You might also like
- Roleof Diabetesin ProsthodonticsDocument4 pagesRoleof Diabetesin ProsthodonticsHemiya ThomasNo ratings yet
- Oral Leukoplakia.Document5 pagesOral Leukoplakia.RA Risa EffendiNo ratings yet
- Letter MamburaoDocument1 pageLetter MamburaoZyreen Kate BC75% (4)
- NCLEX Practice QuestionsDocument4 pagesNCLEX Practice QuestionsbrandycarlsonNo ratings yet
- Dental Caries A Microbiological Approach 2476 213X 1000118Document16 pagesDental Caries A Microbiological Approach 2476 213X 1000118NOVITANo ratings yet
- JBM - Effect of MalocclusionDocument10 pagesJBM - Effect of MalocclusionAma AmuasiNo ratings yet
- Hiv/Aids: January 2021Document70 pagesHiv/Aids: January 2021Chaerunnisa Supriani SaputriNo ratings yet
- Oral LichenoidDocument12 pagesOral LichenoiddjianNo ratings yet
- International Seminar On Oral Leukoplakia and Associated Lesions Related To Tobaceo HabitsDocument11 pagesInternational Seminar On Oral Leukoplakia and Associated Lesions Related To Tobaceo HabitsSiti Fatimah Khaerun NisaNo ratings yet
- 7 DB 6Document6 pages7 DB 6AamirNo ratings yet
- Khusbuandsatyam Dentalcaries ReviewDocument8 pagesKhusbuandsatyam Dentalcaries ReviewLoredana BarbaneagraNo ratings yet
- Sjogrens Syndrome AReviewDocument6 pagesSjogrens Syndrome AReviewAndani KurniaNo ratings yet
- JHeadNeckPhysiciansSurg4129-194289 052348Document6 pagesJHeadNeckPhysiciansSurg4129-194289 052348Javeria MNo ratings yet
- Role of Taste Perception in WSL Formation During Orthodontic TreatmentDocument6 pagesRole of Taste Perception in WSL Formation During Orthodontic TreatmentShreya JohnNo ratings yet
- DeVisschere-Gerodontology-2011 An Oral Helath Care Guideline For Institutionalised Older PeopleDocument5 pagesDeVisschere-Gerodontology-2011 An Oral Helath Care Guideline For Institutionalised Older PeopleAlejandro Perdomo RubioNo ratings yet
- An Oral Health Care Guideline For Institutionalised Older PeopleDocument5 pagesAn Oral Health Care Guideline For Institutionalised Older PeopleAvina Anin NasiaNo ratings yet
- 9800 9800 WJCC-2-866Document8 pages9800 9800 WJCC-2-866An Nisaa DejandNo ratings yet
- JIntOralHealth 2021 13 5 441 3278672Document10 pagesJIntOralHealth 2021 13 5 441 3278672IgnasNo ratings yet
- Proliferative Verrucous Leukoplakia: An Update: Review ArticleDocument5 pagesProliferative Verrucous Leukoplakia: An Update: Review Articlepoi09No ratings yet
- Precancerous Lesions of Oral MucosaDocument9 pagesPrecancerous Lesions of Oral MucosaregysujitNo ratings yet
- 1 s2.0 S0300571216302202 MainDocument6 pages1 s2.0 S0300571216302202 MainRaluca ChisciucNo ratings yet
- Antibióticos y EndodonciaDocument8 pagesAntibióticos y EndodonciaPaola AndreaNo ratings yet
- (23350245 - Balkan Journal of Dental Medicine) Salivary Theranostics in Pediatric and Special Care Dentistry PDFDocument8 pages(23350245 - Balkan Journal of Dental Medicine) Salivary Theranostics in Pediatric and Special Care Dentistry PDFTushNo ratings yet
- Khus Bu and Satyam Dental Caries ReviewDocument8 pagesKhus Bu and Satyam Dental Caries Reviewmeena syedNo ratings yet
- S Jog Rens Syndrome Are ViewDocument6 pagesS Jog Rens Syndrome Are ViewOcha24 TupamahuNo ratings yet
- Assessment of Oral Health-Related Quality of Life Among Head-And-Neck Cancer Patients Attending Cancer Care Center at Kanchipuram, Tamil Nadu  A Cross-Sectional StudyDocument7 pagesAssessment of Oral Health-Related Quality of Life Among Head-And-Neck Cancer Patients Attending Cancer Care Center at Kanchipuram, Tamil Nadu  A Cross-Sectional StudyFelix SchweppeNo ratings yet
- Journal Reading 1Document16 pagesJournal Reading 1Rizky Amalia SaputriNo ratings yet
- Oral Health Related Quality of Life: March 2013Document8 pagesOral Health Related Quality of Life: March 2013imadsssNo ratings yet
- Novel Strategies For The Bioavailability Augmentation and Efficacy Improvement of Natural Products in Oral Cancer PDFDocument30 pagesNovel Strategies For The Bioavailability Augmentation and Efficacy Improvement of Natural Products in Oral Cancer PDFNourhan AbdalkaderNo ratings yet
