You might also like
- Mind Power SecretsDocument38 pagesMind Power SecretsIan Faian92% (52)
- Mcqs of Family LawDocument24 pagesMcqs of Family LawVenugopal Mantraratnam32% (19)
- Form Ibpr Haul Road PDFDocument2 pagesForm Ibpr Haul Road PDFelvandi100% (1)
- DCM601A51 - Technical DataDocument405 pagesDCM601A51 - Technical Datathanhthuan100% (1)
- TDI - Full Cave Diver Course: TDI Instructor Manual Part 2 - Diver Standards Date: 12/31/2009 Revision: 10.0Document5 pagesTDI - Full Cave Diver Course: TDI Instructor Manual Part 2 - Diver Standards Date: 12/31/2009 Revision: 10.0BraulioNo ratings yet
- 6 DLL HOPE 3 2019-2020 JulyDocument2 pages6 DLL HOPE 3 2019-2020 JulyCelia BautistaNo ratings yet
- Community-Based Forest ManagementDocument7 pagesCommunity-Based Forest ManagementZiazel ThereseNo ratings yet
- Applications in High Resolution Mass Spectrometry: Food Safety and Pesticide Residue AnalysisFrom EverandApplications in High Resolution Mass Spectrometry: Food Safety and Pesticide Residue AnalysisRoberto Romero-GonzálezNo ratings yet
- Artigo 1Document18 pagesArtigo 1Ricardo PáscoaNo ratings yet
- Artigo 2Document17 pagesArtigo 2Ricardo PáscoaNo ratings yet
- Artigo 3Document16 pagesArtigo 3Ricardo PáscoaNo ratings yet
- Emile 2017Document11 pagesEmile 2017eleni kanelNo ratings yet
- Selection of Efficient Wavelengths in NIR Spectrum For Determination of Dry Matter in Kiwi FruitDocument12 pagesSelection of Efficient Wavelengths in NIR Spectrum For Determination of Dry Matter in Kiwi Fruitkby36No ratings yet
- YOUNG e ODUKODocument13 pagesYOUNG e ODUKOStella MainothNo ratings yet
- Materials and Methods: Globosa in Lesional Skin Was Only 6.3% (22) - The DifferencesDocument19 pagesMaterials and Methods: Globosa in Lesional Skin Was Only 6.3% (22) - The DifferencesalexNo ratings yet
- MCR AlsDocument10 pagesMCR AlsAndrés F. CáceresNo ratings yet
- Effect of CT Modality on Pediatric Radiation Doses and Image QualityDocument9 pagesEffect of CT Modality on Pediatric Radiation Doses and Image QualitySoma SweetNo ratings yet
- Apendicitis AgudaDocument17 pagesApendicitis Agudalbritez7No ratings yet
- Deploying Swarm Intelligence in Medical Imaging Identifying Metastasis, Micro-Calcifications and Brain Image SegmentationDocument11 pagesDeploying Swarm Intelligence in Medical Imaging Identifying Metastasis, Micro-Calcifications and Brain Image SegmentationSurbhi AnandNo ratings yet
- Comparison of Retropubic, Laparoscopic and Robotic Radical ProstatectomyDocument13 pagesComparison of Retropubic, Laparoscopic and Robotic Radical ProstatectomyOrlando SotoNo ratings yet
- Author's Accepted Manuscript: TalantaDocument44 pagesAuthor's Accepted Manuscript: Talantaida ratna nilaNo ratings yet
- Quantitative Analysis of Patient Specific Dosimetric IMRT VerificationDocument18 pagesQuantitative Analysis of Patient Specific Dosimetric IMRT VerificationMuhammad IrsyadNo ratings yet
- 13 PDFDocument10 pages13 PDFgitapusNo ratings yet
- Coronary Angiography and PTCA Skin Dose Evaluation Using Gafchromic FilmsDocument9 pagesCoronary Angiography and PTCA Skin Dose Evaluation Using Gafchromic FilmsAnne MbrkNo ratings yet
