You might also like
- Application/Registration For Disaster Assistance: Tornado Wind OtherDocument2 pagesApplication/Registration For Disaster Assistance: Tornado Wind OtherJIMOHNo ratings yet
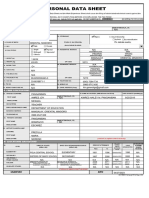
- CS Form 212 S2017Document4 pagesCS Form 212 S2017kinNo ratings yet
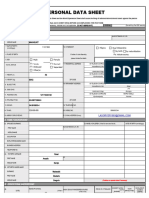
- Copy of Personal Data Sheet CS Form No. 212 Revised 2017 1Document8 pagesCopy of Personal Data Sheet CS Form No. 212 Revised 2017 1Nalyn BautistaNo ratings yet
- Proposal Form Standard Fire and Special Perils PolicyDocument6 pagesProposal Form Standard Fire and Special Perils PolicyAATMIK KRISHNA 2211731No ratings yet
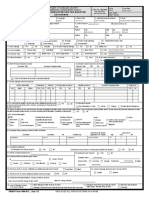
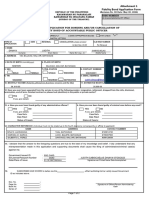
- Fidelity Bond Application Form Fillable v1.0 - (1) - (1) - (1)Document2 pagesFidelity Bond Application Form Fillable v1.0 - (1) - (1) - (1)Gary LLagunoNo ratings yet
- Customer Information Form IndividualDocument2 pagesCustomer Information Form IndividualCiel AnnNo ratings yet
- Personal Data SheetDocument8 pagesPersonal Data SheetAlberta Monica Defiesta YubalNo ratings yet
- Borang Tuntutan Kebakaran: Fire Claim FormDocument2 pagesBorang Tuntutan Kebakaran: Fire Claim FormNafy OmarNo ratings yet
- Cs Form TabanaoDocument4 pagesCs Form TabanaoHarris DarpingNo ratings yet
- PDS Blank FormDocument5 pagesPDS Blank Formax-120stNo ratings yet
- JEFFREY MACALINO Personal Data Sheet RevisedDocument4 pagesJEFFREY MACALINO Personal Data Sheet RevisedJeffrey MacalinoNo ratings yet
- Excel File CSC Personal Data Sheet PDS 2017Document8 pagesExcel File CSC Personal Data Sheet PDS 2017lasorrey1993No ratings yet
- Personal Data Sheet: Ragudo Joy Paul Autentico 1/5/1995Document4 pagesPersonal Data Sheet: Ragudo Joy Paul Autentico 1/5/1995ragz autenticNo ratings yet
- Fidelity Bond Application Form FBAFDocument2 pagesFidelity Bond Application Form FBAFREYES-DEVILLA LAW OFFICENo ratings yet
- Belle Pds 2020Document6 pagesBelle Pds 2020Angeline Baltar MarisgaNo ratings yet
- Aissa 1Document8 pagesAissa 1paulinoaissajNo ratings yet
- Personal Data Sheet: Kiangan, IfugaoDocument4 pagesPersonal Data Sheet: Kiangan, IfugaoCyprene Chady DumawatNo ratings yet
- Personal Data Sheet: Kiangan, IfugaoDocument4 pagesPersonal Data Sheet: Kiangan, IfugaoCyprene Chady DumawatNo ratings yet
- Personal Data SheetDocument8 pagesPersonal Data SheetNabel SalicNo ratings yet
- Pds New BlankDocument4 pagesPds New BlankJohn CanalitaNo ratings yet
- Personal Data Sheet FormDocument4 pagesPersonal Data Sheet FormCasim Bailan JrNo ratings yet
- New PDS MayetteDocument4 pagesNew PDS MayetteMayette Danias MondaloNo ratings yet
- Che PDSDocument16 pagesChe PDSLILIBETH G. SALATANNo ratings yet
- Personal Data SheetDocument12 pagesPersonal Data Sheetroldan lahingNo ratings yet
- Pds 2023 BlankDocument5 pagesPds 2023 BlankMea Joy Albao ColanaNo ratings yet
- CS Form No. 212 Revised Personal Data Sheet 2023-2024Document4 pagesCS Form No. 212 Revised Personal Data Sheet 2023-2024Juanito Jr. RafananNo ratings yet
- Personal Data SheetDocument4 pagesPersonal Data SheetCromwell dela CruzNo ratings yet
- CS Form No. 212 Revised 2017Document14 pagesCS Form No. 212 Revised 2017Janie Mary Bonz50% (2)
- Guideline On How To Fill Out The Customer Signature Card - ShopeeDocument2 pagesGuideline On How To Fill Out The Customer Signature Card - ShopeeCharisse Hope RadazaNo ratings yet
- CS Form No. 212 Pds JAN 2023Document4 pagesCS Form No. 212 Pds JAN 2023Aurelio Jr. BatuaNo ratings yet
- PDS MedinaDocument4 pagesPDS MedinaRashiel Jane CelizNo ratings yet
