You might also like
- Art. FisuradosDocument11 pagesArt. FisuradosInma Coronado de la TorreNo ratings yet
- Clinical Assessment of Short Implants Retsining Removsble Partial DenturesDocument7 pagesClinical Assessment of Short Implants Retsining Removsble Partial DenturesLouis HutahaeanNo ratings yet
- Child Neglect in Rich Nations - Sylvia HewlettDocument70 pagesChild Neglect in Rich Nations - Sylvia HewlettMarko KrstićNo ratings yet
- Lifting Vs Volumizing-The Difference in Facial Minimally Invasive Procedures When Respecting The Line of LigamentsDocument7 pagesLifting Vs Volumizing-The Difference in Facial Minimally Invasive Procedures When Respecting The Line of LigamentsArcelino Farias100% (1)
- i1945-7103-92-2-161Document12 pagesi1945-7103-92-2-161mlnunezNo ratings yet
- Coronally Advanced Flap With and Without VerticalDocument13 pagesCoronally Advanced Flap With and Without VerticalLEONARDO ALBERTO CRESPIN ZEPEDANo ratings yet
- 10 1067@mpr 2000 107113Document7 pages10 1067@mpr 2000 107113gbaez.88No ratings yet
- Does The Maxillary Midline Diastema Close After Frenectomy?: Oral SurgeryDocument10 pagesDoes The Maxillary Midline Diastema Close After Frenectomy?: Oral Surgeryantonio dlNo ratings yet
- Current Practice For Transverse Mandibular and Maxillary Discrepancies in The NetherlandsDocument10 pagesCurrent Practice For Transverse Mandibular and Maxillary Discrepancies in The NetherlandsDONGXU LIUNo ratings yet
- Cekic Nagas2016 PDFDocument8 pagesCekic Nagas2016 PDFAkanksha MahajanNo ratings yet
- 10 1016@j Joms 2012 03 016Document12 pages10 1016@j Joms 2012 03 016Karam EidNo ratings yet
- Examination of Antimicrobial and AntiinfDocument66 pagesExamination of Antimicrobial and AntiinfCristina CapettiNo ratings yet
- Periodontal Plastic Surgery To Improve AestheticsDocument7 pagesPeriodontal Plastic Surgery To Improve AestheticsElizabet KalmykovaNo ratings yet
- i1945-7103-92-4-431Document15 pagesi1945-7103-92-4-431mlnunezNo ratings yet
- Cambiano Nonsurgical Treatment and Stability of An Adult With A Severe Anterior Openbite MalocclusionDocument9 pagesCambiano Nonsurgical Treatment and Stability of An Adult With A Severe Anterior Openbite MalocclusionAlex ReaNo ratings yet
- Jawline Contouring AlfaroDocument5 pagesJawline Contouring AlfaroÂngelo Rosso LlantadaNo ratings yet
- IVOJI-Contemporary Management of AnDocument8 pagesIVOJI-Contemporary Management of AnivojiNo ratings yet
- Long-Term Stability of Anterior Open-Bite Treatment by Intrusion of Maxillary Posterior TeethDocument9 pagesLong-Term Stability of Anterior Open-Bite Treatment by Intrusion of Maxillary Posterior TeethNg Chun HownNo ratings yet
- Periodontal Status of Impacted Maxillary CaninesDocument5 pagesPeriodontal Status of Impacted Maxillary CaninesDiana ElíasNo ratings yet
- The Philippine Journal of Orthodontics: ISSN: 0115-3498Document42 pagesThe Philippine Journal of Orthodontics: ISSN: 0115-3498Thomas Karl Anthony QUILANGNo ratings yet
- Guerrero 1997Document10 pagesGuerrero 1997Deyvid Gustavo Capelo RiosNo ratings yet
- Fratura Condilar - AnquiloseDocument8 pagesFratura Condilar - AnquiloseMatheus MoraisNo ratings yet
- Stability of Anterior Crossbite CorrectionDocument8 pagesStability of Anterior Crossbite CorrectionannysaNo ratings yet
- Cleft Maxillary Distraction Versus Orthognathic Surgery: Clinical Morbidities and Surgical RelapseDocument13 pagesCleft Maxillary Distraction Versus Orthognathic Surgery: Clinical Morbidities and Surgical RelapseRohan BhagatNo ratings yet