- The Framework Involving Scleractinian Coral Skeletal System Reviewed Simply by Neutron Diffraction and Also Neutron Computed Tomographylgqsa PDFDocument1 pageThe Framework Involving Scleractinian Coral Skeletal System Reviewed Simply by Neutron Diffraction and Also Neutron Computed Tomographylgqsa PDFcordfuel2No ratings yet
- P H Artes, Published Papers 1999-2013Document304 pagesP H Artes, Published Papers 1999-2013Paul H ArtesNo ratings yet
- Effect of Working Length Measurement by Electronic Apex Locator or Radiography On The Adequacy of Final Working Length A Randomized Clinical TrialDocument4 pagesEffect of Working Length Measurement by Electronic Apex Locator or Radiography On The Adequacy of Final Working Length A Randomized Clinical TrialDaniel Martínez VásquezNo ratings yet
- Ijarcce 47Document7 pagesIjarcce 47talha42103No ratings yet
- DTH 14650Document19 pagesDTH 14650Evelyn LimNo ratings yet
- Draft4 Researchproject Group8Document18 pagesDraft4 Researchproject Group8api-633248237No ratings yet
- Impact of MLC Leaf Width On Volumetric-Modulated ADocument13 pagesImpact of MLC Leaf Width On Volumetric-Modulated ANandha KumarNo ratings yet
- Villegas2012 PDFDocument5 pagesVillegas2012 PDFDiego Antonio Rodriguez CoronadoNo ratings yet
- Biomolecules 10 01123 v2Document13 pagesBiomolecules 10 01123 v2Adru von MatterhornNo ratings yet
- 163 FullDocument3 pages163 FullVola FaurisNo ratings yet
- Clinical Implications of High Definition Multileaf Collimator (HDMLC) Dosimetric Leaf Gap (DLG) VariationsDocument6 pagesClinical Implications of High Definition Multileaf Collimator (HDMLC) Dosimetric Leaf Gap (DLG) VariationsCargoNo ratings yet
- Particle Size Regression Correction For NIR Spectrum (Tamanho de Particula, MI 2013)Document8 pagesParticle Size Regression Correction For NIR Spectrum (Tamanho de Particula, MI 2013)Mikaelle DutraNo ratings yet
- Quantification of Paracetamol in Intact Tablets Using Near-Infrared Transmittance SpectrosDocument4 pagesQuantification of Paracetamol in Intact Tablets Using Near-Infrared Transmittance SpectrosGabbsgabyNo ratings yet
- Entrance Surface and Ovarian Doses in HysterosalpingographyDocument4 pagesEntrance Surface and Ovarian Doses in HysterosalpingographyTryana HuangNo ratings yet
- 38 FullDocument7 pages38 FullPaulomi PalNo ratings yet
- Serum Protein Profiles in Myasthenia Gravis: Ann Thorac SurgDocument8 pagesSerum Protein Profiles in Myasthenia Gravis: Ann Thorac SurgtotoedahNo ratings yet
- Gallego 2016Document1 pageGallego 2016Nacho Castro IzquierdoNo ratings yet
- Digital Morphometry of Cytologic Aspirate Endometrial SamplesDocument7 pagesDigital Morphometry of Cytologic Aspirate Endometrial SamplesCodruta BelegaNo ratings yet
- J, Watanabe Et Al.2021Document9 pagesJ, Watanabe Et Al.2021Mai M. AlshalNo ratings yet
- 1 s2.0 S016781401634333X MainDocument7 pages1 s2.0 S016781401634333X MainAngelina ProtikNo ratings yet
- Nodal - Multi-Institut Oligo - Plus COREDocument13 pagesNodal - Multi-Institut Oligo - Plus COREsilviuNo ratings yet
- Comparison of Dose Volume Parameters Evaluated UsiDocument15 pagesComparison of Dose Volume Parameters Evaluated UsiBenfredj KhalilNo ratings yet
