te (EGIEA TEE Cano)
7D pasic inronmarion
DEFINITION
‘ene vulgaris isa chronic disorder othe plseba-
caous apparatus caused by abnormal desquama-
ton of foliar epithelium leading to obstucton of
the plosebaceous canal resulting in inlaeation
and subsequent formation of papules, pustules,
nodules, comedones, and scaring. Based on thor
appearance, the acne lesion can be divided into
Intammatery (presence of papules, pustules, and
nodules) or nonnfammatory (open and ciosed
‘umedones) For inlammatory acne sons can be
classied ss papulopustular, nodular. or both The
‘American Academy of Dermatology clasicaton
seme fr aoe denotes the flowing tre levels:
1. Mild acne: Characterized by the presence of
comedanes (Fis. and £2) (nonnflaryma-
‘ory lesions), few papules and pustules (gen-
erally <10), but no nodules.
Moderate acne: Presence of several to many
papules and pustules (10 to 40) along with
‘omedanes (10 to 40}, The presence of >40
papules and pustules along with larger, deep-
nodular inflamed lesions (Figs. 3 and £4)
(up to fv) denotes moderately savere acne,
Severe acne: Presence of umerous or exten-
sve papules and pustules as well as many
nodular lesions (9.5).
SYNONYM
ene
|e0-t0cm coves
1700 Acne vulgaris
170.1 Acne conghobata
170.2 Acne varioltormis
1703 Acne topica
170.4 infantile acne
1705 Bene excoriee des junes files
1708 Other acne
170 Acne, unspecified
1730. Aene keloid
EPIDEMIOLOGY &
DEMOGRAPHICS
+ ene is the mast common skin isease inthe
us.
+ Iti mast common in teenagers, with 85% of
all toonagers being affected to some degree.
‘+ Highest incidence between ages of 18 and
18 yn both genders,
« Involution of the disease usually occurs
before age 25 yr, but 26% of waren and
12% of men will continue to have clinical
acne until the mi-<0s,
PHYSICAL FINDINGS & CLINICAL
PRESENTATION
+ Open comesenes (blackheads, dosed com-
eres whtcheads)
Greases (oy sk)
Presence of scars fom prior acne esis
Various tages of development and sevety
may be present eoncomtartiy
Common cision of acne face, back and
upper chest
Infammatory papules, pustules, and ecaic
pores
ETIOLOGY
«+ Aone vulgaris is exclusively a folicular dis
ease, with the principal abnormally being
comodone ‘formation,
Overactvty of the sebaceous glands and
blockage inthe ducts. The obstruction lads
to the formation of comednes, which can
become inflamed because of overgrowth of
Propionibacterium acnes.
Eracerbated by environmental factors (rot
humid, topical ciate), medicatons (eg
Indie in cough murs, hal greases), nus.
‘val exposure to halogenated hydrocarbons
Mechanical or fctonal frees can aggravate
eristing acne (eg. excessive washing by
some patents to spr them oftheir black:
heads or aiiness)
(}VbiaGNosis
DIFFERENTIAL DIAGNOSIS.
Gram-negative focus
Staphylocoeal pyoderma
‘ene rosacea
Drug eruption
Sebaceous hyperplasia
‘Angiooromas, basal call carcinomas, osteo
mma cutis
(Occupational exposures to ais or grease
Steroid acne
Hiradenits suppurativa
Perioal dermatitis
Psoudtolicults barbae
ilar
Sebortheie darmattis
WORKUP
History ad physical examination:
+ Inquire about previous treatment
+ Careful drug history (hncluding all OTC
products)
Family history history of joe menstrual fares
History of use of cosmetics and cleansers
Oral contraceptive use
Use of medeations that may worsen acne
such as corticosteroids, anabolic steroids,
Ithium, neuroleptics, yeosporine
Consider the possibility of hyperancrogenic
state in all women (sus, regular men
8s, androgenic alopecia) or cilien (ebor
‘hea, acanthosis nigricans, onset of acne
between ages 1 and 7 yr and no obvious
external factors)
LABORATORY TESTS
* Laboratory evaluation is generally nat help
ful Patients who are candidates for ther
apy with isotretinoin should have baseline
lver enzymes, cholesterol, and tigyerides
checked because ths mediation may result
in elevation of lipids and iver enzymes.
‘+ A negative serum pregnancy test or two
negative urine pregnancy tests should also
be obtained in females 1 wi before inttion
of isotretinoin: if also imperative to main
tain effective contraception during and + mo
after therapy wi isoteioin ends because
of its teratogenic effects. Preanancy status
shouldbe rechecked at monthly visi,
+t hyperandrogenism is suspected in female
pallens, levels of dehydroepiandrosterone
sulfate (OHEAS), testosterone (otal and tee),
land androstenedione should be measured
For women with regular menstrual cycles,
serum androgen measurements generally
‘aro nat necessary,
a TREATMENT
NONPHARMACOLOGIC THERAPY
* Blue ght (CleasLight therapy system) can be
sed for eatment of moderate inflammatory
‘acne vulgaris. Light in the vileUblue range
can cause bacterial death bya photoeaction
inti porphyrins react with oxygen to gen-
‘erate reactive oxygen species, which damage
the cell membranes of P acres. Testment
usually consists of 15-nin exposures twice
weekly for 4 wk, Phototherapy may be effec
tive for short-term treatment of acne, but
Jongéterm efcacy and how it compares with
conventional acne therapy is unclear.
Diet: in obese patients, dietary counseling
recommended, high-gheemic diet may
worsen acne, although the strength ofits
ifuence is controversial
ACUTE GENERAL Rx
Treatment generally varies with the type of
lesions (comedones, papules, pustules, cystic
lesions) and the severty of acne. Table 1 sum-
Imarizes an acne treatment algorithm. Fisting
treatment for mid acne vulgaris icudes ben-
209 peroxide, topical retinoid ora combination
tf topieal medications, inusing topical antbiot-
les, Use of topical treatments for 6 to 8 weeks
Is required to judge their efcacy. Table £2
Aesctbes prescription topical therapes for acne
+ Comedones (nonnlammatory acne) can be
treated with retinoids or retinoid. analogs
Topical retinoid are comedolyc and work by
‘normalizing fliclrkeratnizaton, Commonly
avaiable agents are Adapalene (Dien, 0.1%
gl or cream, applied once of twice daly
tararotone Tazorac 0.1% cream or gel applied
ai, tretinoin (Retin-A 01% cream or 0.025
gel applied once daly), tretinoin mirosphere
{Retin-A Micro, 01% gel, applied at bedtime.
Tretinoin i inactivated by ultraviolet ight and
cxiized by benzoyl peroxide; therfore it
should only be applied at right and not used
concomitant wih benzoyl peroxide.
+ Tretinoin is pregnancy category C and taza
tene is pregnancy category X Salicylic acid
preparations (eg, Neutrogena 2% wash)
have keratlyte and antinlammatory orop-
etios and are also useful in the treatment of
‘comedones. Large, open comedones (lack-
has) shouldbe expressed,
Pationts shoud be roovaluated ater 4 to 6
wk, Benzoyl peroxide gel (2.5% or 5%) may
be added i the comedanes become inflamed
‘or form pustules, The most common adverse
fects are dryness, erythema, and pooling.
‘Topical anites (erynromycn, clindamycin
lotions or pads) can also be used in patients
with signicant inflammation, They reduce P
acnes inthe pllasebaceous flicle and have
@ Acne Vulgaris 17
TABLE 1 Acne Treatment Algorithm
‘Severity (Lesion Type)
Ta avon ot Save niente? Sr
wan Ban Me nmin ASS ay
epeal caps
5 sbsan ef nvacangares 2 swat eseitans
ay be condi pla of ucla.
neces era yoann sn bul stan.
a Zagt Teas OM Beet cate et
clay neal oes aap 0% nominate Dae,
rc a rape Pea, 05 hat Da a ae st ae
thugs erat 765-8208: Cae Hea argent oer arepar am 2 Gna Aire snore Ozone ite, JA ced Dera Sap 1-3 2003.
‘some antiammatory effects. The combina
tion of S% benzoyl peroxe and 3% enytro-
mycin (Benzaryci) or 1% clindamycin with
5% benzoyl peroxide (BenzaCln) is highly
effective in patents who have a mixture of
‘comedanal and irlammatary acne lesion.
+ Fixed-dose combinations. of clindamycin
phosphate 1.2% and totinoin 0.025% are
availble (Velin gel, Ziana) and are more
effective than ether product used alone:
however. they ae much more expensive than
the individual goneric component.
+ Pustular acne can be tested with tretinoin
‘and benzoyl peroxide gel applied on atemate
evenings; orying agents (sulacetamide-sufa
lotions [Novacet, Sufacat) are also effec:
tive wnen used in combination with benzoyl
peroxide; orl antibiotics (dxyeyclne 100
img qd or enjtromycin 1 ad given in 2 to
3 did doses) ae effective in patents with
moderate to severe pustuar acne. Patents
not responding well to these anbiaties can
be switched to minocylne 0 to 100mg bid
Tablo £3 summarizes oral antics for aene
vulgaris.
«+ Patients with nodular cystic acne and those
with moderate to severe inflammatory acne
unresponsive to topical drugs can be treated
with systemic agents: anbioties (erthromy-
cin, tevacyaine, doxyeyeline, minocycie),
isotretinoin (avaliable on a restricted bass).
(oF oral contraceptives. Periodic intalesionl
‘riamcinolone Kenalog) injections by a der
Imatologst are also effective. The possibilty
‘of endoctinopathy should be considered in
patients responding poor to therapy.
+ Isotretinoin isthe mostetfectve drug availabe
for treatment of severe naduleyte acne is
Indicated fr acne esstant to anit thera-
pyand severe ace. tints P aonescolon-
“ation by reducing sebum production and has
antinflammatory and keatoic effects tis
avalable only on a restricted basis. Dosage is
0.5 to 1 mghalday in 2 dvded doses (max-
‘mum of 2 mg/day); duration of therapy is
generally 20 wi fora cumulative dose 2120
g/kg for severe ost ane. Before using tis
‘medication paionts should undergo baseline
laboratory evaluation see “Laboratory Tests")
This drug is absolutly contraindicated during
Pregnancy because of is teratogenicity. It
Should be used with cautgn in pants with
history of depression Physicians, cstrbuos,
pharmacies, and patients must reise inthe
|PLEDGE program (nm pledgeprooram com)
before using isottinon
+ Aula acid is a bacteriostatic dearboxiie
acid used to normalize Kerathization and
reduce inflammation. can be used in preg-
rant women,
+ Oral coniraceptves reduce androgen lev-
‘ls and therefore sebum production. They
representa useful ajunctve therapy fr all
‘ypes of acne in women and adolescent gs
Commonly used agents are norgestimate/
ethinyl estradiol (Otho Tr-Cyclen) and dro-
spirenonelethiny estradiol (Yasmin),
REFERRAL
Referal for intlesional injection and derm-
abrasion shouldbe considered in patients with
severe acne unresponsive to conventional
therapy, Tele E¢ summarizes altemative veat-
ments for acne vulgar
PEARLS &
CONSIDERATIONS
‘+ Gram-negative folicultis should be sus-
pected if inflammatory acne worsens after
several months of oral antbati therapy.
+ Acne may worsen during the fist 30 4 wk of
retinoid therapy before improving,
COMMENTS
Indications for systemic therapy of aone are:
* Painful dep papules or nodules
«+ Extensive lesions
= Active acne with
hyperpigmentation
+ Pationts morale
Pations shoud be educated tat in most cases
‘acne can be controlled but not cured and trat
atleast 4 to 6 wk of inal therapy should
bo required before significant improvement is
noted,
+ The nogatve psychological effect of acne
‘may be severe and long-lasting
severe scarring of
SUGGESTED READINGS
‘valable a ExperConsult com
RELATED CONTENT
‘Acne (Patient information)
‘AUTHOR Fred er MD
Acne Vulgaris
TABLE E2 Prescription Topical Therapies for Acne Vulgaris
Drug Brand Formulation
‘sbiotics
Clnaamyein Chola 1% seat, gl pleats, ton
Cindalax eaten
Clidets 1% ples
Cindogel Hoe
Evoain 1% foun
lnc? Beran 1% 61482 gel
use 1% (5% 8 gel
Deana 12% 25% BP gel
Onexon 12% (8.75% 87 gol
Dapsone Dezane 5% oa
Enitroryen Linge Eel 29a
Ener nay, Stat 2% seuton
‘Stan 1.5% sokten
ne mycin 2% cirtment
TheramyeinZ 2% ston «28
Enptronyen* Benzamycin 3% (5% 8) gel pa
Sulfacatarice Kron 10% tion
Pein 10% (6% sully clots, wash
Ciena 10% (3% sult era, wash
Pasula 10% 4 sur wash
oa ais Drlex 20% ream
Retinoids
Posen iter 0.1% ream, ge, ton
03% gl
aaoabene BP! Epidve 01% (2.5% BP gal
Taartene Taree 005, 0.1% cream
005, 0.1% gel
Fable 01% foam
Tretnon Fetnek 0,028,005, 0.1% cream
101, 0025% gel
fati-A Mico 004,0.1% gel
ta (0.028% ream, gel
Dale 0.08% gel
Tretnocnsanycin Zana 0.028% (0.2% cladamycn ge
vain (10254 (1.2% cladanycr gel
7 ero pre ie ale
‘ted ae nat: a sve Many ese rps hve ert enti
‘onan bey pot.