- Epithelial DysplasiaDocument9 pagesEpithelial DysplasiaS HNo ratings yet
- The Sixth Edition WHOManualfor Human Semen AnalysisDocument14 pagesThe Sixth Edition WHOManualfor Human Semen AnalysisMEDIWAY CLINICNo ratings yet
- Public Health Dentist As An "Environmental Scientist" - An Unexplored AreaDocument3 pagesPublic Health Dentist As An "Environmental Scientist" - An Unexplored AreaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Review Articles: Management of Oral Leukoplakia: A ReviewDocument8 pagesReview Articles: Management of Oral Leukoplakia: A ReviewKarma YogaNo ratings yet
- SaudiJOralSci313-2968904 081449Document9 pagesSaudiJOralSci313-2968904 081449EnochDomprehNo ratings yet
- JOralMaxillofacPathol23119-9376184 023616Document9 pagesJOralMaxillofacPathol23119-9376184 023616porkodi sudhaNo ratings yet
- Saliva ApromisingdiagnostictoolDocument3 pagesSaliva ApromisingdiagnostictoolTitodcNo ratings yet
- Medoral 25 E106Document11 pagesMedoral 25 E106Piercy EvaNo ratings yet
- Oral Cancer Literature ReviewDocument5 pagesOral Cancer Literature Reviewjsmyxkvkg100% (1)
- 23.balsaraf Et - Al.pubDocument6 pages23.balsaraf Et - Al.pubKamado NezukoNo ratings yet
- Pone 0145837Document16 pagesPone 0145837Raluca ChisciucNo ratings yet
- Expert Consensus On Irrigation and Intracanal Medication in Root Canal TherapyDocument10 pagesExpert Consensus On Irrigation and Intracanal Medication in Root Canal Therapydocbsg21No ratings yet
- Leucoplasia DiagnosticoDocument2 pagesLeucoplasia DiagnosticoFrancisco VargasNo ratings yet
- EJMCM Volume 7 Issue 8 Pages 1659-1663Document5 pagesEJMCM Volume 7 Issue 8 Pages 1659-1663andifarra281002No ratings yet
- SaudiJOralSci83143-5397926 145939Document8 pagesSaudiJOralSci83143-5397926 145939soniNo ratings yet
- APACT 2021 MetadataDocument126 pagesAPACT 2021 MetadataJohn HudsonNo ratings yet
- Occupational Hazards in Dentistry: January 2017Document14 pagesOccupational Hazards in Dentistry: January 2017Mustafa AmmarNo ratings yet
- Acad Dermatol Venereol - 2019 - ChernyshovDocument11 pagesAcad Dermatol Venereol - 2019 - ChernyshovRizki irsyad MaulanaNo ratings yet
- Dr. Junaid Faisal WazirDocument10 pagesDr. Junaid Faisal Waziryasir iqbalNo ratings yet
- Idh 12304Document10 pagesIdh 12304Hiba HamidNo ratings yet
- Effect of Ageing On Oral Health-Related Quality of Life: Review ArticleDocument3 pagesEffect of Ageing On Oral Health-Related Quality of Life: Review ArticlejoephinNo ratings yet
- GeriatriaDocument6 pagesGeriatriaGoku BlackNo ratings yet
- Association of Microbiome With Oral Squamous CellDocument21 pagesAssociation of Microbiome With Oral Squamous CellGhimpu DanielaNo ratings yet
- Hyaluronic Acid: A New Approach For The Treatment of Gingival Recession-A Systematic ReviewDocument11 pagesHyaluronic Acid: A New Approach For The Treatment of Gingival Recession-A Systematic ReviewGali Alfaro ZagalNo ratings yet
- 2 AdultExpertsurveyJdentDocument13 pages2 AdultExpertsurveyJdentpepeNo ratings yet
- Dental HealthDocument3 pagesDental HealthTerem TebaNo ratings yet
- Oral Potentially Malignant Disorders A Consensus Report From An International Seminar On Nomenclature and Classification, ConvenDocument19 pagesOral Potentially Malignant Disorders A Consensus Report From An International Seminar On Nomenclature and Classification, ConvenSophia RochaNo ratings yet
- Oral Oncology: Jingyi Liu, Yixiang DuanDocument9 pagesOral Oncology: Jingyi Liu, Yixiang DuanSabiran GibranNo ratings yet
- Triphala Vs Chx-ArticleDocument7 pagesTriphala Vs Chx-ArticleDebjyoti DebnathNo ratings yet
- Oral CareDocument8 pagesOral Caredwiwahyu ningsihNo ratings yet
- Development and Validation of The Oral Mucositis Risk Assessment Scale in Hematology PatientsDocument6 pagesDevelopment and Validation of The Oral Mucositis Risk Assessment Scale in Hematology PatientsPaola GilNo ratings yet