- Flow Chart Perio Ortho 1-S2.0-S1761722721001431-Main PDFDocument14 pagesFlow Chart Perio Ortho 1-S2.0-S1761722721001431-Main PDFSofia Zaematul ArifahNo ratings yet
- Alveolar Bone and Epithelial Attachment Status Following Two Different Closed-Eruption Surgical Techniques For Impacted Maxillary Central IncisorsDocument6 pagesAlveolar Bone and Epithelial Attachment Status Following Two Different Closed-Eruption Surgical Techniques For Impacted Maxillary Central IncisorsAndres CoboNo ratings yet
- Atm ArtDocument6 pagesAtm ArtYessyka EscalanteNo ratings yet
- Risk Factors Associated With Early Implant Failure: A 5-Year Retrospective Clinical StudyDocument6 pagesRisk Factors Associated With Early Implant Failure: A 5-Year Retrospective Clinical StudystortoNo ratings yet
- Novel surgical approach for deep recession coverageDocument6 pagesNovel surgical approach for deep recession coverageJoshua Diaz QuiquijanaNo ratings yet
- Two Bilateral Zygomatic Implants Placed and Immediately Loaded A Retrospective Chart Review With Up-To-54-Month Follow-UpDocument5 pagesTwo Bilateral Zygomatic Implants Placed and Immediately Loaded A Retrospective Chart Review With Up-To-54-Month Follow-UpBagis Emre Gul100% (1)
- Long Term Vertical ChangesDocument5 pagesLong Term Vertical ChangesthganooNo ratings yet
- Management of Sub Condylar Fracture in 15 Yr Old Patient: Case ReportDocument6 pagesManagement of Sub Condylar Fracture in 15 Yr Old Patient: Case ReportIma ShofyaNo ratings yet
- Winitsky 2018Document8 pagesWinitsky 2018Bagis Emre GulNo ratings yet
- S088954062100442XDocument11 pagesS088954062100442Xleoncio cabrera rojasNo ratings yet
- Artigo 5Document9 pagesArtigo 5joao pauloNo ratings yet
- A Comparison of Treatment Results of Adult Deep-Bite Cases Treated With Lingual and Labial Fixed AppliancesDocument7 pagesA Comparison of Treatment Results of Adult Deep-Bite Cases Treated With Lingual and Labial Fixed AppliancesScribd AccountNo ratings yet
- Skeletal Width Changes After Mini-Implant-Assisted Rapid Maxillary Expansion (MARME) in Young AdultsDocument6 pagesSkeletal Width Changes After Mini-Implant-Assisted Rapid Maxillary Expansion (MARME) in Young AdultsRolando Huaman BravoNo ratings yet
- Distal Wedge Technique SelectionDocument9 pagesDistal Wedge Technique SelectionJoshua Diaz QuiquijanaNo ratings yet
- Stalpers Am JOrthod Dentofac Orthop 2007132316323Document8 pagesStalpers Am JOrthod Dentofac Orthop 2007132316323thomas QuilangNo ratings yet
- Maxillary Arch Distalization Using Interradicular Miniscrews and The Lever-Arm ApplianceDocument8 pagesMaxillary Arch Distalization Using Interradicular Miniscrews and The Lever-Arm ApplianceJuan Carlos CárcamoNo ratings yet
- Dentigerous Cyst Treatment in ChildrenDocument35 pagesDentigerous Cyst Treatment in ChildrenRifaniNo ratings yet
- Maxillary expansion effects of bone-borne appliance in young vs late adolescentsDocument13 pagesMaxillary expansion effects of bone-borne appliance in young vs late adolescentsDr.Thrivikhraman KothandaramanNo ratings yet
- 2021 Does The Timing of 1-Stage Palatoplasty With Radical Muscle Dissection Effect Long-Term Midface Growth A Single-Center Retrospective AnalysisDocument7 pages2021 Does The Timing of 1-Stage Palatoplasty With Radical Muscle Dissection Effect Long-Term Midface Growth A Single-Center Retrospective AnalysisDimitris RodriguezNo ratings yet
- Parameters Deciding Orthognathic Surgery or Camouflage? - A ReviewDocument8 pagesParameters Deciding Orthognathic Surgery or Camouflage? - A ReviewDr. Sagar S BhatNo ratings yet