"a Pale, ae Hawt eines pete mabey» bok af i oe ot ads asco
5 Pei, 20, Che
171
Acne Vulgaris 1722
TABLE E3. Oral Antibiotics for Acne Vulgaris:
Drug Usual Dosage" ‘Comments/Side-Etfects
Commonly wed
Tetacjine 250-500 m9 Dental taining <9 yt
Dairy produce decreas absarpton
upset, hoses, teratogenic, PTC, WE, 8D
Mireyane 50-100 mg Dental taning <2
55,65, 20,105,118 mp ER airy produce decease absorption
it mpg once dit
‘artigo (ower incidence wi E preparation) lyse. ue-ay skin pigmentation, severe dg reactions
‘th epaspreumentis,Lpuslke rasta, 8, teralaganc, heats, PTC, WC, BO
Dowyeytne 50-100 mg Dna taing <2 yr
75,100, 150 mgER. once aly produce deraase abserton
sai
20mg (‘subantimcotial ——_—Photosnstvty.pholoaychaysi, Gl upset fare teratogenic, PTC, WE IBD
dese’)
Enthromn 250-500 m9 6 upset (commor, WC rug-cugmaractons, logan ofthe GT rt no longer reammanded by
tet experts gen Iceated eitance
Lass commonly used
Trimetboprin 0/400 m, 160/800 mg Severe drug resctons 48, bone marion supeston, heats, upset, NC had drug exupton: une
tullameiocazoe se for acre stony scauaged
‘ncamyein 75.150 m9 Pseuderembranous colts upset, drug reactions, WE
Cephalexin 280-500 m5 upset, rug eaions We
[ede ese rn: gastos 8D, itera bowl eae PT
“Guay ee day or ace rs cows rtd le
From Plo Ai A Mr clncl ed ati tek kn srs of cn and ascent , hse, 206 Ee,
rome coer 55 Snare one VE wll cand,
TABLE E4 Alternative Treatments for Acne Vulgaris
‘Treatment Comment
‘oecone extractor Perermed win eomedeneoxarlor
Inectons Invalesona tiancioiore ected to ge ots notes
Unt teapy Bue ight ray potoinatvae acres
Aaclight (nay have atinlanmatory tect
Combination eed ight
bense pulse ght PL)
Proiodynasc therapy POT)
Laser therapy A pulsed dye ase araly use)
Reuraing leer nsing bah naralatve and bli recuracing hes) uel for acne cating
Dermaarasenidemasinng eet for aoe seating
Colagn jctn Use for acne searing
Chae! pets Use for acne seating and yperpimentatin
Punch gratsssueaugmen set fr ace scaring
‘Wehbreacte ais set for aopic ane sear
Fasten tetany ‘Outdated medaty
[Panam ton pep
From Pater AS Mand A acne ped emriey atc kn srs of chishn and dolce, 5, heb, 206, Ese
7D pasic inronmarion
DEFINITION
‘Nopic dermatitis is @ genetically determined
‘ezematous eruption that is pur, symmet,
and associated with personal amily istory
of allorge manifestations (atopy) Box | sum-
marzes criteria fr atopic dermattis, Modified
criteria for children with atopic dermatitis are
Aeserbed in Box 2
SYNONYMS,
Eczema
‘pic neurodermatis
‘pic eczema
|ep-t0cm coves
1208 Atopic dermatitis, unspecified
120.89 other atopic dermatiis
EPIDEMIOLOGY &
DEMOGRAPHICS
+ Incidence is between 5 and 25 cases/1000,
persons
Highest incidence is among children (10% to
2094) accounts for 4% of acute care pal-
ave visits, I affects 1% to 3% ofthe adult
Population.
Onset of disease before age yr in 85% of
patents
‘+ More than $0% of children with generalizes
atopic dermatitis develop asthma and allergic
‘hints by age 13 yc
+ Concordance in monozygotic twins is 77%,
PHYSICAL FINDINGS & CLINICAL
PRESENTATION
+ AMopic dermis presentation can be subi
vided nt three phases:
1. cue: Vescular, crusting, weeping erup
tion
2 ‘Subacute: Dry, sly, erythematous pap-
ules and plaques.
3. Chronic: Liceniication fom repeates
seratching
+ The lesions are typically onthe neck, face
Upper trunk, and bends of elbows and knees
(eymmetsc on flexural surfaces of extrem
ties) (Fo. 1, A. and Fig. 2). Atopic derma.
Its lesions are usualy ciscrete but vaguely
delineated, scaly and erythematous.
‘There is dryness, thickening ofthe involved
areas, discoloration, blistering, and oozing
Papular lesions are frequently found in the
antecubital and popliteal fosae,
In chien, red scaling plaques are often
confined to the cheeks and the perioral ana
perinasal areas.
‘+ Hertoghe sign: Loss of the outer eyebrow
ftom ehranc ubbing (ig. 1.8,
+ Constant scratching may result in areas
af hypapigmentzion or hyperpigmentation
(ore common in backs).
BOX 1
Criteria for Atopic Dermatitis,
Major erteria
Must have tvee ofthe followin:
© Pras
+ Typical morphology and distribution
+ Flenaral ichenieaton in aduts
+ Facal and extensor involvement In infancy
+ Chronic or enrerically relapsing dermatits
* Personal or family history of stop disease (e.,, asthma, allergic rhinitis, atopic der
mattis)
Minor criteria
Must algo have thee othe following
= Xerosis
+ htyosis or hyperlnear palms or keratosis pars
* IgE react (mediate skin test reactivity, RAST test positive)
* Elovatod serum IgE
+ Early age of onset
+ Tendency for cutaneous infections (especially Staphyloceccus aureus and HSV)
* Tendency to nonspecific handioot dermattis
+ Nipple eczema
© Chel
+ Recurrent conjunctivitis
‘+ Dennie-Morganinfrarotal fold
* Keratoconus
* Anterior subcapsular cataracts
+ Orbital darcening
«+ Facil pallor or facil erythema
+ Piyriasis aba
* ch when sweating
+ Intolerance to Woo! and tp sovents
* Porifolicuaraccentuation
+ Food hypersensitvity
‘+ Course inuenced by environmental or emotional factors
* White dermatographism or delayed blanch to cholinergic agents
Sw Herpes apes its: I, erunoghbuln E: AAS! rasalergoenent asa,
From les WD st at Arcos" dresser! she 12, Phsdpie, 216, Saunders,
In adults, redness and scaling in the dorsal
aspect ofthe hands or about the finger are
the mast common expression of atopic dr-
malis; oozing and crusting may be present
+ Secondary stin infections may be present
(Staphylococcus aureus, dermatophytosis,
herpes simplex.
ETIOLOGY
Unknown; elevated T-ymphocyte activation,
Aetectve cell immunity, and B-cell gE overpro-
ction may play a significant rok.
(}yoIeNosis
DIFFERENTIAL DIAGNOSIS.
* Scabies
* Psoriasis
Dermat herpetiorm
Contact dermatitis
Photosonsitity
Seborheie dermatitis
Candidiasis, tea
Lichen simplex cronicus
Other: Xerosis, impetigo, Wiskot-Aldrich
syndrome, phenyketonuria, ichthyosis, HN
Germatiis, nonummular eczema, histo-
cytasis X, malignancies (T-cell iymphomal
mycosis fungoides, LettererSive disease),
raft-versus-host disease, metabole and
hutrtional deficiencies (zinc, niacin, pyt-
oxine deficiencies)
BOX 2 Modified Criteria for
Children with Atopic
Dermatitis
Essential
= Prtus
+ Eczema,
+ Typical morphology and age-
specie pattern
+ Chronic or relapsing history
Important features
* Ear age at onset
+ Atopy
‘Personal or fay history
+ IgE reactivity
= Narosis
Associated features
+ Alypicl vascular responses (eg. facial
pall, white dermstographism)
+ keratosis paris, ichthyosis, or hyperin-
ear pains.
+ Orbital or periorbital changes
= other regional findings (e.g. perioral
changes, peraurcua lesions)
+ Perifolicuaraccentuation,lchentieatio,
or peurigo lesions
atures
@ Atopic Dermatitis
FIG. 1 A, Fiesral atopic dermatitis wth ichanicaton, Many ofthe skin changes are secondary to scratching.
Linear eheniteation, as shown here, and excoratons are ype B, Hertoghe sign: Los ofthe outer yebron
may occur in haat paint a a result of cri ubting. rom We GM, Cox NA eds: Diseases of the
‘shin coor atas and texted 2, St Lui, 2008, Mosby)
Table 1 summarizes characteristics and c=
cal features of disorders in the dferental
agnosis of atopic dermatis
WORKUP
Diagnosis is based on the presence of tree of
te folowing major features and three minor
featus,
[MAJOR FEATURES:
Prius
Personal or family history of atopy: Asthma,
allergic rhinits, atopic dermatitis
Facial and extensor involvement in infants
and children
Flexural ichenifistion in aduts
[MINOR FEATURES:
Elevated IgE
Exzema-pertolicularaccentuaion
Recurrent conunctvtis
letnyosis
Nope dermattis
Woo! intlerance
Cutaneous $. aureus infectons or herpes
simplex infections
Food intolerance
Hand dermatis (nonalergic rian
Facial allo, facil erythema
nels
White dermographism
Ely age of onset (after 2 mo of age)
LABORATORY TESTS
Lab tests are generally not helpful
Elevated I levels are found in 80% to 90%
of atopic dermatits
+ Cans by ony t et
shew teanen
(Qi reearmenr
NONPHARMACOLOGIC THERAPY
© Gp al decrease arson sn
+ frucnc of tary te
1 Sulion tongue aes, sweating
low hay Oe wer
2. Sone wth tag ssace
wot tole ome sap ad
ort tne)
3. Feds tt poke excels 9
toon peau fn oy wet
4 Stoo
5 Hlogens an at
& Sete ns esting
« Putoray uray maybe fects
invent aoe
ACUTE GENERAL Rx
+ Emollonts can be. used to provent dry-
ness. Severely fected skin canbe optimally
hydrated by occlusion in adaton to apolea-
tion of emolients.
+ Low-potony topical corticosteroids (0.9. 1%
to 25% hycrocortisone) may be helpfl and
fare generally considered first-line therapy.
Use intemedite-poteney steroids (e.9. i-
amcinoioe, fuocinolone) for more. severe
cases and limit potent corticosteroids (e9
belametrasone, desoximetasone, clobetasol
to severe cases. Tale 2 summaries relative
potencies of topical corticosteroids.
(rsaborole 2% ointment i a phosphodi-
esterase typed (PDE) inhibitor modesty
effective for shor-term ‘reatment of mild to
moderate atopic dermatitis
Oral antihistamines (@.9.hydroxyzine,
tiphenhydramine) are effective in controling
paris and inducing sedation, restful seep,
and prevention of seratcing during sleep.
Doxopin and other teylic antidepressants
also have antihistamine eect, induce sleep,
and reduce pratus
The topical Immunomodulators pimecrolus
and tacrolmus are especialy useful or reat-
ment of the face and inertginous sts,
where steoidinduced atrophy may occur
However, due to concems about carsnogenic
potential the FDA recommends imiing ther
use for short periods in patients who are
Intolerant or unresponsive to other weatments
Pimecroimus cream 1% applied bid and has
antinlammatory eects secondary to block-
age of activated T-call cytokine production
Tacrolimus ointment (0.03% or 0.1%) applied
bid is @ macrolide that suppresses: humoral
and cell-mediated immune responses,
‘+ al prednisone, niramusculrtiamcinolone
Goeckerman regimen, psoralen and utavioit
Aight therapy are generally reserved for
severe cases,
‘+ Cyclosporne, azathioprine, mycophenolate
and interferon gamma are sometimes ted
‘or recalcitrant disease in adults by physi-
cians wo specialize in severe inflammatory
skin condos.
‘+ The human monocional antbody dupiumab
is effective in adults with moderate to sovere
atopic dermatitis that have not responded
to topical therapies. tt can be used with or
without corticosteroids. tis injected subeu-
taneously. Cost isa lmiting factor.
4 Table 3 summarizes the management of
topic dermatits
DISPOSITION
+ Resolution occurs in approximately 70% of
patents by adulthood.
‘+ Most patints have a course characterized by
remissions and intermittent fares.
SUGGESTED READINGS
Avalable at ExpertConsultcom
RELATED CONTENT
Dermatitis Patient information)
Eczema (Patent Information)
AUTHOR: red er MD
185
sioposia pue
1s Atopic Dermatitis @
TABLE 1 Differential Diagnosis of Atopic Dermatitis (AD)
Main Age Group
Affected
Frequency” (Characteristics and Clinical Features
seer bats common ‘Saimor-red greasy sa lesions, often on te scalp (rae cp)
cate ‘and raphe are: geeraly oresens in th frst 8 we af:
‘peal lars win weaks
saber esate common tamalous patches wth allow, white or rash scales in seb-
amats trae sens, paricllythe sap cenval face and eter
chest
rma Chere ane aus common ‘Coin-shaped scaly eles, masty on es and butecks usualy
emats ravten
tant contact Chen an acu common out t tri ezemateus lesan, mst confined tothe sie
ermatts of exposure; story of lal appl inant is a sk facto
righ coos wih AD
Alegl onact den ane suits common Eczema rsh with masinum expression at shes o ares xp.
eats sce but might pread story of cay apie rani 2
Fak acer, might coma with AD
Lieto sine este common (ne or more cae ckcumscribed,cherifes plaques tht
cronies result rm repelive seractng or bing because of itanse
teh
Asti eczema ate common ‘Sealy sured pate of crate ovryng dy sin, mos ten
on over les
Infectious Skin Diseases
Dermatopyte Chen ane ate common ne or more demarcated scaly plagues with cent clearing and
inecton slg ried redaneseage vara eh
Ingetiga criden common Demarco ertematous patches wth ster or honey yl
crusting
sealer eriden common! ety sper turows and pustules on gals and sola,
Between fingers, and on geal ig produce secondary
tezoratous changes
HY (here ane ats Uncommon Sebathestke ash
Keratinzation Diss
Tentyossvalgaris fants and alts common Ory skin with ne sealing, pata onthe lower abdomen an
‘censors; perfolicuar skin augheing: paar hyper~
linen: fal form (2 FLGmtatons uncommon: cen
coon wre ad
Nutritional Deficioney-Matabolie Disorders
dine efiency Children Uncommon Eryharatous scaly palches an plaques, mas ofn around the
(acotematis mouth and ana rae congenital frm accompanied by ahaa
Ferteropatica) and abpeca
Bion decency bons Uncommon ‘Sealy perioral deat, ape, conjunc, tary
(euro or Typotnia
Dtinaredaiceney)
Palogra iain Mages Uncommon Sealy crusted epidermis, desquamato, sun-exposed areas, ar
celery, hea
wasboton bats anderen oogrptic lak say dermatits, swollen in with races pong patches
‘oendent
Prenshetonuia bats seamen ematous rash, hypesigmentatn, onde ha, developmental
‘alay
Neoplastic Disease
Culnonue Te ats Uncommon Etyemalous ps troan acu and lags witha fies
lymphoma pry espnsive otal caress val ite
ery stages)
Langerhans cot bats Uncommon ‘Sealy and pupurie dermal, nepalosplnamepay cjopeiar
Fistoyais
‘Caen appetinaty ih otoT ie commen = 1a 12011 00: are 1 100 tin 10.00% 1 in 9000.
