You might also like
- Local Media4154693009839718894-2Document3 pagesLocal Media4154693009839718894-2MAY JOY MARQUEZNo ratings yet
- Hypovolemia: Lozada - Marcelo - Maulana - Oliver - Ombo - PadillaDocument10 pagesHypovolemia: Lozada - Marcelo - Maulana - Oliver - Ombo - PadillaMudzna MaulanaNo ratings yet
- AssessmentDocument14 pagesAssessmentAdriane VillanuevaNo ratings yet
- Nursing Care Plan for Urinary Retention ManagementDocument2 pagesNursing Care Plan for Urinary Retention ManagementCherry CayabyabNo ratings yet
- NCP Deficient Fluid VolumeDocument3 pagesNCP Deficient Fluid VolumeDoneva Lyn MedinaNo ratings yet
- Fluid Volume Deficit Related To Loose Watery Stool Diarrhea)Document2 pagesFluid Volume Deficit Related To Loose Watery Stool Diarrhea)Jesse James Advincula Edjec100% (15)
- NCP-Fluid Volume DeficitDocument2 pagesNCP-Fluid Volume Deficitanon_207994234100% (1)
- Wala Na Jud Koy Masuka,"Document4 pagesWala Na Jud Koy Masuka,"INTERO, GERALD JANE S.No ratings yet
- NursingCarePlanGroup4 RevisedDocument3 pagesNursingCarePlanGroup4 Revisedjae jaeNo ratings yet
- Nursing Care Plan: Cues/Clues Nursing Diagnosis Plan Intervention Rationale EvaluationDocument1 pageNursing Care Plan: Cues/Clues Nursing Diagnosis Plan Intervention Rationale EvaluationJoanna Jaira SalcedoNo ratings yet
- NCP of PTBDocument8 pagesNCP of PTBdisenueve_jhOanneNo ratings yet
- Fluid Volume Deficit Related To Active Fluid Volume LossDocument3 pagesFluid Volume Deficit Related To Active Fluid Volume LossMelDred Cajes BolandoNo ratings yet
- College of Nursing and Allied Medical Sciences: WesleyanDocument3 pagesCollege of Nursing and Allied Medical Sciences: WesleyanPrince Juzzel Banag100% (1)
- AssminentDocument2 pagesAssminentnajm ktkNo ratings yet
- Patient Verbalizes Understanding of Causative Factors and Purpose of Individual Therapeutic Interventions and MedicationsDocument3 pagesPatient Verbalizes Understanding of Causative Factors and Purpose of Individual Therapeutic Interventions and MedicationsSheenaGuinoCullaNo ratings yet
- Assessment Diagnosis Planning Intervention EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention EvaluationPatricia Ellise JuatNo ratings yet
- Assessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Short Term: Independent: Short Term: Goal Partially MetDocument3 pagesAssessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Short Term: Independent: Short Term: Goal Partially MetPrincess Mildred AbdonNo ratings yet
- NURSING CARE PLAN FOR DIARRHEADocument2 pagesNURSING CARE PLAN FOR DIARRHEAKrizha Angela NicolasNo ratings yet
- NCP. Deficient Fluid Volume by Eben D.C.Document1 pageNCP. Deficient Fluid Volume by Eben D.C.dominoredwing2024100% (1)
- PneumoniaDocument2 pagesPneumoniaPia MedinaNo ratings yet
- Ate Gabs Nyo Pagod NaDocument3 pagesAte Gabs Nyo Pagod NaGabrielle EvangelistaNo ratings yet
- Hydration and Constipation ManagementDocument3 pagesHydration and Constipation ManagementCharissa de LeonNo ratings yet
- UTI in A Pregnant Woman - NCPDocument6 pagesUTI in A Pregnant Woman - NCPella joyce75% (4)
- College of Nursing: Assessment Diagnosis Analysis Planning Implementation Rationale EvaluationDocument2 pagesCollege of Nursing: Assessment Diagnosis Analysis Planning Implementation Rationale EvaluationDiana Anne MarisNo ratings yet
- Deficient Fluid Volume (AGEDocument2 pagesDeficient Fluid Volume (AGENursesLabs.com83% (6)
- BSN2 C Ihps NCP FinalDocument7 pagesBSN2 C Ihps NCP FinalAdrian DecolongonNo ratings yet
- Impaired Swallowing Related To Dysphagia Secondary To Dry Oral MucosaDocument3 pagesImpaired Swallowing Related To Dysphagia Secondary To Dry Oral MucosaJUN JUN PALISOC100% (1)
- NCP Peptic Ulcer DsDocument4 pagesNCP Peptic Ulcer Dsplug0650% (10)
