetics FormTori BaileyNo ratings yet
- Consent Sample For Sexual AbuseDocument8 pagesConsent Sample For Sexual Abuseamarch517No ratings yet
- Health Questionnaire: Oral &maxillofacial SurgeryDocument6 pagesHealth Questionnaire: Oral &maxillofacial SurgeryPaul MathaiNo ratings yet
- APS FormDocument1 pageAPS Formviraj duaNo ratings yet
- Fitness Aziz AlhaidariDocument2 pagesFitness Aziz Alhaidariabdulaziz saif ali mansoorNo ratings yet
- Genitourinary Care Plan: InvestigationsDocument2 pagesGenitourinary Care Plan: InvestigationsOlaya alghareniNo ratings yet
- FORMS Informed Consent (For Procedures)Document1 pageFORMS Informed Consent (For Procedures)Jessa MaeNo ratings yet
- Hirtii Angajare OshawaDocument1 pageHirtii Angajare Oshawahutira1decembrieNo ratings yet
- Reason for TravelDocument1 pageReason for TravelDoyTanNo ratings yet
- Consent For Medications 2011Document1 pageConsent For Medications 2011maconjanice222No ratings yet
- Epilepsy Questionnaire SEODocument2 pagesEpilepsy Questionnaire SEOMexico EnglishNo ratings yet
- Digestive Questionnaire (Medical)Document1 pageDigestive Questionnaire (Medical)Mexico EnglishNo ratings yet
- Laws of Chemical CombinationDocument9 pagesLaws of Chemical CombinationMexico EnglishNo ratings yet
- LIC New Endowment Plus 9 Inch X 8 Inch EngDocument20 pagesLIC New Endowment Plus 9 Inch X 8 Inch EngMexico EnglishNo ratings yet
- Chest Pain Questionnaire (Medical)Document3 pagesChest Pain Questionnaire (Medical)Mexico EnglishNo ratings yet
- Merchant - Marine - Questionnaire (Non Medical)Document1 pageMerchant - Marine - Questionnaire (Non Medical)Mexico EnglishNo ratings yet
- Mountain climbing questionnaire guideDocument1 pageMountain climbing questionnaire guideMexico EnglishNo ratings yet
- Hypertention Questionnaire (Medical)Document1 pageHypertention Questionnaire (Medical)Mexico EnglishNo ratings yet
- Aviation - Questionnaire (Non Medical)Document2 pagesAviation - Questionnaire (Non Medical)Mexico EnglishNo ratings yet
- Employer-Employee - Annexure - D - Version - 1.0-4 (Non Medical)Document1 pageEmployer-Employee - Annexure - D - Version - 1.0-4 (Non Medical)Mexico EnglishNo ratings yet
- NRI - Questionaire (Non Medical)Document2 pagesNRI - Questionaire (Non Medical)Mexico EnglishNo ratings yet
- Tobacco Consumption Questionnaire (Medical)Document1 pageTobacco Consumption Questionnaire (Medical)Mexico EnglishNo ratings yet
- PAN (Encl. Photocopy) : Total DeductionsDocument1 pagePAN (Encl. Photocopy) : Total DeductionsMexico EnglishNo ratings yet
- RCare For You Health Declaration For Child Less Than 5 Yrs Ver1.2 (Medical)Document2 pagesRCare For You Health Declaration For Child Less Than 5 Yrs Ver1.2 (Medical)Mexico EnglishNo ratings yet
- InfoDocument1 pageInfoMexico EnglishNo ratings yet
- RtiDocument2 pagesRtiMexico EnglishNo ratings yet
- BRC Guidelines 2Document7 pagesBRC Guidelines 2Mexico EnglishNo ratings yet
- Cultural Organization Promotes Indian HeritageDocument18 pagesCultural Organization Promotes Indian HeritageBANDI N BHARADWAJ100% (2)
- Brahmacharya Gaurav by Swami Jagdishswaranand Saraswatipdf PDF FreeDocument83 pagesBrahmacharya Gaurav by Swami Jagdishswaranand Saraswatipdf PDF FreeMexico EnglishNo ratings yet