From Mgmnt Nan Tak Peds 21, Peis, 2020, Shave,
@ Atopic Dermatitis 17
TABLE 2 Relative Potencies of Topical Corticosteroids rom Most Potent to Weakest) wa
Class Drug Dosage Form(s) ‘Strength (%)
Tiara
Ange vanes cx os
Se
cx pre ce nt os
seme per
‘prt etre com tos uy
seamen Spon cram iu en os p
ees tem rer re i
nesses er vos
Davee ste oan oes |
Psa Ga re tn eos
vane ce eam ne 08
14 om ty
brace let crams i en os
Poca mee Oran ime oor
fro em oe tos
tone eos oem o
Trane ie am ie EB
‘awe eto ay
rete ne oe rn 2
Pecans com
ow ny
ence Ge gm eo tos
Pcie ete rm ston oo
one pny
a oean 03
weer Ge i in oases
Pere so one ro os
From Fair AS, Monee Hn inal pated a ebook an arr of ison and gee, 5,201, Ee
TABLE 3 Management of Mild, Moderate, and Severe Forms of Atopic Dermatitis,
wi Moderate Severe
ating and baer par ating ad barre par Bathing ard baie par
‘ccane oferta and Serge ogee ‘rose of wan and serge ogee Aceanee ofan nd lege Wiggers
btemiterehoeterm usecase Var top-_Inarmtent, tartar ue of he IV topical Clas I top tro fr ae; cae S- tap terie +
sted + top caineven ino ‘sods = toplal acneun nibs ‘azrolms omen fr maliennce
Treatment of suprnecton Tweament of suprnecton Treatment of supernecton
Oral aninstamiee Oral anthstamines
‘Systemic aninammatry agents, revi ight therapy
"Bark epar maybe aarp by plein ot fei eas 9 ar reap ae
From Por AS Mace A art al pets drmty nk kn adr ae and decency, 5,201, Eee
Bullous Pemphigoid Ezrs
PHYSICAL FINDINGS & CLINICAL enon, cast! (nd ay te
CD BASIC INFORMATION) Prescirarion trgotri cowering ene nb)
rsront poncho dees, tem
DEFINITION Tsenes ate pacing cpr
Bullous pemphigoid (BP) is a chronic, autoim- 1, Non-bullous phase: Starts as excoriat- ‘ins, sulfasalazine, acetylsalicylic acid, non-
mune, subepidermal blistering disease com- ed, eczematous, papular, or urticarial ‘steroidal antiinflammatory drugs (NSAIDs),
‘monly seen in the elderly. Itis the most common plaques characterized by extreme pruritus: dipeptidy! peptidase IV inhibitors (gliptins),
sree tent hoe sions ore: 2. Bil pase ecu tay monhe Tse mrad vcs
‘toses. Other related diseases in the pemphi- later and is characterized by formation of * Additionally, there are several reports of UV-
OF atl time ences amsebltan is rhb on ince etadan Pare nuces BP
cicatricial pemphigoid (MMP), anti-laminin 332 flaccid after rupture '* BP patients are significantly more likely
pont, Buty amp ot, PANSIEAL FHS 1 fae Youn eno rg
laminin gamma-1 (anti-p200) pemphigoid, and —* Anatomic distribution: sclerosis having the strongest association;
Str napountSoneemeacainte 1"Hsurtcs of he ams ad legs, sor Dprdaorr denen soa
IgA bullous dermatosis (LABD) and epidermoly- groin, axilla, chest, and abdomen; gener and Parkinson disease are also associated
Shuts scusta G98 ote ome aM Sy esther mk ina?
sedate eal hrecercedty aes; 2. Wein nentane mene een in
Groulecsemeicsnnenancenes| "tow low apaens foam pent (DIAGNOSIS
Srbtonet mere te pal ieee he omar wih
ara ft) Digs Is based on a contnton ef
svmonves ‘+ Lesion configuration: clinical, histologic, and immunotluorescence
& {Pay bebeled np t 20% fees fining Dec inmneuorecenes
Penh (ecteiies neateapron ar tosne isos ste go sed fea
fronted medal toy ning tea oe ee
2, Berta jae an emo oneal pans of pa ase
te-toe cone
ster andmayraolesyoaromt ae hevlpe aye disses and
120 Bulls pempnins fiome semoeen mlances, and medication hisry over
+ Let maha ope Cron, sab coe BF
EPIDEMIOLOGY & PRMT eC tue meaning 93 Sd be Ngan‘. oon
DEMocnaPnics tin lett an eg Gecroe_ sity pater peng wi aeertaed
"tat common e te ainnute buss “Song Chenaernemalor__ fer fontearig iss wie mozota
Somos dred eas iia se rele reer and yg te hee nck
cee eer ate yay 2 Re ten Tgnre Wo send of Th dagen be nee wi he
Weslo ncating owns yon endetbusastctsrupun nda on pt
‘satis mat nea 9 Myo eg Tate BP ctr: Tee of ew de
STEGUEC Rian deta apne 3. Hea wine seri bt may nw "fees (ae S75, rc, nes
Metmetevate a's cae Seem guctntanmaty hpenbmaraton o,f shane of Bla sone on
Itoposonyrin te US andor fon teem fan rd ne ps enn ete 96
2.4 to 42.8 cases per 1 million person-yr in and/or C3 deposits along basement mem-
Europe. person ETIOLOGY brane on DIF microscopy
«Eee seminary rxsin con, = Atcmmane dase wh munegbu- 2 Sn bp) Evans 60a atemet
caer Sy cy'aettene "bn. andl C3 complet ey matic aothoge on eto
Se se andesncond en BPISO a BBEID)_mureers (mee
a ea tng ne! end h be oleral bueno new”. Sknbepy eon ae BF0 an
entot te ecioningeing cast _ bare roe erat thao ye ctatncesonenme
seinimaateceerttueccr + Bpindaed pemphigoid. athoagh Ink immuraon sy LN
age 80, luncommon, can occur in patients "2k EEERENTIAL DIAGNOSIS
+ Bullous arthropod bites
* Linear 1g bulous dermatosis,
* Dermatits herpetiformis
«+ Aati-laminin amma-t(an-p200) pemphigois
Brunsting-Pery pemphigoid
Bulous systomic lupus erythematosus
Mucous membrane or cicatricial pemphigoid
Epidermalysis bulls acquista
Pemphigoid gestainis
Bullous erythema muttforme
Generalized fxed drug eruption
Impetigo
Porphyria cutanea tarda
Blous lichen planus
Pemphigus wulgars
Paraneoplastic pemphigus
Table Ef compares some ofthese immuno-
bullous aiseases
FIG, E1 duilous pemphigoid. Large, tense bullae ae seen onthe lower region ofthe abgomen inthis
18-year-old boy. Tom Pall AS, Manca Al Hurt cna pedlae damatology textbook o kn car. © LABORATORY TESTS
rs of childhood and adlescence, a8, 201, Philadelphia, Elsevier) * Histology of lesional skin
27406
Bullous Pemphigoid @
TABLE E1 Immunobullous Skin Diseases
Immunobullous Targeted Protein or Tissue
Disease Clinical Prosentation Sorum Autoantibodies Structure Immunotiuoresconco*
Pemphigus Dermatoses
Pemphigus wigs Flaccid bullae on nonin-
flamed skin, crusting,
postive Nis sign}
‘commonly atfets scalp,
chest intertiginous
areas, and oral mucosa
Superficial bulla, erosions,
‘and scale with cresting,
Epidermal IgG and C3 call
surface staining
IgG epthtal cel suiace;
conelates with disease
activity
Desmoglin 3 and
desmoglein 1 ofthe
desmasome
Pemphigus foliaceous IgG epithelia cel surtace
comelates with disease
Desmoglein 1 of the
desmasome
Epidermal IgG and C3 cell
surface Staining
positive Nikolsky sign? activty
Paraneoplastic. Flaccid bulla, lchenoid or g6 epithelia el sutace Desmoglin 3, desmo- Epidermal IgG and C3 cell sur
pemphigus erythema muitforme and basement membrane pak 1, desmopla- fae and basement mem-
ike, usually inoWes 2one anng on kin 2, PAG, envo- brane zone staining
mucosa, often exten- rodent bladder eitielum paki, perpaki,
sively includes esopha- is charactersto):cove- ater proteins ofthe
geal and respiratory Ines wih cseaseactvty —_desmasome and
areas hemigesmosome
9A pemphigus Faccid bul, similar to ighelthlia cell surface: Desmocolin ofthe Epidermal igh call surface
pemphigus vulgaris corelates with disease desmasome staining
actviy
Pemphigold Dermatoses
Bullous pemphigoid Tense bulla, offen on urt- IgG basement membrane _—_-BPAG2, BPAGI Linear basement membrane
‘carl base, prominent one, epidermal hemidesmosome, zone IgG and C3
pruritus amin Wcida
Mucous membrane or Tense bullae and erosions, IgG basement membrane BPAG2, laminin 382 Linear basement membrane
teal scaring sequelae Zone, epidermal (previously known zone IgG and C3
empnigoid as laminin § or epi-
gti), hemidesma-
some, lamina lucida
Pemphigoid Tense bullae, similar to bul- Complement xing, base-_BPAG2, BPAGI Linear basement membrane
gestationis lous pemphigoid; onset ‘ment membrane zone, hemidesmosome, zone C3
uring or immediatly epidermal Tamina lucida
ater pregnancy
Tense bullae; commonly
‘curs in areas of ta
sma arin orl mucosa
Linear basement membrane
zone IgG and C3; may show
linear igh and gM
Epidermolysisbulosa
scmusta
IgG basement membrane
zone, dermal:
‘Type Wt collagen,
anchoring fons
Linear igh butous Tense bulla, similar to IgA basement membrane __97-K0 portion of LUnear basement membrane
dermatosis and bullous pemphigoid oral zone, epidermal rarely BPAG2, hemides- zone IgA
chronic bullous dis invoWement common in derma ‘mosome lamina
ease of childhood ‘adult disease Tucida
Dermattishorpat Small bulze on extensor ‘IgA endomysial and vans- Epidermal ransgluta- Granular basement membrane
formis| surfaces (elbows and slutaminase antibodies; mminase zane IgA with siping in
ven) markedly prurt- correlates with disease oral papilae
ic; assocated wit ines-_actvty and compliance
tial gluten senitvity with gluten-free det
Bulous lupus Tense bulla, photodstib-WyG basement membrane Type Vi collagen near basement menbrane
erythematosust uted zone, dermal ‘anchoring fois zone gf may stow grrr
IgM and C3 basement mer
rane ze asin bps band
Sp) 2204 ml prin a | G2, Dba pr ati canna ange ca et
snatuinera Gp bt rags ant ee seer Serie ts
"wala sata eben tn Raman pl ny ae! rere om
From inant os ln alr esa pte oP, 2016 Sura,
1. Light microscopy: Subepidermal bullae
wth eosinophils and/or neutrophils with
associted eosinophil andor neutrophil
‘ermal ntitvate
2, Direct immuncfuorescence (DIF) miros-
copy (gold standard}: Linear and or C3
deposits along dermoepidermal junction
+ Immune serological tests. sot: Only confi
matory with DIF microscopy findings
1. Indrectimmunatuarescenc Crating
IgG ant-basement antibodies using mai
NaC-separated normal skin as sustate
2. EUSA: Test for ant-BP180 IgG; if nega-
tive, test for an-8P230 gd
a TREATMENT
Bullous pemphigoid may be a sel-limited ds
aso, but Is course may last ftom months
to yrs, Treatment is based on the degree of
isease invoWement and the rate of dsease
@ Bullous Pemphigoid 27-7
progression; however, there is no general con-
sonsus on how to determine disease severity A
European guideline defines severity by percent
skin involvement, with ess than 10% defined as
nil, between 10% and 20% defined as mader-
ate, and grater than 30% defined as severe,
NONPHARMACOLOGIC THERAPY
+ Mild soaps with emolients to wt skin after
bathing
+ Use ofronadhernt kes nth case fon
‘Se eos lesions to prevent betel supe
‘ecton minimize pai ar prorat reaing
> Only ran larger blisters and leave the biter
toof intact as a natural essing; remove fue
tering skin only in broken bistrs
+ Avoid mechanical trauma tothe skin
‘STAGE-SPECIFIC THERAPY
* Mild: Topical cass | steroids daly
+ Moderate: Class | topical steroids dally sys
temic therapy may be added as needed
‘TREATMENT-RESISTANT
‘THERAPY,
‘THERAPY
‘Once dsease contl is achioved with oral
storolds, begin tapering corticosteroids by
25th at 7- to TM-day intervals; if induction
tose is less than 20 may, taper over 2- to
4-wook intervals,
+ Severe: Clas topical steroids daly in com- + If relapse occurs, return to dose given two
reduction intervals prior can resume taper
ator 14 days of disease control lesions.
bination wih systemic immunosuporessants
+ Inalesional tiameinolone acetonide to 0-
lated lesions “© May adé or switch to adjuvant agents as
+ Oral antihistamines to contro pruritus needed.