- 2021 Margaritis - DEVELOPDocument12 pages2021 Margaritis - DEVELOPfabian.balazs.93No ratings yet
- Atlas of Inflammatory Bowel DiseasesFrom EverandAtlas of Inflammatory Bowel DiseasesWon Ho KimNo ratings yet
- Madohc Ms Id 000124Document4 pagesMadohc Ms Id 000124eris nurulNo ratings yet
- Systematic Review and Meta-Analysis in Oral Medicine-An UpdateDocument5 pagesSystematic Review and Meta-Analysis in Oral Medicine-An Updateeris nurulNo ratings yet
- Balakumar 2015Document34 pagesBalakumar 2015eris nurulNo ratings yet
- Cardiovascular Disease and Periodontal Disease - Nguyen2018Document6 pagesCardiovascular Disease and Periodontal Disease - Nguyen2018eris nurulNo ratings yet
- Courses InfoDocument3 pagesCourses InfoHAJARATHNo ratings yet
- Gestational HTNDocument6 pagesGestational HTNSim DimalantaNo ratings yet
- Case StudyDocument26 pagesCase Studyamazing grace mejia carlos100% (2)
- Selina Concise Biology Solutions Class 9 Chapter 16 Diseases Cause and ControlDocument3 pagesSelina Concise Biology Solutions Class 9 Chapter 16 Diseases Cause and ControlSiri ChandanaNo ratings yet
- EphysemaDocument4 pagesEphysemaHanaNo ratings yet
- EmilyresumemphDocument2 pagesEmilyresumemphapi-375369324No ratings yet
- Literature Worksheet Revision - Grade VIIDocument2 pagesLiterature Worksheet Revision - Grade VIIVedansh DixitNo ratings yet
- GALZOTE PaperCase1-SurgeryDocument4 pagesGALZOTE PaperCase1-SurgeryRock GalzoteNo ratings yet
- 4.review of LiteratureDocument16 pages4.review of LiteratureMAHESH KOUJALAGINo ratings yet
- Methodology Series Module 1 Cohort StudiesDocument5 pagesMethodology Series Module 1 Cohort StudiesRaa ShaviraaNo ratings yet
- Hypopyon UveitisDocument18 pagesHypopyon UveitisjochigNo ratings yet
- Contact Dermatitis Fact SheetsDocument1 pageContact Dermatitis Fact SheetsJoe Aire SalvediaNo ratings yet
- Pediatric Soft Tissue Lesions: Andres Pinto, DMDDocument18 pagesPediatric Soft Tissue Lesions: Andres Pinto, DMDHanin AbukhiaraNo ratings yet
- Rakhmat A.H - Current Concept Polytrauma Approach FINAL REVDocument22 pagesRakhmat A.H - Current Concept Polytrauma Approach FINAL REVTezarNo ratings yet
- Disseminated Intravascular Coagulation in PregnancyDocument8 pagesDisseminated Intravascular Coagulation in Pregnancydr_asaleh100% (1)
- WIL - English Does Work 7 Cronica WRITINGDocument2 pagesWIL - English Does Work 7 Cronica WRITINGwilbert edill rodriguez martinez50% (2)
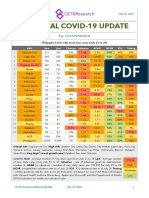
- National COVID-19 Update by Octa Research On July 30, 2021Document2 pagesNational COVID-19 Update by Octa Research On July 30, 2021RapplerNo ratings yet
- Jurnal Reading: Sit Dolor AmetDocument20 pagesJurnal Reading: Sit Dolor AmetLiri AndiyaniNo ratings yet
- Job Descriptionof ICNDocument5 pagesJob Descriptionof ICNsari sasiNo ratings yet
- Soccer InjuriesDocument19 pagesSoccer InjuriesEmannuel GomesNo ratings yet
- Throats Cancer TreatmentDocument4 pagesThroats Cancer Treatmentmuadzzulkar9No ratings yet
- Vermont School Immunization Exemption Form2.8Document1 pageVermont School Immunization Exemption Form2.8DonnaNo ratings yet
- CASE ANALYSIS - Arcasitas. Kenneth IDocument2 pagesCASE ANALYSIS - Arcasitas. Kenneth IKenneth Arcasitas100% (1)
- Update From St. Louis County Department of Public HealthDocument14 pagesUpdate From St. Louis County Department of Public HealthKayla GaffneyNo ratings yet
- LESSON PLAN On EpdemionlogyDocument6 pagesLESSON PLAN On EpdemionlogyAshish GuptaNo ratings yet
- CDI Consumer Factsheet BrochureDocument2 pagesCDI Consumer Factsheet BrochurebejarhasanNo ratings yet
- SMARTCHEK Novel Coronovirus (SARS-CoV-2) Detection KitDocument2 pagesSMARTCHEK Novel Coronovirus (SARS-CoV-2) Detection KitJHORDY ADISONSCOT ARMAS AMATNo ratings yet
- Health Psychology An Introduction To Behavior and Health 8th Edition Brannon Test BankDocument26 pagesHealth Psychology An Introduction To Behavior and Health 8th Edition Brannon Test BankJosephMartinezwgrin100% (10)