- Surgical Reconstruction of Interdental PDocument11 pagesSurgical Reconstruction of Interdental PMaria Jose GodoyNo ratings yet
- Zucchelli 2010Document8 pagesZucchelli 2010Evan BlackwellNo ratings yet
- Sri Dwi Mutiara - Jurnal Maloklusi 1Document8 pagesSri Dwi Mutiara - Jurnal Maloklusi 1sri dwi mutiaraNo ratings yet
- Openbite CamouflageDocument8 pagesOpenbite CamouflageRakesh RaveendranNo ratings yet
- Berlin Et Al (2023) Multidisciplinary Approach For Autotransplantation and Restoration of A Maxillary PremolarDocument7 pagesBerlin Et Al (2023) Multidisciplinary Approach For Autotransplantation and Restoration of A Maxillary PremolarISAI FLORES PÉREZNo ratings yet
- 1 s2.0 S027823911501438XDocument8 pages1 s2.0 S027823911501438Xhyl776210No ratings yet
- Mandibular Incisor Alignment in Untreated Subjects Compared With Long-Term Changes After OrthodonticDocument9 pagesMandibular Incisor Alignment in Untreated Subjects Compared With Long-Term Changes After OrthodonticPAOLA IVETTE MARTINEZ RODRIGUEZNo ratings yet
- Pos Nick 2004Document16 pagesPos Nick 2004Bhárbara Marinho BarcellosNo ratings yet
- Clinical Efficacy of Periodontal Plastic Surgery Procedures Consensus Report of Group 2 of The 10th European Workshop On PeriodontologyDocument8 pagesClinical Efficacy of Periodontal Plastic Surgery Procedures Consensus Report of Group 2 of The 10th European Workshop On PeriodontologyImplant DentNo ratings yet
- Journal ProstoDocument6 pagesJournal ProstoAvila Aita Harun RasyidNo ratings yet
- Reduced Need For Alveolar Bone Grafting by Presurgical Orthopedics and Pimary GingivoperiosteoplastyDocument4 pagesReduced Need For Alveolar Bone Grafting by Presurgical Orthopedics and Pimary GingivoperiosteoplastynoraveNo ratings yet
- Bompereta Labial 2Document7 pagesBompereta Labial 2Aleja LombanaNo ratings yet
- PlicacionesencirugiaDocument5 pagesPlicacionesencirugiahelvi fridayaniNo ratings yet
- International Journal of Surgery Case Reports: Kanistika Jha, Manoj AdhikariDocument4 pagesInternational Journal of Surgery Case Reports: Kanistika Jha, Manoj AdhikariYeraldin EspañaNo ratings yet
- Artigo BomDocument6 pagesArtigo BomCiro GassibeNo ratings yet
- Open Reduction With Internal Fixation of Mandibular Angle Fractures: A Retrospective StudyDocument6 pagesOpen Reduction With Internal Fixation of Mandibular Angle Fractures: A Retrospective StudyRudnapon AmornlaksananonNo ratings yet
- Graftless Solutions for the Edentulous PatientFrom EverandGraftless Solutions for the Edentulous PatientSaj JivrajNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- Dentistry JournalDocument9 pagesDentistry JournalAlex ReaNo ratings yet
- Chunlei Xun Microscrew Anchorage in Skeletal AnteriorDocument10 pagesChunlei Xun Microscrew Anchorage in Skeletal AnteriorAlex ReaNo ratings yet
- CHUI SHAN Orthodontic Treatment of Anterior Open BiteDocument6 pagesCHUI SHAN Orthodontic Treatment of Anterior Open BiteAlex ReaNo ratings yet
- Cambiano Nonsurgical Treatment and Stability of An Adult With A Severe Anterior Openbite MalocclusionDocument9 pagesCambiano Nonsurgical Treatment and Stability of An Adult With A Severe Anterior Openbite MalocclusionAlex ReaNo ratings yet
- Psychopathic Personality: Bridging The Gap Between Scientific Evidence and Public PolicyDocument69 pagesPsychopathic Personality: Bridging The Gap Between Scientific Evidence and Public PolicyGokushimakNo ratings yet