TETRACYCLINES
+ Daxyoydne 100 mgtwiedalyissinfarinefoc. lesions
tiveness to oral prednisone, with decreased
‘Se eft compared wth ol steroids.
+ Tetacyeline 500 mg four times dally pls rico
tinamie $00 mg thoe tims daly had simi
ceflectveness as predrisone 40 to 80 mg dally.
SYSTEMIC STEROID INDUCTION
THERAPY
* Prednisone (or equivalent) 0.5 mg/kg per
ay, which can be combined with adjuvant
+ Disease contrl is defined 28 no new lesion
{ormaton concurrent with healing of exsing
DISPOSITION
SUGGESTED READINGS
BageIS et al: Bulbus rerpig,Atoimmun Rev 185} 445-455, 2017
Baan & et a: Pemphigus wiya Is the most common auonmune bulous
lsease in Norhuestrn Romani, int J Dermatol 49(7:788-774, 2070.
Baum $ et a: Diagnosis and easteaton of auoimmure Misting sare,
‘Autorun Re 144-5) 482-£88, 018
Bene J ela Bullous pemphigoid and dipepyl peptidase W iis: a case-
nenease study in te French Pharmacoglance Databese, Br J Dermat!
1752286-201, 2016
Bia WP et a Localzs buleus pemphigoit on sts of raaterapy and
lymphedema inte sare patent Inan Dermatol Onn J Supp 23S101—
3103, 2014
Brick KE ela Icdence of bulous pemphigoid and mortally of pts with
bullous pemphigoid in Ose County, Mnnesca, 1860 through 208, J Am
‘Acad Dermatol 82-88, 2014
Cots B et al: Atommune bullous disease Swiss stusyG: morality of bulous
ompignid in Switzerland: a prospectvestuty, Br J Dermatol 1652) 388-
374,201,
ia Funte Set a: Postracaton bulouspemphiel ininfany- report of tree
new cases an trate review, edt Dermat 308)74-744, 2013
Di Zanzo Geta: Bullous pamphigot rm the nc ate bench, Clin Demate)
s0()16, 2012
immunasuppressve therapy, including aza-
thioprin, dapsone, doxyeycie, methotrex-
ate, and mycophenolate mofetil
+ Ina doses greater than 1.0 mgikg of pred-
risolone show Ite added beneft
«+ Intravenous immunoglobulin therapy 2 g/kg
er oft (4- to 6-week intervals)
‘+ Immunoadsorton or plasmapheresis
“+ Rituximab (ani-cD20) 1000 mg W on day 1
then day 14 or 875 mgimé IV administered
four times at weekly intervals
SYSTEMIC CONSOLIDATION
+ Relapse is defined as greater than three new
lesions per mont or one lesion greater tan
40m that does not heal spontaneously
in one week or progression ofthe exsing
lesions or emergence of daly purus.
In the Unites States, moray rates are est-
mated at between 11% to 23% after 1 yt,
Standardized morality ratios range trom 1.90 to
6.6. BP isa chronic disease; exacerbations and
relapses are not uncommon, even in success-
fully treated indviuals, A recent prospective
study reported 45% relapse rate of the evalu-
able patents a 12 months, with the majority of
felapses occuring in te frst 6 months afer
cessation of therapy n this study, an ELISA ther
soore thee times higner than the normal cutoff
valu at time of therapy cessation was the main
predicting factor for 8P relapse within the next
Dementia and intial extensve disease may
be two additonal independent risk factors asso-
ciated with relapse during the fist ro harap.
REFERRAL
Dermatology
PEARLS &
CONSIDERATIONS
COMMENTS:
* Pruttus can be the presenting complaint
and can precede the appearance of any skin
+ Bullous pemphigoid should be high on the
diferental in paints over 70 yr old with
tense bullae,
+ Exemely prrtc uricaral plaques can pre-
‘cede onset of tense bulla by months
+ Doxyeycine 100 mg twice daily is equally
effective tool prednisolone,
RELATED CONTENT
Bullous Pemprigos Patent Information)
‘AUTHORS: Sara Mora Tuehayl, MO, snd
achiuC Lee, MD, MPH
ming ta: 5 guidelines for he treatment of pompigus vgersotacous
and bullous penphiat isch Dermat Ges 13)8833-844, 2015.
Falcin tat Management of buleus pemphigt the European Dermatology
Forum consosut in calibeaton with the European ade Of Deacon)
‘ed Vneresogy, Br J Demata 172 887-877, 2015.
Feel Feta: Cinical and immroloi ators ascorited wit bllous peg
‘goirelapse curing the first year of treament a muiceie, prospecive study
JAMA Dermatol 1501) 25-38, 014
lsohashi Fo aA case of bulls pemphigoid exaoerbstad by iadaion ate
breast conservative radteray, J Cin Oncol 811-813, 2011
ily Petal: Incidence and mortal of balous pemphigoid in France, J vest
Dermata13281898-2004, 012.
LYE, Yew YW Lambert WC: Bulous pmghigaé adits association wth eo
loi eeeaser 8 systamati review and mela-nais, J ur Acad Demalal
Venere! 30(12 2007-201, 2018
‘sha 0, Lprtay 6, Grenae T: Bulous pemphigl folowing ajant radio
‘therapy fr breast cancer, Beast J 172:204-205, 201,
‘Sear ta Buloue pomprigndinauces by easoterapy recur on recha:
lenge, cn Exp Dermat! 87(8)916-817, 2012
Wiams HC aa Dorje versus predaisoln as an intalweabrant stony
for bulois pemphigod: a pragmatic, norinerory, randomised controled
a, ance 380079)1630-1638, 2017
fm Dermatitis Herpetiformis 49 ©
7D pasic inronmarion
DEFINITION
Dermatitis herpetiformis (DH) i an autoimmune
bisterng disease that Is considered to be a
cutaneous mantestaton of celia disease (CD).
Its associated with gliton-sonsitve enter-
‘pathy in near all cases though only 20% of
Patients have gastrointestinal symptoms. 15%
to 25% of patents with CD vill have DH
SYNONYMS,
DH
Dunring disease
|ep-10cm cove
113.0 Dermatitis herpetiformis
EPIDEMIOLOGY &
DEMOGRAPHICS
PREVALENCE (IN US): 11 cases per 100,000
persons per yr prevalence for CD is one in 133
adults
PREDOMINANT SEX: Male predominance (2:1),
however, female predominance in chien
PREDOMINANT AGE: Fourth decade a Ie, but
can occur at any age
PREDOMINANT RACE: Most common in
Caucasians of Northern European ancestry
GENETICS: oth CD and Di have a stong
genetic component. 10% to 15% of patients with
DH have a frst-dogree relative with ether DH
or CD. Specific HLA genes (involved in process-
ing giadn angen in geneteally susceptible
Indviauals) have also been shown to predispose
to developing DH (HLA-DQ2 in 90%, DOS in the
remaining 10%). However, les than 50% of
genetic predisposition i atbuted to HLA genes.
PHYSICAL FINDINGS & CLINCIAL
PRESENTATION
‘Classically, the lesions of OH aro small,
‘rouped,“herpetiorm” vesicles that are ds-
‘rbuted symmeticaly on extensor surfaces
(elbows, knees (Fig. £1], scalp, back, and
buttocks). However, due to Intense prurtus
and scratching, pinpoint erosions and exco-
riations in the above distribution are often
‘he most prominent fndings on examination,
wth ntact vesicles rarely seen,
“Spontaneous improvement with oytc exac-
ebation is common,
+ Celiac-type enamel defects to permanent
teeth oral vesicles, or palmoplantar purpura
have boon ropored as potential associated
‘indings
PATHOGENESIS
(0 and DH are both autoimmune-mediated by
immunoglobulin A (ig) class autoantibodies.
Dietary glten is carta tothe pathogenesis in
both. In genetialy predisposed individual, tis
hypothesized thatthe gluten by-product, an,
complexes with tssue ranslutaminase (6) in
‘the gut binging a8 an antigen to HLA-DQ2 on T
calls, creating an immune response that results
in antTG IgA antibodies (Le. atiendomysial
antibodies) in the blood. 176 cross-reacts with
‘epidermal TS (eT). The blood of CD patents
with and without skin disease is found to have
both skin and gut ant-T6Ig8 antibodies. Ye, t
is thought thatthe high-affiity Ig against eT
{erm complexes that are responsible for i. The
deposition of lgA-eTS complexes inthe papillary
dermis triggors an immunologic cascace result
ing in neutrophil recruitment and complement
acivation
(}ybiaeNosis
Physical examination and routine histopatho
‘ogy ae often suggestive of DH; however, ect
immunofluorescence (OIF ofa perlesional skin
biopsy has pathognomonic findings and is the
gold standard for diagnosis. Fig. 2 describes an
approach othe pation with suspected derma
‘tis herpetiformis.
DIFFERENTIAL DIAGNOSIS
+ Cinically and histologically, the etferential
dagns's includes:
1. Linear igh dermatosis
2. Bullous pemphigoid
5. Bullous lupus
Those diagnases canbe differentiated by DIF
on prisionl skin biopsy
Other ania diagnoses to consider
4 Scabies (check for inesigitl burrows
and invclverent of genitalia)
2 Arthropod bite (papular urtcaria over
exposed areas)
3. Eczematous dermaits ll-defined weep-
Ing erythematous plaques)
44 Herpes simplex or zoster infection (pain
ful not symmetric)
5. Generalized prurtus (no blter history)
WORKUP AND LABORATORY
TESTS
* Evaluation for gastrointestinal. symptoms,
family history of DH or CD and prurts shoud
be sought in patents with suspcted DH
+ Lesional skin biopsy: Wil demonstrate 2
noutopti-rch subeplermal bulla and rule
out many conditions.
‘+ DIF of normal-appearing perilesional skin
biopsy: Wil demosstate pathognomonic Ink
epost localized to the dormal papillae
and dermal-pidermal junction ina granular
patter
+ Serology (enzyme-linked. immunosorbent
assay [ELISA for Ig tissue transgltamin
ase, ELISA for Igh epidermal transgltamin
ase, if avalable, and indirect immuno.
rescence for yA endomysialaniboces (otal
IgA) can be used to aid in the agnosis of
DH in cases where the OIF is negatve or
‘equivocal, or for monitoring disease activity
response to treatment. hough these ci
culating antibodies n the blood exist, there
is high false-positive rate for antssue TS
and fo antiendorysal antibodies (one tia
of DH patients are negate for aniendo-
mysial antibodies}, and their absence does
not exclude the diagnosis. Also, IA-defcient
DH patents may aso nave negative serologic
results. Those with th prosence of circulat-
ing antibodies wil have a reduction in levels
in response to treatment adnerence
a TREATMENT
[A gluten-tee det (GFD) and dapsone are con-
sidered first-line therapy and are often started
in connection
+ GED mproves symptoms ofboth Gland skin dis-
ease, wih Gl responding queker (kin responds
attr 2 mo. A reespectv study showed rmis-
Son 2 yr witht symptoms) in 12%
Dapsone results inimproverent of skin mani-
festations within days but does nat teat Gl
manifestations. Dapsone is typically tapered
cover time, while felong gluten avoidance is
oten necessary
+ One study demonstrated GFD alone was
comparable to GFD plus dapsone in the
‘weatment of DH; hence GFD is an essanil
‘component inthe treatment of Di.
NONPHARMACOLOGIC THERAPY
+ Fist line: GD:
1. Avoid barley, re, wheat (can consume
ric, com, and oats)
2. Consultation with a cletitan is recom-
mended
‘3. Most patents need to follow let indet-
ritely; however, cases of spontaneous
remission have been reported,
+ Second line: Elemental it (controversa
1. Can consider elemental det aveidance of
hole proteins) in those patents wo do
not adequately respond to a stict GFD;
however, data are limited.
ACUTE GENERAL Rx
«Fist lne:Dapsone:
1. Inia dose 25 to S0 mg PO daily with
(gradual increase to an average mainte-
nance dose af 0.5 to 1 mg/kg daly ten
maintenance dose of 100-mg dal.
2, Glinical_ monitoring weekly is recom-
mended to aptmize dose (optimal dose
is when 1 to 2 new lesions
‘3, auton: Dapsone may produce hemalyis
(especialy if G8PD deficiensy),agranu-
locytosis, methemoglobinemia, systemic
tug hypersensitivity reaction (DRESS),
and a peripheral neuropathy.
4, Baseline labs: CBC, LFTs, O6PO levels
‘tar te intition of therapy, monitor CBC
every wk x1 mo, then every other Wk x2
smo, montaly 3 mo, then every 3 o 4 ma.
Monitor LETS every 3 to & mo,
+ Seconds aternativs:
1. Sulfpytidine (00 to 1500 mlday, com-
Pounded. medication) or sulfasalazine
{600 to 1000 mg bd) may be substtuted
in cases of dapsone intolerance or inthe
rare case that neuropathy develoos.
