You might also like
- Jbmoa 07 00257Document6 pagesJbmoa 07 00257susithraNo ratings yet
- Dengue The Breakbone Fever A Crisis WithDocument9 pagesDengue The Breakbone Fever A Crisis WithUTHSO NANDYNo ratings yet
- Jurnal NursngDocument14 pagesJurnal NursngEraCitraNo ratings yet
- 01 Daljeet KaurDocument9 pages01 Daljeet KaurOcta VianiNo ratings yet
- Guzman 2010Document3 pagesGuzman 2010Renaldi ArdiyaNo ratings yet
- Dengue PCFM REPORT 1st RevisionDocument14 pagesDengue PCFM REPORT 1st RevisionTartaglia IIINo ratings yet
- Dengue Hemorrhagic Fever: Past, Present and Future DevelopmentsDocument14 pagesDengue Hemorrhagic Fever: Past, Present and Future DevelopmentsDyraWirasasmitaMirsanNo ratings yet
- Vector Control Interventions To Prevent Dengue IndiaDocument7 pagesVector Control Interventions To Prevent Dengue IndiaShadows BlameNo ratings yet
- Raza Et Al-2019-Advances in Difference EquationsDocument19 pagesRaza Et Al-2019-Advances in Difference EquationsShoaib ArifNo ratings yet
- A Literature Review On DengueDocument5 pagesA Literature Review On DengueFrancico XavierNo ratings yet
- Dengue Haemorrhagic Fever: A Job Done Via Exosomes?: Emerging Microbes & InfectionsDocument11 pagesDengue Haemorrhagic Fever: A Job Done Via Exosomes?: Emerging Microbes & InfectionsJuan Fernando BermúdezNo ratings yet
- Facts: Geographic DistributionDocument3 pagesFacts: Geographic DistributionMarianne R. LorenzoNo ratings yet
- Paper Dengue FeverDocument5 pagesPaper Dengue FeverMardiano PutraNo ratings yet
- Infections of Dengue Viruses in Belgaum, Karnataka and India, Dengue in BelgaumDocument120 pagesInfections of Dengue Viruses in Belgaum, Karnataka and India, Dengue in BelgaumJ NuchinNo ratings yet
- Dengue in IndiaDocument10 pagesDengue in IndiaMohiniNo ratings yet
- MBHSJDocument7 pagesMBHSJsarahsaNo ratings yet
- DengueDocument32 pagesDenguetummalapalli venkateswara rao100% (3)
- 35 PDFDocument10 pages35 PDFChika FebrianiNo ratings yet
- Q3-Health DengueDocument29 pagesQ3-Health Denguenormalguy34kNo ratings yet
- Dengue Viral Infections: ReviewDocument14 pagesDengue Viral Infections: ReviewALHUSNA YAINNo ratings yet
- Dengue Viral Infections: ReviewDocument14 pagesDengue Viral Infections: Reviewjeanne_mbNo ratings yet
- Severe Dengue in Travellers - JTMDocument36 pagesSevere Dengue in Travellers - JTMSulindri IntanNo ratings yet
- Etiologi (DF, DHF, DSS, Cikungunya, Zika) : Figure 2. Transmission of Dengue VirusesDocument43 pagesEtiologi (DF, DHF, DSS, Cikungunya, Zika) : Figure 2. Transmission of Dengue Virusestiffa0711No ratings yet
- Water-Borne Dengue: A Mosquito DiseaseDocument16 pagesWater-Borne Dengue: A Mosquito DiseaseJaylive AnziaNo ratings yet
- Dengue PreventionDocument8 pagesDengue PreventionMaria Elvira Abrogena DuadNo ratings yet
- A Case Study On DengueDocument11 pagesA Case Study On DengueYetTamparong100% (1)
- Malavige PDFDocument14 pagesMalavige PDFirenesmbNo ratings yet
- 1194-Article Text-5520-1-10-20200717Document8 pages1194-Article Text-5520-1-10-20200717Heryanti PusparisaNo ratings yet
- Dengue Reviewarticle Mss BRK PDFDocument11 pagesDengue Reviewarticle Mss BRK PDFkillerleeNo ratings yet
- Dengue Infection Global Importance, Immunopathology and ManagementDocument5 pagesDengue Infection Global Importance, Immunopathology and ManagementAlice in wonderlandNo ratings yet
- Dengue ControlDocument2 pagesDengue ControlJosephine Bauyon MedinaNo ratings yet
- Dengue 3y1 2Document37 pagesDengue 3y1 2johnmichael008No ratings yet
- Progress Towards A Dengue VaccineDocument10 pagesProgress Towards A Dengue VaccineAna MendozaNo ratings yet