- Canine-Assisted Occupational Therapy For Children On The Autism Spectrum: Parents' PerspectivesDocument10 pagesCanine-Assisted Occupational Therapy For Children On The Autism Spectrum: Parents' PerspectivesDaniele PendezaNo ratings yet
- Hazards of Nitrogen AsphyxiationDocument10 pagesHazards of Nitrogen AsphyxiationRaja Senthil NathanNo ratings yet
- Acute Respiratory Distress Syndrome: Jason D. Sciarretta, M.D. Critical Care Conference October 13, 2010Document24 pagesAcute Respiratory Distress Syndrome: Jason D. Sciarretta, M.D. Critical Care Conference October 13, 2010JelenaNo ratings yet
- Neonatal Care Pocket Guide For Hospital Physicians PDFDocument319 pagesNeonatal Care Pocket Guide For Hospital Physicians PDFelmaadawy2002100% (7)
- The Works of Alan OpenshawDocument38 pagesThe Works of Alan OpenshawAlan OpenshawNo ratings yet
- Managing Painful Diabetic NeuropathyDocument26 pagesManaging Painful Diabetic NeuropathyAthalia TalawayNo ratings yet
- Borderline Personality DisorderDocument7 pagesBorderline Personality DisorderleaNo ratings yet
- Pseudostrabismus ExplainedDocument3 pagesPseudostrabismus ExplainedbebetangNo ratings yet
- Appendix7 I-131Document4 pagesAppendix7 I-131Crizzz001No ratings yet
- Theory Critique of Boundaries in MarriageDocument8 pagesTheory Critique of Boundaries in MarriagepatrickakingNo ratings yet
- 2020 Corportate Sustainability ReportDocument22 pages2020 Corportate Sustainability ReportMohamed KannouNo ratings yet
- A Critical Review of The Effect of Working Conditions On Employee PerformanceDocument11 pagesA Critical Review of The Effect of Working Conditions On Employee PerformanceStephanie Bacunawa0% (1)
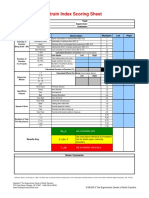
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- Concept PaperDocument3 pagesConcept Papergladylou siocoNo ratings yet
- Round Hill Community Garden FAQ - Round Hill, VirginiaDocument3 pagesRound Hill Community Garden FAQ - Round Hill, VirginiaZafiriou MavrogianniNo ratings yet
- Change Your Life in 7 Days With NLP - Paul Mckenna BrochureDocument2 pagesChange Your Life in 7 Days With NLP - Paul Mckenna Brochureapi-385316675% (4)
- Ent Solved Kmu Seqs by RMC StudentsDocument68 pagesEnt Solved Kmu Seqs by RMC StudentsAamir Khan100% (1)
- The Effect of Potassium Permanganate (KMnO4) Concentration and Storage Time on Quality of California Papaya (Carica papaya LDocument8 pagesThe Effect of Potassium Permanganate (KMnO4) Concentration and Storage Time on Quality of California Papaya (Carica papaya LSyifa UlNo ratings yet
- 1.2 POWERPOINT History of ForensicsDocument23 pages1.2 POWERPOINT History of ForensicsSilay Parole & ProbationNo ratings yet
- Human Population and EnvironmentDocument4 pagesHuman Population and Environmentmonkeybike88No ratings yet
- Pedia ComputationsDocument5 pagesPedia ComputationsRheenz Fornoles100% (1)
- Effects of Energy Gel Ingestion On Blood Glucose, Lactate, and Performance Measures During Prolonged CyclingDocument9 pagesEffects of Energy Gel Ingestion On Blood Glucose, Lactate, and Performance Measures During Prolonged Cyclingjose david HerreraNo ratings yet
- MSDS for Feldspar PowderDocument7 pagesMSDS for Feldspar PowderRıdvan SürmeliNo ratings yet
- Midwifery LedDocument15 pagesMidwifery LedRizka Dita Hidayati100% (1)
- DISC2-14071 AppealLetter PublicCommentsDocument17 pagesDISC2-14071 AppealLetter PublicCommentsJames ParsonsNo ratings yet
- NCP LymphomaDocument3 pagesNCP Lymphomamahmoud fuqahaNo ratings yet
- 210 419 1 SMDocument4 pages210 419 1 SMIneMeilaniNo ratings yet