2. Case reports of efficacy using topical
dapsone 5% twice daly In patients who
o not tolerate oral dapsone; also report-
@® Dermatitis Herpetiformis «us
jopsies
+ Lsional punch biopy for RE
+ Perfesional punch ropa for DIF
biopiy rents
Monterey
iG. 2 Appr
ey te aa
ane
es
Tm
Beri,
{Aaa A
“Screening for associated diseare
Del poote
SDE ld peocoe st
eke "
+ Ober Buoimmane sera
Soved Texan focings
«onal bod near
+ Total
+ An
eae
Consider genetic testing
+ HIADQ2, HAD OS:
ipa ‘analysis
ach tothe patient with suspected dermatitis herpetiformis, DH, Demattsherpettoeis DIF srctimmunaorescence: eT, epidermal ans-
jutamiase; HAE ematonin and eosin; HLA-D02hstocompabailty locus atigen haleype DO2: HLA-DOS, itecompatity lous antigen haplotype DOB;
‘mmunoglouln; 6, tetanus immune globulin, (rom Balatn 0, Petrone-RascV Dermat herpetfornis: ar. Diagnss, mangement. and progress, JA Acad
ermata68:1027-1083, 2011}
tobe effieacious as an ajuvant oor
dapsone.
3. Uncontrolled studies and case reports
have suggested eficacy wh tetracy-
lines, nicotinamide, cyclosporin, colch
cine, and heparin,
+ Symptomate rele for orurtus:
1. Potent and superpotent topical cortcnste-
roids (atrophy with prolonged use, iit
to 14 days per mo), nonsedating anis-
famines twice dally, sedating anthiste-
mines at bedtime, menthalatd lotion
‘CHRONIC Rx
‘As DH Is considered to represent the cute-
noous manifestations of CD, Ielong avoié-
ance of glen is typically’ recommended
Information about educational resources,
‘such as national and local support groups,
should be provided (ve.clac.0),
+ Patients with DH and CD have an increases
risk of developing Hashimoto thyroid
(60% with thycoid disease). non-Hodgkin
Iymphoma, and Gl lymphomas, An increases
incidence of other autoimmune dlsoroers
(ype 1 abetes melitus, pernicious ane-
Ina, Addison disease, viligo, systemic lupus
erythematosus, rheumatoid artis, and
Sjogren syndrome) and osteoporosis have
‘also been reports.
1. Screening for tyrold disease (TSH, ant-
thyrod peroxidase antibody tes) spl
cally commended,
2 Screening for autoimmune connective
tissue diseases should be considered if
there are suspicious signs or symptoms.
3. Routine screening for Gi lymphomas is
controversial
REFERRAL
+ Dermatologist for skin biopsy and manage
ment of cutaneous disease
+ Gastoenterologist fr evaluation of CD
+ Nuttionist to educate patients about glter
free diet
+ National support groups (wwwrcelia.org)
and local support groups
PEARLS &
CONSIDERATIONS
+ Classic areas invoWed are those that are
exposed it ina “fetal poston,
Lesions may be worsened by iodides and
certain NSAIDs; systemic steroids inetectve
+ Location of biopsies is IMPORTANT: False-
negate DIF can result if biosies are taken
from Iesional skin (should be taken trom
normal-appeaing skin adjacent to lesion) as
agnostic IgA deposits are usualy destoyed
by the blistering proces.
+ GFD results in reduced IgA in skin on DIF
(with eventual dsappearance) and reduced
antendomysial antibodies in the blood.
Hence, serologies (.g.,aniendomysial ant-
bodies) can be used to monitor degree of
compliance to dietary gluten restition.
+ Some studies have suggested a possible pro-
tectve effect of GFD against intestinal m=
phoma. first-degree relatives do not appear
to be at increased risk for Gl or systemic
lymphomas in the absence of DH or CD.
SUGGESTED READINGS
Available at ExertConsultcom
RELATED CONTENT
Cela Disease (Related Key Topic)
AUTHOR: Lisa K Pappas-Tater, MO
seston
sioposa put
ews Erythema Multiforme (19 ©
7D pasic inronmarion
DEFINITION
Eythema multiforme is an intammatory disease
characterized by eruption of annular, maculo-
papular lesions with dark raised, erythematous,
or vesiculobulous center surrounded by a pale
zon. tis believed tobe caused by immune cm-
Plex formation and subsequent deposition inthe
skin and mucous membranes. It fs considered
a byporsonstity reaction to infection or drugs.
SYNONYM
=m
|ep-t0cm copes
51.0 Nonbullous erythema multiforme
L518 Other erythema muliforme
51.9 Erythema multiforme, unspecified
EPIDEMIOLOGY &
DEMOGRAPHICS
PREDOMINANT AGE: 20 to 40 yr
RISK FACTORS: Often assorated with herpes
Simplex and oer infectious agents, drugs, or
connective tissue diseases
PHYSICAL FINDINGS & CLINICAL
PRESENTATION
‘+ Prodrumal symptoms ae mid or absent. thing
fr buning atte se of erupton may osc:
‘Symmetric skin lesions (Fig. £1) with a
Classic “target” appearance (caused by the
centrfugal spread of red’ maculopapules to
circumference of 1 to 3em witha purpuric,
cyanotic, or vesicular center) ae present (ig.
2), The papules may enlarge into plaques
measuring afew centimeters in dameter
with a dark or red central parton (Fg. £3)
Target lesions. may ot be apparent for
several days and generaly heal in 1 to 2 Wk
tout scaring,
“+ EM lesions are mast common on the face,
back of the hands and feet, and extensor
aspect ofthe forearms and legs (EM mar.
Trunk involvement can occur in severe cases
EM majo,
+ Urticarial papules, vesicles, and bullae may
also be present and generaly indicate EM
major.
‘+ EM major bullae and erosions may also be
present inthe ora eavity. The mast common
sites are the Ips and buccal mucosa,
ETIoLocy
+ Immune complex formation and subsequent
depostion in the cutaneous microvasculature
may ply a role in the pathogenesis of ery:
‘hema mutiorme.
4 The majority of cases folow outbreaks of
hetpes simplex vs 1 and 2
+ Mycoplasma pneumoniae, fungal infection,
medications (bupropion, sulfonamides, pen
ellis, nonsteroidal antintammatory drugs,
barbiturates, phenothiazines, hyantans).
+ In >80% of pationts no speci: cause is
ident.
(}yoIGNosts
DIFFERENTIAL DIAGNOSIS.
* Chron urticaria
Pityriasis rosea
Contact cermatits
Pompigus vulgaris
Lichen planus
Serum Sickness
Drug eruption
Grandloma annlare
Polymorphic ight eruption
Vial exantema
Stevens-Johnson syndrome (8)
‘oxi epidermal nazralysis (TEN)
Bulous pemphigoid
Vial exantnems.
+ Leukocytoctastc vascults,
«+ Lupus erythematasus
Secondary syphilis
WORKUP
‘+ Modical history with emphasis on drug
ingestion,
* Laboratory evaluation in patients with sus
pected colagen-vascuar diseases
+ Skin biopsy whan diagnosis is unclear
Fig. E1 Erythema multiforme (EM). Round erthemtous swolen plaques and target lesions on the
alms. Tis il developed EW in association wits her systemic pus erythematosus. rom Pall AS, Mancin
‘A: Huns inal petatc dermatology a textbook of skin disorders of childhood and adolescence, ed 8,
Philadel, 2016, lav
LABORATORY TESTS
+ Complete blood count wih dierent, ele-
vated ESR
+ Atinucloar antibody
+ Serology for Mycoplasma pneumoniae, HSV-
1 HSV-2
+ Blopsy for atypical cases
* Direct immuncfuorescence if suspecting
bullous diseases
RX} TREATMENT
NONPHARMACOLOGIC THERAPY
+ Mil cases gonraly do nat equ treatment
lesions esove spontaneously within mo,
+ Potential drug preciptants should be
ACUTE GENERAL Rx
+ Treatment of associated diseases (e.g. vala-
cycovie oF famecovr for herpes simplex,
cexythromycin for Mycoplasma infection),
Dapsone, antimalarials, or azathioprine for
sovere or resistant cases,
Prednisone 40 to 80 mgitay for t to 3 wi
effective for decreasing inflammation and
pain and may be tried inpatients with many
target lesions; however, the role of systemic
stores romains controversial
LLevamiscle, an immuncmodulator, may be
fective in the treatment of patients with
chronic or recurrent oral lesions (dose is 150
mglday for 3 consecutive days used alone or
in combination vith prednisone.
1V immunoglobulins in severe cases
Antimicrobial therapy i indicated if. pneu
‘moniae isthe trigger of EM.
DISPOSITION
‘The rash general evolves over a 2-wk period
and resolves within 3 to 4 wh without seating
‘A severe bullous form can occur (se entry for
*Stevens-Jonnson Syndrome")
REFERRAL
Hospital admission in patients with suspected
Stovens-Johnsonsynrome
PEARLS &
CONSIDERATIONS
COMMENTS
‘The risk of recutence of erytema mutforme
exceeds 30%%, Recurrence may be treated with
valacylovr 500 to 1000 mgiday, facile 125
to 250 mg/day oracyclr 400 mg bd. Dapsone,
antimalarials, azathioprine, or eychosporne use is
reserved for cases resistant to antvials,
RELATED CONTENT
Exyhama Multforme (Patent information)
Stovers-Johnson Syndrome (Related Key Tops)
AUTHOR: Fre Fee, MO
9 sasic inronmaTion
DEFINITION
Erythema nodosum (EN) is an acute, tender,
frythematous, nodular skin eruption resulting
‘rom inflammation of subcutaneous fat, atten
associated with bruising Its the most common
‘orm of panniculitis,
‘SYNONYM
eN
eD-10¢M CODE
152. Erythema nodosum
EPIDEMIOLOGY &
DEMOGRAPHICS
INCIDENCE: ts the most common form of pan-
nicultis, Two to three cases/100,000 persons
ery
PREDOMINANT SEX: Forale:male rato of 3
toa
PREDOMINANT AGE: 25 to 40 yr
PHYSICAL FINDINGS & CLINICAL
PRESENTATION,
+ Prodromal symptoms of fatgue, malaise,
upper respiratory infection symptoms. may
precede eruption by 1 to 2 wk
+ Auto onset of tender nodules typical locat-
‘eon the shins and occasionally seen on the
‘highs and forearms Fg. E),
4 Tho nodules are usvally 1/8 to 1 Inch in
dametor but can be as lage as 4 inches;
‘hay begin as lott rd lesions, then become
Garker and often ecchymotc. The nodules
heal witin 8 w without ulceraton
+ Assocated findings:
1. Fever (60%)
2. lymphadenopathy (<50%)
3. artralgia (64%)
44. ‘Signs of the underying ines
ETIOLOGY
Cell- mediated hypersensitivity reaction is seen
‘more ‘requendy in persons with human louko-
ct antigen (HLA) BB. The lesion resulls ftom
fan exaggerated Ineracon between an antigen
and cell-mediated immune mechanisms lead-
ing to granuloma formation. Up to 85% of cases
Of EN ae idiopathic.
Infectons:
* Bactera:
1 Campylobacter
8
4
5
6
1
8
8
10.
1
12
13.
14
15,
Streptococcal pharyngitis (28% to 48%)
Salmonelientertis
Yorsinta enters
Psittacas's
Chlamydia pneumonia infection
‘Mycoplasma pneumonia
Meningococcal infection
Senora
Sypils
Lymohogranuioma venereum
Tularemia
Cat-sratch cisease
Leprosy
Tuberculosis
+ Fung
1
2,
3
4
Histoplasmosis
Coceidnidomyensis
Blastomycosis
Tichophyton verucesum
= Vises:
1
2
3
Cytomegalovirus
Hepatitis B
Epstein-Barr ius
Drugs (3% to 10%):
Sulfonylureas
Sulfonamides
Pencins
(ral contraceptives
Gold sats
Prazosin
Aspirin
Bromidos
Sarcoidosis (11% to 25%)
Inflammatory bowel disease
Hodgkin disease, non-Hoagkin ymphoma
Ankylosing spondylosis and reactive arthrop-
athies (eg. associated with inlammetory
bowel disease)
+ Beicet disease
Latgrn syndrome
+ Acute myelogenous leukemia
(yoinewosis
DIFFERENTIAL DIAGNOSIS
+ Insect bites
Postraumate ecchymases
Vasculitis
Wober-Chrstian disease
Fat necrosis associated with pancreatitis
NecrooiassIpoiica
Scleroderma
Lupus pannicutis
Subcutaneous granuloma
16 Erythema Nodosum
WORKUP
* Physical examination
+ Diagnass of underyng less. by istry,
physical examination, and laboratory tests as
Indicated
LABORATORY TESTS
«+ Erythrocyte sedimentation rate
Throat culture and antteptoiysn Other
Purid protein derivative
Others. depending on index of suspicion
(eg, stool euture and evaluation for ova
and parasites in patients with diarea and
gastointestinal symptoms),
Skin biopsy in doubtil cases:
1. Eaty lesion: Inlaation and hemor
‘hag in subcutaneous issue
2, Late lesion: Giant cels and granulomata
IMAGING STUDIES
Chest radiograph to rule out sarcoidosis and
tuberculosis
gq TREATMENT
‘Tho disease is sled and treatment is
‘symptomatic, EN nodules develop in pretit-
ll locations and resolve spontaneausly over
‘several weeks without scarring or ulceration,
Treatment of underyng dsordors,
Aidance of contact Iritation of affected
areas.