- Subjective Data: Long Term Goal: Diagnostic:: "I Was Trying To Vomit in The Emergency Department."Document5 pagesSubjective Data: Long Term Goal: Diagnostic:: "I Was Trying To Vomit in The Emergency Department."Erle Gray CadangenNo ratings yet
- Nursing Care Plan: Cues/Clues Nursing Diagnosis Plan Intervention Rationale EvaluationDocument1 pageNursing Care Plan: Cues/Clues Nursing Diagnosis Plan Intervention Rationale EvaluationJoanna Jaira SalcedoNo ratings yet
- Ncp-retdem Torio Grp6Document6 pagesNcp-retdem Torio Grp6pinkgirljojiNo ratings yet
- Nursing Care Plan - BeDocument6 pagesNursing Care Plan - BeMart UrsuNo ratings yet
- NCP Deficit Fluid VolumeDocument4 pagesNCP Deficit Fluid VolumeKingJayson Pacman06No ratings yet
- Dysfunctional Gastrointestinal Motility Maybe Related To Sedentary Lifestyle and Limited Water Intake As Evidenced byDocument6 pagesDysfunctional Gastrointestinal Motility Maybe Related To Sedentary Lifestyle and Limited Water Intake As Evidenced byCecil MonteroNo ratings yet
- NCP CushingDocument4 pagesNCP CushingKatherine BautistaNo ratings yet
- Nursing Care Plan #1 for Fluid Volume DeficitDocument1 pageNursing Care Plan #1 for Fluid Volume DeficitJohn Martelino EnriquezNo ratings yet
- Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goal: IndependentDocument2 pagesNursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goal: IndependentEva Marielle CezaldoNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanJobelyn TunayNo ratings yet
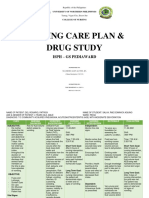
- Salva, R.D NCP & Drug Study (Isph - Gs Pediaward)Document7 pagesSalva, R.D NCP & Drug Study (Isph - Gs Pediaward)Rae Dominick Aquino SalvaNo ratings yet
- NCP For CholecystitisDocument9 pagesNCP For Cholecystitisjmravago220% (1)
- Fluid Volume Deficient Cues SDocument6 pagesFluid Volume Deficient Cues SjedrickNo ratings yet
- Prio NCP NG Dka ByeDocument5 pagesPrio NCP NG Dka ByeMARIA HILARY TABLANTENo ratings yet
- Nursing Care for Amoebiasis: Assessment, Diagnosis, Planning, Intervention & EvaluationDocument9 pagesNursing Care for Amoebiasis: Assessment, Diagnosis, Planning, Intervention & EvaluationRobin HaliliNo ratings yet
- Nursing Care Plan: Subjective: Fluid Volume Deficit IndependentDocument2 pagesNursing Care Plan: Subjective: Fluid Volume Deficit IndependentJade GordoncilloNo ratings yet
- Nursing Care Plan: Subjective: Fluid Volume Deficit IndependentDocument2 pagesNursing Care Plan: Subjective: Fluid Volume Deficit IndependentJade GordoncilloNo ratings yet
- FNCPDocument2 pagesFNCPMrRightNo ratings yet
- Adolescent NCPDocument1 pageAdolescent NCPClaire DobleNo ratings yet
- made.FEU Institute of Nursing Care Plan: Fluid Volume DeficitDocument8 pagesmade.FEU Institute of Nursing Care Plan: Fluid Volume Deficitelaine_tengco50% (2)
- Nursing Interventions for Fluid Volume DeficitDocument2 pagesNursing Interventions for Fluid Volume Deficitdeadgrave16No ratings yet
- Nursing Care Plan Cues Nursing Diagnosis Goal Nursing Interventions Rationale EvaluationDocument2 pagesNursing Care Plan Cues Nursing Diagnosis Goal Nursing Interventions Rationale EvaluationRainier Rhett ConchaNo ratings yet
- Subjective:: Assessment Nursing Diagnosis Planning Interventi ONS Rationale EvaluationDocument2 pagesSubjective:: Assessment Nursing Diagnosis Planning Interventi ONS Rationale EvaluationCuttie Anne GalangNo ratings yet
- NCP Deficient Fluid VolumeDocument1 pageNCP Deficient Fluid VolumeMatth N. ErejerNo ratings yet
- The Development of a Model of Human Nature that reflects Patient Presentation in General PracticeFrom EverandThe Development of a Model of Human Nature that reflects Patient Presentation in General PracticeNo ratings yet