- Space Novelty Detection in Short Diffusion MRI Scans of Multiple SclerosisDocument3 pagesSpace Novelty Detection in Short Diffusion MRI Scans of Multiple Sclerosisyovof trimsjNo ratings yet
- PIIS0007091217320603Document10 pagesPIIS0007091217320603amjedsenoussiNo ratings yet
- Megbaru 10 PDFDocument7 pagesMegbaru 10 PDFMegbaruNo ratings yet
- Predicting The Risk of Malignancy in Adnexal Masses Based On IOTA AJOG 2016Document14 pagesPredicting The Risk of Malignancy in Adnexal Masses Based On IOTA AJOG 2016Fernando Suarez ChumaceroNo ratings yet
- Comparing Diode & Ion Chamber Arrays for IMRT QADocument13 pagesComparing Diode & Ion Chamber Arrays for IMRT QAenriquefisicoNo ratings yet
- Using_Kaplan_Meier_analysis_together_witDocument10 pagesUsing_Kaplan_Meier_analysis_together_witrayhanckpoyNo ratings yet
- Interobserver and Intraobserver Variability in The Radiological Assessment of Sialolithiasis Using Cone Beam Computed TomographyDocument5 pagesInterobserver and Intraobserver Variability in The Radiological Assessment of Sialolithiasis Using Cone Beam Computed TomographydaruNo ratings yet
- PALMER2013Document19 pagesPALMER2013Andreyson SilvaNo ratings yet
- Abdi Et Al 2023 Operative Treatment of Tarlov Cysts Outcomes and Predictors of Improvement After Surgery a Series of 97Document8 pagesAbdi Et Al 2023 Operative Treatment of Tarlov Cysts Outcomes and Predictors of Improvement After Surgery a Series of 97jabarin.hNo ratings yet
- Application of spectrophotometric analysisDocument8 pagesApplication of spectrophotometric analysisfares adelNo ratings yet
- Silva 155 166Document12 pagesSilva 155 166Antonio Quintero OtoyaNo ratings yet
- Radiologic Assessment of Periapical Health: Comparison of 3 Different Index SystemsDocument5 pagesRadiologic Assessment of Periapical Health: Comparison of 3 Different Index SystemsHari PriyaNo ratings yet
- Radiotherapy and Oncology: Original ArticleDocument8 pagesRadiotherapy and Oncology: Original ArticleJuancarlos Pari SalasNo ratings yet
- Bhandari2020 PaperDocument24 pagesBhandari2020 PapersaraswathiNo ratings yet
- Comparison Between Four Modalities of Radiotherapy of Prostate CancerDocument5 pagesComparison Between Four Modalities of Radiotherapy of Prostate CancerEdis ĐedovićNo ratings yet
- Does The Choice of Spot, Morning or Both Sputum Samples Determine Optimal Performance of A TB Diagnostic Tool?Document7 pagesDoes The Choice of Spot, Morning or Both Sputum Samples Determine Optimal Performance of A TB Diagnostic Tool?diana.alyNo ratings yet
- Gu Et Al. - 2019 - Metabolomics Analysis in Serum From Patients With Colorectal Polyp and Colorectal Cancer by 1H-NMR SpectrometryDocument15 pagesGu Et Al. - 2019 - Metabolomics Analysis in Serum From Patients With Colorectal Polyp and Colorectal Cancer by 1H-NMR Spectrometryyannick brunatoNo ratings yet
- Surgery: SciencedirectDocument7 pagesSurgery: SciencedirectAriska Nur FitrianaNo ratings yet
- DetectionDocument19 pagesDetectionTommy S.No ratings yet
- j.brachy.2015.02.192Document8 pagesj.brachy.2015.02.192Andreyson SilvaNo ratings yet
- Clinical Applications of Nuclear Medicine Targeted TherapyFrom EverandClinical Applications of Nuclear Medicine Targeted TherapyEmilio BombardieriNo ratings yet