- Personal Data Sheet: Filipino Dual Citizenship by Birth by Naturalization Pls. Indicate CountryDocument4 pagesPersonal Data Sheet: Filipino Dual Citizenship by Birth by Naturalization Pls. Indicate CountrybaroukNo ratings yet
- C4 AmeliaDocument12 pagesC4 AmeliaDexter TantoyNo ratings yet
- Blanko PDS New Update Feb 2019Document4 pagesBlanko PDS New Update Feb 2019Rexter UnabiaNo ratings yet
- Customer Information Form Individual PDFDocument2 pagesCustomer Information Form Individual PDFDessa Mae SarmientoNo ratings yet
- Personal Data Sheet: Coronel Emilou Name Extension (JR., SR) SapungayDocument7 pagesPersonal Data Sheet: Coronel Emilou Name Extension (JR., SR) SapungayEm CoronelNo ratings yet
- Fidelity Bond Application Form FBAFDocument2 pagesFidelity Bond Application Form FBAF20192370No ratings yet
- Datomanong, NadjirahDocument4 pagesDatomanong, NadjirahMonikie MalaNo ratings yet
- Edris PDSDocument4 pagesEdris PDSEbrahim PanesNo ratings yet
- PDS Sample For SubstituteDocument8 pagesPDS Sample For SubstituteJennylyn JulianNo ratings yet
- Mellissa Anne Wright (Carone)Document4 pagesMellissa Anne Wright (Carone)Law&CrimeNo ratings yet
- CS Form No. 212 GuideDocument8 pagesCS Form No. 212 GuidePolicy & Research Unit - Center for Federalism & Constitutional ReformNo ratings yet
- 1175.15 (Land Contract) 20200825082228328Document15 pages1175.15 (Land Contract) 20200825082228328Emeka GratitudeNo ratings yet
- Pds Latest1Document4 pagesPds Latest1PsycheNecko VillacortaNo ratings yet
- List of Attorneys 2019Document3 pagesList of Attorneys 2019Richard RamkissoonNo ratings yet
- CS Form No. 212 Personal Data SheetDocument7 pagesCS Form No. 212 Personal Data SheetRenalyn CatalanNo ratings yet
- Grace PantaleonDocument4 pagesGrace PantaleonAnonymous WXqKjTXMNo ratings yet
- Personal Data Sheet: Filipino Dual Citizenship by Birth by NaturalizationDocument7 pagesPersonal Data Sheet: Filipino Dual Citizenship by Birth by NaturalizationAniaNo ratings yet
- CS Form No. 212 Revised Personal Data Sheet - 2017Document4 pagesCS Form No. 212 Revised Personal Data Sheet - 2017Agnes Francisco94% (17)
- CS Form 212 GuideDocument4 pagesCS Form 212 GuideAle XaNo ratings yet
- Personal Data SheetDocument14 pagesPersonal Data SheetRene GalanzaNo ratings yet
- CS Form No. 212 Personal Data Sheet CopyDocument4 pagesCS Form No. 212 Personal Data Sheet Copyairblaze27No ratings yet
- Santosmj - 97M0052Document7 pagesSantosmj - 97M0052jongsantos73No ratings yet
- CS Form 212 PDS 2017 Blank 1Document9 pagesCS Form 212 PDS 2017 Blank 1Yessamin Villadares PetchayNo ratings yet
- Personal Data SheetDocument6 pagesPersonal Data SheetNeresa MonesNo ratings yet
- 1pds Form Princess1Document4 pages1pds Form Princess1secret hahahaNo ratings yet
- 2017 Personal Data Sheet GRACEDocument13 pages2017 Personal Data Sheet GRACEGrace Cañones-TandasNo ratings yet
- Ate TessDocument15 pagesAte TessAYSON N. DELA CRUZNo ratings yet
- Maverick Real Estate Investing: The Art of Buying and Selling Properties Like Trump, Zell, Simon, and the World's Greatest Land OwnersFrom EverandMaverick Real Estate Investing: The Art of Buying and Selling Properties Like Trump, Zell, Simon, and the World's Greatest Land OwnersRating: 5 out of 5 stars5/5 (1)
- T0050DL SKLLSRSTSTSMNLDocument43 pagesT0050DL SKLLSRSTSTSMNLAshwini PrabhakaranNo ratings yet
- Bank of America: It's Bank Policy!: IBS Center For Management ResearchDocument3 pagesBank of America: It's Bank Policy!: IBS Center For Management Researchgowtham .BNo ratings yet
- National Association of The Deaf v. Harvard University, Class Action ComplaintDocument31 pagesNational Association of The Deaf v. Harvard University, Class Action ComplaintFindLawNo ratings yet