Nonsteroidal antinfammatory crus for pan
Systemic steroids (prednisone 1 mglkg of
body weight/ay, tapered over several days)
may be useful in severe cases if underying
risk of sopsis and malignancy have been
ercluded,
Potassium iodide gen as tablet 800 mg ti
(oF a5 a supersaturated solution (five drops
‘ree tmesiday in orange juce) has bean
reported as etlective for symptom conto
+ Invalesonalcortcosteoi irjetions for per-
sistent lesions
PROGNOSIS
Typical case:
+ Pain for 2 vik
luton within 8 wk
RELATED CONTENT
Erythema Nodosum (Patent information)
Sarcoidosis (Related Key Topic
NoTHOR Fre Fer, MD
539
seston
‘spiosg pur
Fira Folliculitis °16
9 pasic inronmarion
DEFINITION
Folicults is inflammation ofthe har flice as
a result of infection, physical injury, or chemical
ination
SYNONYM
Sycosisbarbae
|ep-t0cm coves
1729 Follicular ystof skin and subeuta-
neous tissue, unspected
173.1 Pseudoolicults brbae
173.8 Other specie flicuar disorders
166.2 —Folicuts dcalvans
166.4 Folicultsulerytnematosa retouata
166.3 Pesoliclts capitis abscedens
EPIDEMIOLOGY &
DEMOGRAPHICS
PREVALENCE: Staphylococcal flicults is the
most common form of infectious folicults: i
‘occurs mast commonly in persons wih diabe-
tes. Gram-negative focus occurs in patients
who have had moderatly inflammatory acne
for long periods and have been teated with
long-term anbiotics such as tetracycline.
PREDOMINANT SEX: Sycosis barbae occurs
most frequent in men who have commenced
shaving,
PHYSICAL FINDINGS & CLINICAL
PRESENTATION
‘+ The lesions generally consist of pabfl yel-
low pustules surrounded by erythema: a cen-
ral har is presontin the pustules. Furuncles
vt pus may be present
Patents with sjcosis barbae may intally
present with smal flicular papules or pus-
ules that increase in size with continued
shaving: deep flicular pustules may occur
surrounded by erythema and swelling, the
Upper lips frequent involves
‘+ “Hot tub" folicultis occurs within 1 to 4 days
afer the use ofa hot tub with poor chloe
hatin. tis characterized by papules and
pustules (Fig. £1) with surrounding erythema
(generally affecting the tors, butocks, and
limbs (9. £2.
ETIoLoay
‘Staphylococcus infection (e.
bae), Pseudomonas aeruginosa
‘olicults)
Gram-negative folliculitis (Kiebsiel
Enterobacter, Proteus) assciateé with ant
biotic troatmont a acne
Chronic iitation of the hair folie (use of
cocoa butter or coconut ol chron itation
from workplace)
Initial use of systemic corticosteroid therapy
(steroid acne), eosinophilic folicultis (ADS
patents), Candida albicans mmunocompo-
mised patents)
+ Piyrosporum orbicuare
(}ybiaNosis
DIFFERENTIAL DIAGNOSIS.
‘+ Pseudotolicultisbarbae (ingrown has)
«Acne vulgaris
+ Dermatophyte fungal infections
«+ Keratoss plans
* Cutaneous candidiasis
+ Supericial fungal infections
= Wiles
WORKUP.
‘Physical examination and medical history
(@9., use of hot tub: "hot tub” flicutis
adolescent patients vino have started sha:
ing: syeosis barbae: use of occlusive topical
steroid therapy: Staphylococcus fliclts.
+ Gram-negative fliculis in acne patents on
prolonged antibiotic treatment manifests with
superficial pustules 3 to 6 mm in diameter
‘lring ut from anterior nares or futuant,
deep-seated nodules.
LABORATORY TESTS
+ General not necessary.
* Gram stan i useful to identity the infective
organisms in infectious focus and to der
erate infectous follculs rom noninfectious,
a TREATMENT
NONPHARMACOLOGIC THERAPY
‘+ Prevention of chemical or mechanical skin
iritation
+ Gljcemic conto inaiabetcs
+ Proper chlorination of hot tubs and spas
Shaving with a clean razor
ACUTE GENERAL Rx
+ Cleansing ofthe area with chlorhexidine and
application of saline compresses to involved
sea,
+ Application of 2% mupiocin ointment or 1%
relapamulin ointment for bacteria folios
afecting aimted ar (9. sycossbarbae.
+ Treatment of severe cases of Pseudomonas
folicultts with eorotoxaci
+ Treatment of S aureus flicults with dilx-
aca 250 mg qd for 10 days,
* Isovetnoin is the treatment of choice in
gram-negative flicultis,Amoxiclin or TMS-
‘SMX canbe used whan scretinoin is conta-
indicated or canna be tolerated,
CHRONIC Rx
+ Chronic nasal or perineal S. aureus caries
With frequent folicults can be treated with
rifampin 300 ma bid for 5 days
‘+ Mupitocn or retapamulin ointment appli to
ares bids also effective for nasal caries,
DISPOSITION
+ Most cases of bacteral folicults resobe
completly wih proper treatment
+ Steroid foliculits responds to discontinuation
ofsterias,
PEARLS &
CONSIDERATIONS
COMMENTS
Patonts shouldbe instructed in good personal
hygiene and avoidance of sharing razors, tow
tls, and washalaths,
RELATED CONTENT
Folicultis (Patent information)
AUTHOR: Fred Fe, MD
FG, E2 Pseudomonas hot foot syndrome, Tender papules anépapuloousiuls on tre plentaraspect of te
foot Cute of a swab rom ora ofthe pustules grew P seruginasa (Courtesy John J. Van Aa, MD. Frm
Palle AS, Mancini A: Hurniz einal pediatric dermatology a txtook of shin cists of eihood and
adooscones, 4 5, Placephia, 2016, Elsevier)
FIG. E1 Paputes and pustules in het tub fl-
eultis, (From Klagman RM eta. Nelson textbook
of pais, ed 18, Phacalpia, 2011, Saunders)
Em Food Allergies
7D pasic inronmarion
DEFINITION
Food alleges are divided into IgE-medieted
and Immunologicaly mediated non-gE reac-
tions. They include & spectrum of cisorders
that involve adverse immunologic responses to
iotary antigens.
leD-10cm coves
780. Adverse food reaction (including
anaphylactic shock)
78.1 Other adverse food reactions, not
slsewhere classified
1272 _ Dermatitis ue to ingested food
721,010 Allergy o peanuts
791.011 Alergy to milk products
221.012 Alergy o eggs
781.013 Alergy to seafood
291.018 Alergy to other foods
791,02 Food additives allergy status
EPIDEMIOLOGY &
DEMOGRAPHICS
INCIDENCE: Food alergies have a cumulative
incidence of 64 to 8% forthe fist 3 yr of If.
PREVALENCE:
+ Overall prevalence is 1% to 2% in general
population, -3.9% to 834 in chide,
Patont sol-reparted food allergies have a
prevalence of 12% to 13%, demonstrating
the importance of objecive measures. in
assessing fod alrges
Nearly 40% of children with food allergy
have a history of severe reactions that if not
rated immediately with proper medication,
can ead to hospitalization or even death
There Is insucent evidence to conclude a
racial prediction (Greenhava, 2013).
GENETICS: Children with parents or close rela-
tives with allergies may have a tendency to
become allergic to foods
PHYSICAL FINDINGS & CLINICAL
PRESENTATION
‘+ Iof-mediated reactions: (within minutes to a
few hous) Prurtus, urticaria or angioedema,
atopic dermatitis, Gi symptoms, conjunctival
injection, sneezing, nasal congestion ino
‘hee, bronchospasm, and anaphylaxis
Non-igf-mediated reactions: Food-induced
fenteocolis, celiac disease, Crohn disease
dermatiis herpetiformis, and_ pulmonary
reactions such as Heiner syndrome, These
lhesses are discussed separately
Signs, symptoms, and presentation reflect
spectic allergic manifestation, but in food
allergies there is @ reproducible temporal
relationship to ingested food allergens.
ETIoLocy
Failure to establish tolerance to food antigens.
1L-33 mediated epithelial permeabity ang Th?
Gupta AS at a The prevalence, covery nd at
baton of clchand fod algy in he Unies States,
Peds 1288217, 2011,
skewing result in senstizaton to food proteins
which ace presented to primed T cells. Food
processing condone that may affect allergenic
activity ae described in Table
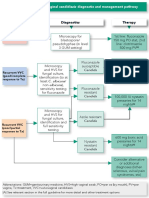
Dx} DIAGNOSIS
+ Thorough history (o ident specific food's,
‘quantity consumed, timing, and nature of reac
tion) and physcal exam shoul be perormed.
‘The temporal relationship and reproduc
ily of the symptoms are most important to
establishing the diagnos
‘review of Ingredent abels may be helpful
Confirmatory testing can include skin testing
or in vito testing
Skin prick testing (SPT): Postive predictive
Value mes pu pezset
po soon nse oe
‘sanpadd py esse000 Hn aun
ms nen sea aa i n i le EPI
‘ye step see,
nen
ry pare-yod oo a NBA
suopeayduy eaquHg|
van
su -sods 09
)
ito us ue)
‘puede ‘ez
86 omeg
aide yoweg
we00y
vid
‘uepyng aA POD
ane Brseaoa say pun oes aye suoREyDOUL
spb pssanad-pu Aianze
ue manus puosusuep-aong 204 ue! subse EN
SLL pur i) subioye ura p aumongs ap sap uN
‘suse sy pu ‘3 yj anon a 8
"a}0m Bupeca a
pat ate ses way yoroute
hand ue! ung $2 pu ea] AueBGrs UE ey,
‘onas oiey ago yn Uo sobs 9
“omongs o-apeu ear S47 4 Ale uedns YUE
‘aupoul ae sfouey | a8 age
fueadne yea
Faupout a sfojuoy 1 meg eT
‘tof an ay w pac sys Yo SoBe Yo #807
bess bu 0 so)
‘sens tuum pa tasune pungsodg
"na usu,
yt pareduco ou s+ fyb 90)
‘eos tno penta stojuou 1m 9g wash
‘suabsaiy wo Buysseo01g yo yeu
onepuztog
sepmad ayy 600
panuaises put tu PauuDe
nds jase ys
su spo jo woes
ty pu unseoy
og
pu ep ay
sn pezzeied jo wgaseey
pu sat
us
“ffi fq 220 0 perowy
sgn pu
nates 1) sodsoune poupoR
Buyss20014 Jo ame
Sayssoo fapuncas
fwsseoi Keung
afi Gusseo01g
‘Aunnoy o1ueBioiry iooyy AeW 1eUL suoRIPUOD BuIsse00i4 poos | TEV.
sm Food Allergies @ @
‘pues yr wt
19 sea pr syed ae seagate SKY WH,
aNosos 0 Sug ioe 5009
cu oso asp ova 3 feu PEG
9 Aiae aubrey sarge 4G
oun
ajucwag se
spas sue Jago yan uzun w pas ae 2b
uy au pu Asa sep Jo aNEU
siopeosne3 oad 1u op so yraead pays,
‘sysfs seromgus 64 vonduns.o 14
ES paepsuo ave yo wrens pauyes Aub 2
‘sun oie
om
nego
sats pu ous 809
sraead ureokos
e680
‘ayn a0
od ao aseseg enue
pnesu jo ved Buea 1a,
pos Bune ayn ha po
teu 658
pauruns “0 paseoodueeg
i pepnp 9 Ae spe pony
sued
spo) passzovtun so. um paseduoopaypou fn
‘om fen safetag Sapo ya pue sabe Su
‘wo fans] pus Ab an usd
rosa pu stood Suse Bp porous a 544
‘9u9pIN3 eRe -ODg
‘suabioiy wo Buyssoo0ug Jo yoeduy
00) poe
$00) poe
28
you 0 pape st sp0oy wnt
awa 10
sept poo peri
Buysse001g Jo oimeN a8 BYSEBO01g
‘Aunnoy o1U06:0ITy you ABW YUL SUORIPUOD BUISSOD0g Pood | TTEVL
@® @ Food Allergies 57
eee)
Sa hae
oop) onder
Pawnee
becave of
“raced wih
oil
ay
ge
z
peste eae Napa a
‘npleasd food Hered
a Tope Tagalog
aaa
ed ed ed ed
Toute alah wai
genni as sey =a)
ie ewehcon || spony on
lod ‘reed ae
orig
FIG, 1 Algorithm forthe management of food allergy “Testng ndats skin-prck testing radoalergo
sorbent ests (RAST) gy a3, anor pach testing Note tat clnical symptoms must be associate with
‘he foot) alts posite before he foots) tou be eliminated frm the dt "Orl foot challenge (OFC)
imlvesreincocucng the fod and observing for sins!symptoms of fod allrgy (Treatment of food allergy
Imvlves elimination tthe caurate fod} fa theca
+ Wheat allergy found to resolve by 5 yr of age
and soybean alrgy by 2 yrof age
PREVENTION
+ There is conflicting evidence regarding the
protoctve effect of breastfeeding on food
allergies.
+ There is no evidence to suggest that exch
sive breastfeeding for 6 mo or more is supe-
tir to exclusive breastfeeding fr 4 to 6 mo
in terms of developing fod alrces.
In high-rsk infants wo are not exclusively
breastfed, here is limited evgence to sug-
gest that feeding with hydrolyzed formula
compared to cow's mik formula reduces
allergies
Currently thee is no evidence to support the
use of prebiotics andr probiotics or the
prevention of allergic diseases.