- Riel Comun Fstguide2Document2 pagesRiel Comun Fstguide2Rosita TejedaNo ratings yet
- Payroll Accounting 2015 1st Edition Landin Test Bank 1Document106 pagesPayroll Accounting 2015 1st Edition Landin Test Bank 1dorothy100% (47)
- Nikon Nivo C Series Instruction ManualDocument65 pagesNikon Nivo C Series Instruction ManualBambang Deriyanto100% (1)
- SorghumDocument13 pagesSorghumMohaajanan AliNo ratings yet
- Reactor & Impeller Design in Hydrogenation: GBHE Technical Bulletin CTB #79Document13 pagesReactor & Impeller Design in Hydrogenation: GBHE Technical Bulletin CTB #79manuNo ratings yet
- Analysis of Alloy Constituents (Cu and ZnDocument5 pagesAnalysis of Alloy Constituents (Cu and Znaryan kushwaha100% (2)
- Working Length Determination in RCTDocument38 pagesWorking Length Determination in RCTDidar Sadiq Kwekha100% (1)
- 4 Dec - Elis Vs ElisDocument6 pages4 Dec - Elis Vs ElisRichard TenorioNo ratings yet
- Flame Amplifier HoneywellDocument8 pagesFlame Amplifier Honeywellgavo vargoNo ratings yet
- Exxonmobil High Density Polyethylene Product Guide: Extrusion MoldingDocument6 pagesExxonmobil High Density Polyethylene Product Guide: Extrusion MoldingDaikinllcNo ratings yet
- ZinkPower Batam - Company BrochureDocument6 pagesZinkPower Batam - Company BrochureansarALLAAHNo ratings yet
- MEH B1 Video Book Answer KeyDocument6 pagesMEH B1 Video Book Answer KeyTru CallingNo ratings yet
- RS9923 - Grade 12 Compulsory Subjects - Test Specification Chart and Model Questions - FinalDocument32 pagesRS9923 - Grade 12 Compulsory Subjects - Test Specification Chart and Model Questions - FinalPrince JaiswalNo ratings yet
- Examination of Power Electronics (Pel) : AnswerDocument10 pagesExamination of Power Electronics (Pel) : Answerves vegasNo ratings yet
- 2requirements Permit PDFDocument1 page2requirements Permit PDFHazel CorralNo ratings yet
- Worlds Healthiest Super Food - SpirulinaDocument16 pagesWorlds Healthiest Super Food - SpirulinaBhadra BasumataryNo ratings yet
- A Study On Satisfaction Level of Employees With Special Reference Textile IndustryDocument12 pagesA Study On Satisfaction Level of Employees With Special Reference Textile Industrysai kiran bade100% (1)
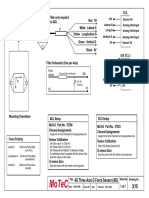
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- Rakovic Dejan - Arandjelovic Slavica - Micovic Mirjana - Quantum-Informational Medicine QIM 2011 PDFDocument150 pagesRakovic Dejan - Arandjelovic Slavica - Micovic Mirjana - Quantum-Informational Medicine QIM 2011 PDFPrahovoNo ratings yet
- Public Stormwater Management With Green StreetsDocument90 pagesPublic Stormwater Management With Green StreetsPranay ManwarNo ratings yet
- 14 People V Manalo (Verba Legis)Document15 pages14 People V Manalo (Verba Legis)zeynNo ratings yet
- DC532: 16 Digital Inputs and 16 Digital Outputs Module for S500 PLCDocument3 pagesDC532: 16 Digital Inputs and 16 Digital Outputs Module for S500 PLCVinay SaiNo ratings yet
- Lab Manual - Skull Bones - English - Student - Fill inDocument6 pagesLab Manual - Skull Bones - English - Student - Fill inthejaskumar2026No ratings yet