- Union Budget 2021Document58 pagesUnion Budget 2021Mexico EnglishNo ratings yet
- BTX LEVEL 1 (PRE-PROGRAM) - Workout Tracking Sheet: Week 1 Workout 1 Workout 2 Workout 3 Workout 4Document5 pagesBTX LEVEL 1 (PRE-PROGRAM) - Workout Tracking Sheet: Week 1 Workout 1 Workout 2 Workout 3 Workout 4Mexico EnglishNo ratings yet
- Referral to Orthopaedic Surgeon for Knee Cartilage SurgeryDocument18 pagesReferral to Orthopaedic Surgeon for Knee Cartilage SurgeryTINU THOMAS THOMASNo ratings yet
- Rehab ManualDocument11 pagesRehab ManualManoj KumarNo ratings yet
- Massage Therapy For Osteoarthritis of The KneeDocument6 pagesMassage Therapy For Osteoarthritis of The KneeDrAbhay ShankargoudaNo ratings yet
- Header Watermark (1) Daniel LemmingsDocument3 pagesHeader Watermark (1) Daniel LemmingsAparnnaNo ratings yet
- Musculoskeletal System - Ii: MBBS Year-3 (Academic Year 2020-2021)Document26 pagesMusculoskeletal System - Ii: MBBS Year-3 (Academic Year 2020-2021)Danyal AzamNo ratings yet
- Farmacoacupuntura JungDocument33 pagesFarmacoacupuntura JungCEMICG OFICIALNo ratings yet
- Top-Quality Physiotherapy DevicesDocument88 pagesTop-Quality Physiotherapy Devicesaudrey pahleviNo ratings yet
- Zimmer Praesentation ThermotkDocument36 pagesZimmer Praesentation ThermotkCrenguta BrasoveanuNo ratings yet
- Nursing PresentationDocument63 pagesNursing PresentationDeekayNo ratings yet
- Arthritis: Lecture By: M.K. SastryDocument17 pagesArthritis: Lecture By: M.K. SastryOmar Duran CastroNo ratings yet
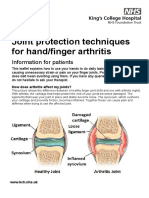
- Joint protection techniques for arthritisDocument5 pagesJoint protection techniques for arthritisXouya SuizenNo ratings yet
- Amavatha & VathasonithaDocument125 pagesAmavatha & VathasonithaCicil AbrahamNo ratings yet
- Thesis Topics For DNB Family MedicineDocument9 pagesThesis Topics For DNB Family Medicinegjhs6kja100% (2)
- 1 SMDocument14 pages1 SMEmmanuel BoulayNo ratings yet
- MeloxicamDocument10 pagesMeloxicamDian ArdiansyahNo ratings yet
- Imaging Approach To Inflammatory ArthritisDocument94 pagesImaging Approach To Inflammatory ArthritisYashan SharmaNo ratings yet
- 10.1016@j.csm.2009.09.004 2Document26 pages10.1016@j.csm.2009.09.004 29661jackNo ratings yet
- Pulun: Template Case Based Scenario Examination (Cbse) 20/21Document52 pagesPulun: Template Case Based Scenario Examination (Cbse) 20/21SleepyHead ˋωˊNo ratings yet
- Task 3 Case Notes: David TaylorDocument4 pagesTask 3 Case Notes: David TaylorMohammed ElSayedNo ratings yet
- ARCOXIADocument22 pagesARCOXIATeresa JunioNo ratings yet
- Medical-Surgical Questions With Rationale 70 QuestionsDocument59 pagesMedical-Surgical Questions With Rationale 70 QuestionsJam Torres100% (7)
- Mims Doctor May 2017 My2Document60 pagesMims Doctor May 2017 My2Budak ComotNo ratings yet
- Primary care polyarthralgiaDocument1 pagePrimary care polyarthralgiaLohJNo ratings yet
- Broccoli Based MedicineDocument3 pagesBroccoli Based MedicineMatthew StoneNo ratings yet
- Pat Fundies 2016Document18 pagesPat Fundies 2016api-371817203No ratings yet
- How Magnetic Therapy & Negative Ion Technology Can Aid Well-Being & Exercise RecoveryDocument9 pagesHow Magnetic Therapy & Negative Ion Technology Can Aid Well-Being & Exercise RecoveryDilpreet SinghNo ratings yet