- Blood DisorderDocument32 pagesBlood DisorderJaezee RamosNo ratings yet
- What Is Dengue?: The VirusDocument1 pageWhat Is Dengue?: The VirusRogie SaludoNo ratings yet
- Dengue Math Biol 35Document22 pagesDengue Math Biol 35gurumatNo ratings yet
- Mst-Case Management (2) - KS - P2M 2022Document40 pagesMst-Case Management (2) - KS - P2M 2022Atikah AbayNo ratings yet
- Dengue 1Document14 pagesDengue 1FikaAuliaNo ratings yet
- Apjtb 01 04 326Document2 pagesApjtb 01 04 326Kennard Aristo ArifinNo ratings yet
- Dengue Awarerness Program 2Document19 pagesDengue Awarerness Program 2Ashok MaramNo ratings yet
- Dengue ClinicalKeyDocument34 pagesDengue ClinicalKeyJuan David OviedoNo ratings yet
- Dengue Fever PDFDocument8 pagesDengue Fever PDFushapadminivadivelswamyNo ratings yet
- Dengue (Lancet)Document16 pagesDengue (Lancet)Roberth Mero100% (1)
- Understanding Dengue: Causes, Symptoms, Prevention and TreatmentDocument34 pagesUnderstanding Dengue: Causes, Symptoms, Prevention and Treatmentmaharshi mNo ratings yet
- Is Dengue A Threat To The Blood Supply?: D. Teo, L. C. NG & S. LamDocument12 pagesIs Dengue A Threat To The Blood Supply?: D. Teo, L. C. NG & S. LamCristhian ReyesNo ratings yet
- Vitamins and DengueDocument13 pagesVitamins and DengueShuvo DasNo ratings yet
- Dengue Case StudyDocument8 pagesDengue Case StudysusanausquizaNo ratings yet
- Dengue LancetDocument16 pagesDengue LancetJorge Ricardo Uchuya GómezNo ratings yet
- Dengue: Human Viral DiseasesDocument4 pagesDengue: Human Viral DiseasesMichelle EscobarNo ratings yet
- JHVRV 05 00179 PDFDocument7 pagesJHVRV 05 00179 PDFTiahNo ratings yet
- Dengue Clinical Presentation and ManagementDocument60 pagesDengue Clinical Presentation and Managementar_thikaNo ratings yet
- Dengue and Dengue Hemorrhagic FeverDocument5 pagesDengue and Dengue Hemorrhagic FeverairasofiaNo ratings yet
- Final DengueDocument61 pagesFinal DengueApril Daye B. AsuncionNo ratings yet
- DENGUE HEMORRHAGIC FEVER-final N ToDocument52 pagesDENGUE HEMORRHAGIC FEVER-final N ToRachel Ann CorpuzNo ratings yet
- Dengue: Mosquito-Borne Viral Infection Affecting Hundreds of MillionsDocument4 pagesDengue: Mosquito-Borne Viral Infection Affecting Hundreds of Millionsycc2327No ratings yet
- 3 MICRO 12 - Emerging and Re-Emerging Infectious Diseases - Dr. RosarioDocument7 pages3 MICRO 12 - Emerging and Re-Emerging Infectious Diseases - Dr. RosarioyayayanizaNo ratings yet
- Epidemiology: Transmission of The Dengue VirusDocument4 pagesEpidemiology: Transmission of The Dengue Viruschiquilon749No ratings yet
- Seminar: Annelies Wilder-Smith, Eng-Eong Ooi, Olaf Horstick, Bridget WillsDocument14 pagesSeminar: Annelies Wilder-Smith, Eng-Eong Ooi, Olaf Horstick, Bridget WillsAlexander ArguelloNo ratings yet
- 13 Who - Int-Dengue and Severe DengueDocument5 pages13 Who - Int-Dengue and Severe DengueJannaNo ratings yet
- Global Perspectives on the Transmission of Zoonotic RNA Viruses from Wild Animal Species to Humans: Zoonotic, Epizootic, and Anthropogenic Viral PathogensFrom EverandGlobal Perspectives on the Transmission of Zoonotic RNA Viruses from Wild Animal Species to Humans: Zoonotic, Epizootic, and Anthropogenic Viral PathogensNo ratings yet
- dm2022 0433Document15 pagesdm2022 0433Charlemagne Sabio GalamgamNo ratings yet
- Guesstimate The Number of COVID Testing Kits Needed by Delhi in OctoberDocument6 pagesGuesstimate The Number of COVID Testing Kits Needed by Delhi in OctobersaiNo ratings yet
- Stress and Conflict Management: The Way To Resilience and SatisfactionDocument6 pagesStress and Conflict Management: The Way To Resilience and SatisfactionMariusNo ratings yet
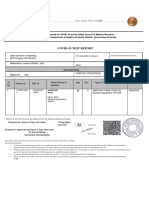