No current evidence exss to support delay-
ing the Introduction ot solid foods beyond
06 mo,
‘+ The eatyinaducton of peanuts significantly
decreases the frequency ofthe development
of peanut allergy among chilien at high
risk for this allergy and modulated immune
responses to peanuts.” Enly peanut into-
duction (ages 4 to 11 months) lowers the
Fisk of developing peanut allergy by 80%
‘compared with peanut introduction after age
5yt
‘In rovent phase 3 tals of oral Immuno-
‘therapy in chilten and adolescents who
were highly allergic to peanut. treatment wth
ARIOI resulted in Ngner doses of peanut
protein that could be ingested without dose-
limiting symptoms,
PATIENT & FAMILY EDUCATION
Information can be found on American
‘Academy of Allergy, Asthma and Immunology
"apa RS ot a: The provance covery, and dit
but of hood food alargy ine Unites Stats,
Plats 122-217, 2011,
(owaeachor), the Food Allergy and
Anaphylaxis Network (wo. foodallrgy0°),
and the Anaphylaxis. Campaign (ww. anapryl
avis. 09.
REFERRAL
Patients maybe referred to an allergyimmunet
‘ogy specialist when the diagnosis is uncertain
orf avoidance measures are not success
SUGGESTED READINGS
‘Availabe at ExperConsut com
RELATED CONTENT
Food Allergies Patient Information)
‘AUTHOR Fre. Fer, MD
72.02 MU Us male)
7D basic inronmarion
DEFINITION
Impetigo is highly contagious superficial skin
Infection generally caused by Staphyocaccus
aureus andor Streptocceus spp
‘Common presentations are bullous impetigo
(generally caused by staphylococcal disease)
and nonbulous impetigo (rom steptoeaceal
Infecon and possible staphylococcal infection)
‘the bullous form is caused by an epldermalytc
toxin produced atthe site of infection.
SYNONYMS,
Impetigo vulgaris
Pyoderma
Impetigo contagiosa
Bullous impetigo
|ep-t0cm copes
{01.00 Impetigo, unspecified
LoT.0t Nonbullous impetigo
L0T.02 Bockhart impetigo
1101.03. Bullous impetigo
L0T.08 other impetigo
EPIDEMIOLOGY &
DEMOGRAPHICS
+ Impetigo isthe mast commen bacterial skin
Infection in clr 2 to 5 yr of ago. Bullous
impetigo accounts for 30% of cases and non-
bullous for 70% of cases. Impetigo is most
common in temperate zones, mostly during
‘he summer hot, humid weather. Common
souroes for children are dirty fingers, pes,
and ater children in school of day care cen-
tes. Impetigo often complicates insect ites,
pediculoss, scabies, eczema, and poison iv,
Bullous impetigo is mast common in infants
and children. The nonbullous form is most
common in chitren ages 2 to 5 yr wih poor
hygiene in arm climates.
The overall incidence ot acute nephritis with
Impetigo varies between 2% and 5%.
PHYSICAL FINDINGS & CLINICAL
PRESENTATION
‘+ Nonbullous impetigo begins as a single ed
macule or papule that quicdy becomes 2
vesicle. Rupture ofthe vescle produces an
feosion of which te contents dry to form
honey-clored crusts. Muliple lesions with
golden yellow crusts (i. Ei) and weeping
areas are often found on the skin around the
nose, mouth and lms.
Bullous impetigo is manifested by the pres-
fence of vesicles that enlarge rapidly to form
bullae with contents that vary from clear to
cloudy, There is subsequent collapse of the
center ofthe bullae (F9. £2); the peipherl
areas may retain Mud, and a honey-colored
crust may appear in the center (9. £3). AS
the lesions enlarge and become contiguous
wath the otters, a scaling border replaces the
‘lidtiled rim: there Is minimal erythema
surrounding the lesions,
‘+ Regional ymphadenopatry is most common
with nonbullous impetigo,
+ Consttutional symptoms are generally
absent,
ETIoLocy
+ . aureus coagulase postive is the dominant
microorganism (50% to 70% of cases)
8. pyogenes (group A f-hemolytc strepto-
003) M-T serotypes of his organism asso-
ciated with acute nephritis are 2,48, 86,87
and 60. Group B streptococci are associated
with newborn Impetige,
(}ybiaGNosis
DIFFERENTIAL DIAGNOSIS.
+ Atopic dermatitis
«+ Horpes simplex infection
* Eethyma
+ Folicutis
+ Dermatitis herpetiformis
* Insoct bites
+ Scabies, pediulsis
* Tinea corporis, cutaneous candidiasis
+ Pemphigus vlgais and bullous pemphigoid
chickenpox
+ Thermal burns
* Contact dermatitis
+ Stevens-Jonnson syndrome, Sweet syndrome
WORKUP
Diagnosis is tinea
LABORATORY TESTS
Generaly not necessary
* Gram stain and culture and sensitiity to
confirm the diagnosis when th clinical pre-
sentation i unclear
+ Sedimentation rate oarall to activity of the
disease
FG. £1 Nonbuious (crusted) Impetigo. Eythemstous papules with honey yelon-colored crusting. From
Palle AS, Mancini Al: Hurt cncl paca dermatlegy a txtook of shi sores of chidhood and
adolescence, ed, 2016, Elsevier)
FIG. E2 Bullous impetigo. Thir-aled vesicles and shalow erosions wth periparlcallareltes and rit
crusting onthe butock and posterior thigh Fm Pal AS, Mani Al: Aart cnc! pela dermatigy,
{2 lertbook of sin ordre of ehidhocd and adoiescens, eS, 20°6, Fever)
Impetigo @
FIG ES Bullous impetige Mull tender, erythematous paches wit apersheral colaret, representing
remnant ofthe blister roo. rom Palle AS, Manca Al: Hurt clnical adie dermatology 2 textbook of
‘ski citorers of chldhond and adolescence, e 5, 2076, leet)
* Increased ant-DNAse 8 and anthyaluroni-
ace
+ Urinalysis reveating hematuria with erythro
cyte casts and proteinuria in pation: with
acute nephritis (most tfequenty occuring
in chlcren between ages 2 and 4 yr inthe
southern part ofthe US)
+H recutent staphylococcal impetigo devel-
ops. a culture of the anterior nares should be
one to rule outa carir state
a TREATMENT
NONPHARMACOLOGIC THERAPY
Remove crusts by soaking with wet coth com-
presses (crusts block the penetration of ant-
bacterial creams}
GENERAL Rx
+ Treatment consists of topical or oral antbot-
1s that are active against both S. aureus and
-hemodti steplocac
SUGGESTED READINGS
‘Agpcaton of 2% mugirocn ointment td or 10
days or reiapamalin 1% applied ba for 5 days 0
‘he tected are or unl allesons have deare,
Czenoracin is topical nonfuorinated qu-
nolone antibiotic recently FDA-approved for
‘teatment of impetigo In patients 2 mo old
Costs a limiting facto,
Oral antbiotes are used in severe cases:
‘Commonly used agents are cilorailin 250
1g aid fr 7 to 10 days, cephalexin 250 mg
{i for 7 to 10 days, azithromycin 500 mg on
day 1, 250 mg on days 2 trough 5, amoxii-
lnlevuanate 500 mg ah.
Impetigo can be prevented by prompt appl-
cation of muprain or tple-antbiaticoint-
ment foaitracin, Plyspoin, and neomycin)
‘sites of skin vauma
Patents who are carters of S. aureus in
‘ther nares should be treated with mupi-
focin ointment applied to theit nares bid
for § days or a 10-day course of rifampin,
6600 mg/day, combined with icloxacilin or
Banger Set a: Bacal resctance ané impaga werd: 2 review, Petr
Dermat 29;481~484, 2012
MarenanAdams ot ak Ingle: sagnsis and treatment, Am Fam Physician
90(:208-235, 2014
methiclin-sensitve Staphylococcus aure-
tus [MSSA}) or tvimethoprim-sulfametnox-
azole [TMP-SHX} (for methiclin-rsistnt
Staphylococcus aureus (MRSA),
‘+ Fingernals shouldbe kept short, and patents
should be advised not to scratch any lesions
to avoid spread of infection.
DISPOSITION
Most cases of impetigo resolve promptly with
appropriate treatment. Both bullous and nonbul-
lous forms of impetigo neal without scaring
REFERRAL,
Nephrology referral in patients with acute
nephritis
PEARLS &
CONSIDERATIONS
COMMENTS:
«+ Patients shouldbe instucted on use of ant-
bacterial soaps and avoidance of sharing of
towels and washeloths because impetigo
extremely contagious
Children attending “day care should be
removed until 48 to 72 hr ale inition of
antbatic treatment.
+ Bulous impetigo may be an early manieste-
tion of HV intecton
RELATED CONTENT
Impetigo Patent information)
-NOTHOR Fre, For, MD
782.03
feed Lichen Planus fd ©)
7D basic inronmarion
DEFINITION
Lichen planus (LP) refers to an idiopathic
inlammatory disease manifesting with a papu-
lar skin eruption characterscaly found over
‘the floxor surfaces ofthe extremities, genital,
and mucous membranes,
SYNONYMS,
LUchon
Lichen planus et alrophicus
iP
|ep-t0cm coves
43 Lichen planus
|L43.0 Hypertrophic lichen planus
443.1. Bullous lichen planus
L423 Lchen planus, unspecified
14338 Other Vehen planus
EPIDEMIOLOGY &
DEMOGRAPHICS
INCIDENCE: One in every 100 new patients
swen in dermatology cline in the United States
Is diagnosed with LP
PREVALENCE: 440 cases/100,000 persons
PREDOMINANT SEX: Found equally between
male and feales (1)
PREDOMINANT AGE: Usually found in people
between the ages of 80 and 60 yr
PREDISPOSING FACTORS:
+ Associated with other autoimmune disorders
(e.9., prmary biliary cithosis, myasthenia
(avs, ulcerative colts, diabetes)
+ Associated with hepatitis C infection
+ Drug-induced form affects any area of the
body surface (e.g. beta-blocker, methyl
dopa, penicilamine, quinidine, nonstero-
al antinflammatory drugs, angiotensin-
comerting enzyme inhibitors, sulfonylurea
agents)
PHYSICAL FINDINGS & CLINICAL
PRESENTATION
Lichen planus often manifests wth prur, t-
‘opped violaceous papules but tre clrical pre-
sentation varies depending onthe aea involve,
History
Usually stats on an extremity and may
remain localized or spread to involve otter
areas over a 1 to 4-mo period
++ Puutie
Physical findings
Anatomie distrbuton:
1, Flexor surface of wrists, forearms, shins,
and upper thighs
Neck and back area
Nalls (6% to 10% of patients)
Scalp (lichen planoplrs)
Oral mucosa, buccal mucosa, tongue,
gingiva, and lps; orl lichen planus can
cause extensive desquamatve gngvits
6, Vulva (Fig. £1), penis Fg. £2)
Genital mucosa:
Lesion configuraton:
1 Unear
2. Annular (more common)
8. Reticular pattern noted on oral mucosa
and genital area
+ Lesion morphology
1, Papules most common presentation (Yat,
smooth, shiny (ig 3)
2. Hypertrophic
3. Follculer
4, Vesicular
+ Color
1. Dark 10d, bluish red, purplsh-vlacoous
colors noted in cutaneous LP (Fig. E
2 Individual lesions enaracteritcaly have
white lines visible (Wicknam striae) (Fig.
3)
3. Oral and genital LP has a reticular net-
work of white lines that may be raised or
annular in appearance (ig. £8)
* Scalp lesions may result in alopecia,
+ The plaques of chen planus may be hyper-
‘eophic but show the charactrstic viol
.20us coloration an intense hyperpigmenta-
ton (Fo. £7.
ETIOLOGY
LUchen planus is characterized by an immu-
ologic reaction mediated by CBs T calls
These eels induce keratinocytes to undergo
apoptosis. though the inflammatory reaction
is believed to be autoimmune, the antigen
targeted by these effector T Iymphocytes is
unknown,
FIG E1 Lichen planus ofthe vulva with a whit, lacelike pattern and erythema. (om Crum C? eta
Diagnastic gmecalogc and obstetric pattology,e 3, Philadelphia, 2018, sever)
FIG. E2 Lichen planus of the penis. rom Swartz MH: Textbook o pyc! agnosis hstory and eraina-
tin 07, Peli, 2014, Saunders)
Lichen Planus @®
FIG, E3 Flattopped, purple, polygonal papules of lichen planus. (Fon Morell JG: Diseases ofthe
‘dermis, in Kogan RM oa os Nolan tevibok of peda, ed "8, Philadel, 2011, Saunders)
FG, E4 Shiny, flttopped, polygonal, violaceous papules of lichen planus. Hote the Wickham
striae linear, whitish-gray streaks) on the surface. ron Pale AS, Mancini A Hurwitz cn pediatric
dermatology, textbook of skin dsrdesof childhood and adlescence of 5, 2016, sev}
+ Clinica history and physical findings usually
establish the diagnosis of LP.
+ Skin biopsy (deep shave or punch biopsy of
‘he most developed lesion) can be performed
to confirm the diagnosis
DIFFERENTIAL DIAGNOSIS:
+ Drug eruption. psoriasis, Bowen disease,
loukoplaka, canditiasis, lupus rash, second
‘ay sypilis, sebortelc dermattis, chronic
graftversus-host disease
‘+ Teble El summarizes variants of lichen
planus
WORKUP
Iv the agnosis is questionable, askin biopsy
's performed
LABORATORY TESTS
Laboratory tests are not speci forthe dagno-
‘is of LP. Lipid panels screening is useful since
increases in serum triglycerides and decreases
in HDL cholesterol are common in patients
with LP
IMAGING STUDIES
Imaging studies are not helpful in dlagnosing
it
NONPHARMACOLOGIC THERAPY
“+ Avoid seratohing.