- Dat Examinee GuideDocument27 pagesDat Examinee Guide1linNo ratings yet
- Circuit JudgesDocument19 pagesCircuit JudgesScribd Government DocsNo ratings yet
- Barrier-Free Washroom Planning GuideDocument24 pagesBarrier-Free Washroom Planning GuideKeshav MehraNo ratings yet
- AT&T Technical Test GuideDocument5 pagesAT&T Technical Test Guideanon_8777166410% (1)
- FED COMPLAINT 2 8 18 FILED - AMENDED 5 8 2018 Bri Stephens PDFDocument63 pagesFED COMPLAINT 2 8 18 FILED - AMENDED 5 8 2018 Bri Stephens PDFPaul Charles D.No ratings yet
- Arthur Jason de Luigi (Ed.) - Adaptive Sports Medicine. A Clinical Guide-Springer (2018) PDFDocument396 pagesArthur Jason de Luigi (Ed.) - Adaptive Sports Medicine. A Clinical Guide-Springer (2018) PDFDL PT&M100% (2)
- Higher Education Law OutlineDocument20 pagesHigher Education Law OutlinestephhuNo ratings yet
- Exam 1 Test BankDocument36 pagesExam 1 Test BankRam Kumar75% (4)
- Rocking The Cradle: Ensuring The Rights of Parents With Disabilities and Their ChildrenDocument449 pagesRocking The Cradle: Ensuring The Rights of Parents With Disabilities and Their ChildrenBeverly TranNo ratings yet
- ACRP Certification Handbook 1Document17 pagesACRP Certification Handbook 1Aishwarya RaghuramNo ratings yet
- Psychology of Gender: PSYC/WOST434, Spring 2015Document11 pagesPsychology of Gender: PSYC/WOST434, Spring 2015Gabz GabbyNo ratings yet
- John Doe v. University of Maryland Medical System Corporation, 50 F.3d 1261, 4th Cir. (1995)Document10 pagesJohn Doe v. University of Maryland Medical System Corporation, 50 F.3d 1261, 4th Cir. (1995)Scribd Government DocsNo ratings yet
- Los Angeles County Jail Plan - 2013Document181 pagesLos Angeles County Jail Plan - 2013Los Angeles Daily NewsNo ratings yet
- Disability EtiquetteDocument36 pagesDisability EtiquetteDisability Rights AllianceNo ratings yet
- Conditional Acceptance For Mandatory VaccineDocument11 pagesConditional Acceptance For Mandatory VaccineAnonymous100% (4)
- Chapter 11 Lodging, Planning and Design QuestionsDocument5 pagesChapter 11 Lodging, Planning and Design QuestionsAbhishek AgarwalNo ratings yet
- Human Resource and Payroll Substantive Procedures: Account BalanceDocument3 pagesHuman Resource and Payroll Substantive Procedures: Account BalancealtheguruNo ratings yet
- Summit County Parking Deck ADA LawsuitDocument21 pagesSummit County Parking Deck ADA Lawsuitemills11No ratings yet
- Judgement by Honorable John J. Tharp Jr. in A.H. Vs IHSA (16-cv-01959)Document34 pagesJudgement by Honorable John J. Tharp Jr. in A.H. Vs IHSA (16-cv-01959)Jonah MeadowsNo ratings yet
- Employee Handbook JCBDocument70 pagesEmployee Handbook JCBJanhvi SaxenaNo ratings yet
- Department of Labor: wc-147 (r7-04)Document2 pagesDepartment of Labor: wc-147 (r7-04)USA_DepartmentOfLaborNo ratings yet
- Integrity Testing: White PaperDocument9 pagesIntegrity Testing: White Paperadedoyin123No ratings yet
- Discussion Board 3 HR Dilemma 1Document3 pagesDiscussion Board 3 HR Dilemma 1api-478028340No ratings yet
- Worldwide Network Services, LLC v. Dyncorp International, LLC, 4th Cir. (2010)Document67 pagesWorldwide Network Services, LLC v. Dyncorp International, LLC, 4th Cir. (2010)Scribd Government DocsNo ratings yet
- Speaker and Speaker-Strobe: FeaturesDocument4 pagesSpeaker and Speaker-Strobe: FeaturesDauXuan HuynhNo ratings yet
- Hosanna Tabor Evangelical Lutheran Church v. EEOCDocument39 pagesHosanna Tabor Evangelical Lutheran Church v. EEOCDoug MataconisNo ratings yet
- MBAC-6450 OnCampus SyllabusDocument21 pagesMBAC-6450 OnCampus SyllabusatoshkhujayevNo ratings yet