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)aishwaryaNo ratings yet
- Zhuhai Lituo Biotechnology Co., LTD: Leading Technology For Healthy LifeDocument32 pagesZhuhai Lituo Biotechnology Co., LTD: Leading Technology For Healthy LifeFrancisca RamliNo ratings yet
- Interpreting COVID-19 lab resultsDocument6 pagesInterpreting COVID-19 lab resultsDari VillaNo ratings yet
- Frequently Asked Questions Regarding COVID-19 - v8Document9 pagesFrequently Asked Questions Regarding COVID-19 - v8Pannaga NandanNo ratings yet
- Lunit Insight CXR Openvino Solution BriefDocument3 pagesLunit Insight CXR Openvino Solution BriefDebora NunesNo ratings yet
- A Quarterly Publication of The Central Office On ICD-10-CM/PCSDocument34 pagesA Quarterly Publication of The Central Office On ICD-10-CM/PCSharu haroonNo ratings yet
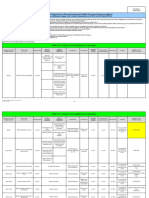
- List of Rapid Antigen Kits 11052021Document13 pagesList of Rapid Antigen Kits 11052021Subhankar SahaNo ratings yet
- LPL - Production Test Collection Centre Sector - 18, Block-E Rohini DELHI 110085Document2 pagesLPL - Production Test Collection Centre Sector - 18, Block-E Rohini DELHI 110085Manav ChhabraNo ratings yet
- Covid19 Diagnostic Products List - enDocument59 pagesCovid19 Diagnostic Products List - enVickyNo ratings yet
- Yashika RajDocument1 pageYashika RajNitin RajeevNo ratings yet
- Covid-19 Status As of May 4 2023Document52 pagesCovid-19 Status As of May 4 2023Kristin VillasenotNo ratings yet
- Rootcauseanalysis Invalid IC PCRDocument6 pagesRootcauseanalysis Invalid IC PCRrpl5polbanNo ratings yet
- ASHISH KESHRI (1) Detailed ReportDocument1 pageASHISH KESHRI (1) Detailed ReportShatabdi VermaNo ratings yet
- Davao Doctors College, Inc.: Gen. Malvar ST., Davao City College of Allied Health Sciences - Nursing ProgramDocument20 pagesDavao Doctors College, Inc.: Gen. Malvar ST., Davao City College of Allied Health Sciences - Nursing ProgramPRECIOUS DIANNE BARDON-MEMPINNo ratings yet
- Final Report - Expedite The Laboratory Investigation of Covid19 Ravi KumudeshDocument33 pagesFinal Report - Expedite The Laboratory Investigation of Covid19 Ravi KumudeshRavi KumudeshNo ratings yet
- Name Date of Birth Passport Number (Verified On Site) COVID Testing Service E-ManifestDocument1 pageName Date of Birth Passport Number (Verified On Site) COVID Testing Service E-ManifestAnna AnnaNo ratings yet
- Eul Covid19 Ivd UpdateDocument3 pagesEul Covid19 Ivd UpdateArya KusumaNo ratings yet
- Covid-19 Among Neonates: Experience From An Sncu of A Tertiary Care Hospital in Eastern IndiaDocument4 pagesCovid-19 Among Neonates: Experience From An Sncu of A Tertiary Care Hospital in Eastern IndiaIJAR JOURNALNo ratings yet
- AmandeepDocument2 pagesAmandeepUppili PranavaneNo ratings yet
- Covid 19Document31 pagesCovid 19Lee BuelaNo ratings yet
- Madhav GuptaDocument1 pageMadhav GuptaLABNo ratings yet
- FWCQ22 COVID19 Healthcare Protocol V28 EnglishDocument24 pagesFWCQ22 COVID19 Healthcare Protocol V28 EnglishKarthik KothandaramanNo ratings yet
- SALIXIUM COVID-19 Rapid Antigen Test Flyer - ENG - 2021.07.16 - V6 (2 Pages)Document2 pagesSALIXIUM COVID-19 Rapid Antigen Test Flyer - ENG - 2021.07.16 - V6 (2 Pages)driftailNo ratings yet
- Policy WordingDocument13 pagesPolicy WordingenahhNo ratings yet
- Ethics WorksheetDocument10 pagesEthics WorksheetJeralyn Gamo SevillenoNo ratings yet
- Covid-19 AddendumDocument10 pagesCovid-19 AddendumPrecious Bardon-MempinNo ratings yet
- CONFIDENTIAL - Klinik Ratulangi Medical Center - January 2023Document20 pagesCONFIDENTIAL - Klinik Ratulangi Medical Center - January 2023Ratulangi Medical CentreNo ratings yet