+ Use mild soaps and emolients ater bathing
‘to proventcryness
GENERAL Rx
FOR CUTANEOUS LP:
> Topical steroids (29. ameinoione aceton-
ide 0.1%, fluocinonide 0.05%, cobetasol
propionate 0.05% cream or ointment) with
‘occlusion used twice daly
‘Acietin 30 ma/day PO for 8 wk
+ Systemic prednisone 30 to 60 ma/day as a
starting dose and tapered to 15 to 20 mg/
day maintenance for 6 wk can be used for
widespread lesions
‘+ Inradermal sto tiamcinolone acatoide
5 mg/ml can be ted for thick hyperkeratoc
lesions
+ Hydraxyzine 25 mg PO a6h can be used for
prurtus|
+ Phototherapy: PUA or narrow-band ultavio-
Iet B therapy: 2 of 3 times per wr, for a total
of 12 sessions (., one cyte)
FOR ORAL LP:
* Topical steroid uocinonide in an adhesive
base used six tmes/day for 9 wk
‘Topical calcineurin in sterold-uwesponsve
cases
+ Topical or systemic retinoids 0.1% retinoic
‘acid in an adhesive base or ge
+ Etretinate 75 mglday for 2 mo
DISPOSITION
* Spontaneous remissions of cutaneous LP
‘ur in >65% of cases within the fst year.
+ Spontaneous remission of oral LP usually
‘ocurs by 5 yr.
+ Approximately 10% fo 20% of patients wi
hhave recurrence.
REFERRAL
To dermatologist agnosis is unclear
COMMENTS:
+ LP can be remembered as purple, planar
prutc, plygona, papules, and plaques (sie
Ps,
+ Lesions can develop at the site of pio skin
inury(Keebner phenomenon).
+ AMthough there Is an increased risk of squa-
mous call carcinoma in chronic lesions of
mucosal L, ransformation to skin cancer is
RELATED CONTENT
LUchen Planus Patient information)
-NSTHOR Fred Fer, MD
Lichen Planus @ 83304
FIG. E5 A 2nd B,Lihon planus. Note te ne, eculted whit sales. Swartz NM: Textbook of physical
iagnass, history and examination, ed 7, Phadelpra, 2014, Saunders)
FIG, E6 Oral lichen planus. Wickham sie onthe buccal mucoss, (rom Palar AS, Mancini Alt Horta
clic pediatc dermatology,» textbook o skin dsrdereo chighend and agoescece ed 6, 2016, ever)
Lichen Planus @®
FIG, E7 Lichen planus. The plaques of licen planus may be hypertepic but stow the etaactersic
Vilacous coloration and intense hyperpigmentation (From Pals AS, Marcin Ai: Aural clinca pedi
‘dermatology. textbook o skin aeordersof childhood and adolescence 8, 2018, Ekevier)
TABLE E1 Variants of Lichen Planus
Variant Type
Characteristics
‘Bulan develo on estan LP lesions
atous
> pamphigeies
satne
‘route
Pyperphi
Arphic
emormapetou-
ure
Un
Erosveleerave
etapa ees
tonue
Lehn planar
UP bulou pemphigoid wit aucune react, sua agaist type cae
lagen ulus pemprignd 180 antigen)
nse cui sping, sume, primey sun-exposed surace Pace, neck. desu of
‘rms and hard} fen anrlar canfguratin most common inciéen an young
ute
(Occur n 10% of patents, een sare ami yl esos ot LP
‘Thick, pruntic, hyperkeratate plagues, expec onthe lege and dorsal repos of he
feet pesson
May represents resoing hase n whic large plaques become cantly depressed
vith esl perpimentaton
‘Shows nonlaching eamponent on scopy
LP owen spontanacsly ang tenes of Bsc, presumably reflect somatic
resaicem
Intensely painful uceaton on he pls and sce; chronic lesan ray avo into
squamous celcarcnoms; eave lslons may ozur on mucosal suraces
Overiopng features of lupus and LP. sions ae sully acral and patents may
show high ters of ANA
Foliclar LP; keratote pigs surouned by vlaceos ertrena, especialy on scab
but can fect ny hai-bearing ars; usally ests in leat alopecia
‘rc rode: een Hs,
From Pale, Maze A Maciel pate mao txook of shins f cheat and aero
ote deen
SUGGESTED READINGS
‘as Sontag So a Crsvazculr rik factors in patti Hen planus,
‘nS od 124543-548, 2011,
Le Cleat, Choséw 0: Lichen planus, M Engl J Med 36:729-72, 2012
Fry Lichen Sclerosus 10 ©)
7D pasic inronmarion
DEFINITION
Lichen sclerosus (LS) isa chronic intammatory
condition ofthe skin usually affecting the vulva,
pens, perianal area, and ron.
SYNONYMS,
Lichen scerosus et atrophicus
kKraurosis vulae
Balai erotica obterans
Is
|eD-10cm cove
190.0 Lichen sclerosus et atophicus
EPIDEMIOLOGY &
DEMOGRAPHICS
Most common in postmenopausal women
and men between ages 40 and 60 yr.
More comman in females (female:male ratio
of $:1). affects 1.7% ofthe general adult
female population
‘Can occur in chidren (usually prepubertal
itis with involement of the vulva. and
perineum),
PHYSICAL FINDINGS & CLINICAL
PRESENTATION
Exythema may be the only inal sign. A
characteriste fnding is the presence of
Inoryetite atrophic lesions onthe involved
Close inspection of the affected area wil
reveal the presence of whit-to-brown fol
cular plugs on the surface (ls),
When the genitals are involved, the white
parchmeni-ke skin assumes an hourglass
Coriguraton around the inital and per-
anal area (*keyhole” cistibuion; Fig. El
Fig. £2) Inflammation, supithalial hemor
ages, and chronic ulceration may develop.
In males, lesions are atophic and may be
hypopigmentedordepigmented,esembingvit-
igo. Phimoss and paraphimoss are common
‘complictons in uncrcumesed males wih LS.
Lesions may be surrounded by an erythoma-
tous to violaceous halo,
Dyspareunia, genital bleeding, and anal
bleeding ae common,
Prutus may be a prominent symptom
ETIoLoay
Unknown, Tere may be an autoimmune asso-
lation and a genetic fala! component
(}ybiaenosts
DIFFERENTIAL DIAGNOSIS.
Localized seerederma (morphea)
Cutaneous discoid ypus erythematosus
‘trophic lichen planus
Psorias's
Lichen simplex eronieus
Vulvar intraepithelial neoplasm
Extramammary Paget disease
‘Table E1 summarizes the ditferentil dag
rosis of common vulvar mucocutaneous
dlsordors
WORKUP
Diagnosis is based on close examination ofthe
lesions forthe presonce of Wory-white atrophic
lesions and typical locaton
LABORATORY TESTS
“+ Punch or deep shave biopsy can be used to
confirm te dlagnosis,
+ Autoantibodies to extracellular mate protein
1 (ECW-1) are present in 8% of LS patents
and the ECM-1 tier coralates with disease
acti
g ‘TREATMENT
NONPHARMACOLOGIC THERAPY
* Aitention to hygione and elimination of i
tants o excessive bathing with harsh soaps.
‘Cryotherapy and photodynamic therapy can
be used in retractoy cases.
GENERAL Rx
+ Applicaton of cobetasel propionate 0.05%
topically bia for up to 4 wk is usualy eter:
tive, Repeat courses of corticosteroids may
be necessary because ofthe cronic nature
of this disorder, Continual application of top
cal steroids may lead to atrophy ofthe vula
‘There is no substantial evidence that use
of topical sex hormones (e.g. topical tes-
tostorane 23) Is effective In gonial lichen
solerosus,
+ Lubricants (eg, Nutraplus cream) are useful
to soothe dry tissues
+ Hydroxyzine 25 ma at bedtime is etective in
ecreasing nocturnal itching
+ Use of intalesional steroids, ebetinate, and
sutgieal management is usualy reserved for
refractory cases.
DISPOSITION
+ The disease persists in approximately one
third of patients
+ Most prepubertal girls improve spontane-
ously at menarche,
+ Squamous cell carcinoma can dvelop within
the lesions in 3% to 10% of older patients
therefore periodic examination and biopsy of
suspicious areas are indicated.
PEARLS &
CONSIDERATIONS
COMMENTS
+ Prepubetal lichen sclerosus may be con-
fused with sexual abuse in prepubertal
gis and may lead to false accusations and
rvestigations.
+ Pregnancy leads to improvement and often
‘complete resolution of lesions, suggesting 2
hormonal component to etiology of lesions.
FAG, £1 Lichen selerosus with stenosis ofthe itrelts,fesuring In the posterior fourchette, and
erianalinvelvement producing the "key
jes" sha BK and Magesson Li: Genital skin
sores: agnosis an restment n Disa P et al Cinel gmecolgi oncology ed 8 Phisdphi. 2017,
Elser)
Lichen Sclerosus 833.07
Lichen sclerosus of the wv (raurosis
wulvae) usually occurs ater menopause and
is generaly chronic. It can be painful and
interfere with sexual activity,
* Lichen sclerosus ofthe penis (balanits xerot-
ica obliterans) is seen more commonly in
Uuncircumesed males. tt affects the glans
and prepuce and may lead to sicture if it
‘enroaches into the urinary meatus.
RELATED CONTENT
Lichen Selerosus Patient Information)
-NOTHOR: Fred For, MO
FIG EZ A, lsicalapoewance at lchen slrous, Note the stop ofthe fblum mins. , Lichen slerosus
wih prominent nourglassappenrance, om Cram OP et a: Dagnoste gynecologic and obsttcpaheegy,
3, Pladephia. 2018, Eker)
‘TABLE E1_Differental Diagnosis of Common Vulvar Mucocutaneous Disorders
Diagnosis Aen PK Spong HK LL IDEM Selva top TTR Exchde
Len simgex + = + = Cane
evoncus 80)
Leben semrsus soe * 2 ann
as)
Eszema * + * Sobol dermatitis
Lichen planes * * + Ey Ls
Lsc+is + + + an
szema + LSC + + ana
en : + * Sypits
Proasis + + 80, Candida
‘ea eas Ae apy a tee avr wpe shai: Wp Flere Gems EX, nny Zep Leh wa PX peor
os Sng apne TT tube maya preset
From Gum Gata Dap sracco and bre pay 08, Pea 2018. bev,
‘SUGGESTED READING
(fC eta Topica interventions for geal chen sclerosis, Coohrane Database
‘jst Rer 200008240, 2011,
9 basic inronmarion
DEFINITION
Psoriasis is a chronic skin disorer charactr-
zed by excessive proleration of keratinocytes,
resulting in the formation of thickened scaly
plaques, itching, and intammatory changes
of the epidermis and dermis. Psoriasis is also
associated with cardovascular, metabo, and
neuropsychiatric effects. The various forms
of psoriasis include plaque (most common),
guttate,eryirodermic, pustular, inverse, and
arts variants
1eD-t0cm coves
Lao. Proriasis
40.0. Psoriasis vulgaris
40.1. Generalized pustular psoriasis,
40.4 Guta psoriasis
L40.8 Other psorass
40. Psoriasis unspected
[40.54 Psoriatic juvenile arthropathy
EPIDEMIOLOGY &
DEMOGRAPHICS
* Peorisis affects 2% to 4% of the world’s
population. Most patients have limited pso-
isis involving
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Irfan Masood PedsDocument160 pagesIrfan Masood PedsUsman AR VainceNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- H.pylori TreatmentDocument3 pagesH.pylori TreatmentUsman AR VainceNo ratings yet
- Medical Globe Guideline 1Document42 pagesMedical Globe Guideline 1Usman AR VainceNo ratings yet
- High Performance Liquid ChromatographyDocument8 pagesHigh Performance Liquid ChromatographyUsman AR VainceNo ratings yet
- Medicine Dosages 210606 223605Document39 pagesMedicine Dosages 210606 223605Usman AR VainceNo ratings yet
- General Medicine Diagnostic PointsDocument14 pagesGeneral Medicine Diagnostic PointsUsman AR VainceNo ratings yet
- 132 - Neurology Pathology - Stroke Syndromes - MCA, ACA, ICA, PCA, Vertebrobasilar Artery SDocument4 pages132 - Neurology Pathology - Stroke Syndromes - MCA, ACA, ICA, PCA, Vertebrobasilar Artery SUsman AR VainceNo ratings yet
- EFY CORRECTIONS - Take 1.0Document7 pagesEFY CORRECTIONS - Take 1.0Usman AR VainceNo ratings yet
- FCPS1)Document36 pagesFCPS1)Usman AR VainceNo ratings yet
- Vulvovaginal CandidiasisDocument5 pagesVulvovaginal CandidiasisUsman AR VainceNo ratings yet
- HemorrhoidsDocument43 pagesHemorrhoidsUsman AR VainceNo ratings yet
- Bashhcandidiasis 35685Document1 pageBashhcandidiasis 35685Usman AR VainceNo ratings yet
- FibroidsDocument10 pagesFibroidsUsman AR VainceNo ratings yet
- AIDSDocument12 pagesAIDSUsman AR VainceNo ratings yet
- Acute Burn ManagementDocument23 pagesAcute Burn ManagementUsman AR VainceNo ratings yet
- CardiacDocument10 pagesCardiacUsman AR VainceNo ratings yet
- Janssen 2012Document6 pagesJanssen 2012Usman AR VainceNo ratings yet
- 10.7556 Jaoa.2005.105.8.369Document11 pages10.7556 Jaoa.2005.105.8.369Usman AR VainceNo ratings yet
- Types of Sutures PDFDocument4 pagesTypes of Sutures PDFUsman AR VainceNo ratings yet
- PpillDocument2 pagesPpillUsman AR VainceNo ratings yet