- Polarity Therapy: How Re-Polarizing Your Body Can Heal YouFrom EverandPolarity Therapy: How Re-Polarizing Your Body Can Heal YouRating: 1 out of 5 stars1/5 (1)
- An Epitome of the Homeopathic Healing Art: Containing the New Discoveries and Improvements to the Present TimeFrom EverandAn Epitome of the Homeopathic Healing Art: Containing the New Discoveries and Improvements to the Present TimeNo ratings yet
- Head NursingDocument5 pagesHead NursingBern NerquitNo ratings yet
- ND2 Initial Output PBL-4Document9 pagesND2 Initial Output PBL-4Bern NerquitNo ratings yet
- 119 Concept PaperDocument4 pages119 Concept PaperBern NerquitNo ratings yet
- PBL 8 Rle 2 - NerquitDocument19 pagesPBL 8 Rle 2 - NerquitBern NerquitNo ratings yet
- SRP Breastfeeding Awareness Group 2 NDDocument39 pagesSRP Breastfeeding Awareness Group 2 NDBern NerquitNo ratings yet
- KARDEXDocument2 pagesKARDEXBern NerquitNo ratings yet
- Chapter 6 - Nursing Care For The Family in Need of Reproductive Life PlanningDocument7 pagesChapter 6 - Nursing Care For The Family in Need of Reproductive Life PlanningBern NerquitNo ratings yet
- Chapter 8 - Nursing Care of The Family Having Difficulty Conceiving A ChildDocument9 pagesChapter 8 - Nursing Care of The Family Having Difficulty Conceiving A ChildBern NerquitNo ratings yet
- Pbl6 Group3 SurnameDocument17 pagesPbl6 Group3 SurnameBern NerquitNo ratings yet
- 6.3 Functions of Nursing JurisprudenceDocument1 page6.3 Functions of Nursing JurisprudenceBern NerquitNo ratings yet
- Gallery Walk PosterDocument1 pageGallery Walk PosterBern NerquitNo ratings yet
- 3f g2 Simulation Video On Leadership TrainingDocument1 page3f g2 Simulation Video On Leadership TrainingBern NerquitNo ratings yet
- NCM 118 and 119 All Notes For ProcessingDocument38 pagesNCM 118 and 119 All Notes For ProcessingBern NerquitNo ratings yet
- Nursing Care of A Family When A Child Has A Neurologic DisorderDocument8 pagesNursing Care of A Family When A Child Has A Neurologic DisorderBern NerquitNo ratings yet
- A.1 Admission & DischargeDocument27 pagesA.1 Admission & DischargeBern NerquitNo ratings yet
- NUTRIENTS - Vitamins and MineralsDocument142 pagesNUTRIENTS - Vitamins and MineralsBern NerquitNo ratings yet
- SpiritualityDocument2 pagesSpiritualityBern NerquitNo ratings yet
- Tracheostomy CareDocument6 pagesTracheostomy CareBern NerquitNo ratings yet
- Laboratory Activity #5 Soft and Mechanical DietDocument3 pagesLaboratory Activity #5 Soft and Mechanical DietBern NerquitNo ratings yet
- Introduction To Diet TherapyDocument42 pagesIntroduction To Diet TherapyBern NerquitNo ratings yet
- Nutrition Care Process: Problem: Diagnostic Label (Term and Code) Etiology: Related Factors Contributing ToDocument1 pageNutrition Care Process: Problem: Diagnostic Label (Term and Code) Etiology: Related Factors Contributing ToBern NerquitNo ratings yet
- Pain: The 5 Vital SignDocument2 pagesPain: The 5 Vital SignBern NerquitNo ratings yet
- Nerquit - Opening and Closing Sterile PacksDocument1 pageNerquit - Opening and Closing Sterile PacksBern NerquitNo ratings yet
- DocumentationDocument3 pagesDocumentationBern NerquitNo ratings yet
- Heat and Cold ApplicationDocument5 pagesHeat and Cold ApplicationBern NerquitNo ratings yet
- Nutritional StatusDocument5 pagesNutritional StatusBern Nerquit100% (1)
- Calculation On Diet and Meal PlanningDocument5 pagesCalculation On Diet and Meal PlanningBern NerquitNo ratings yet
- Legal Aspects of NursingDocument3 pagesLegal Aspects of NursingBern NerquitNo ratings yet
- Heat and Cold ApplicationDocument5 pagesHeat and Cold ApplicationBern NerquitNo ratings yet
- EXPAREL Prescribing InformationDocument17 pagesEXPAREL Prescribing InformationcignalNo ratings yet
- Brush Up On Your Drug Calculation SkillsDocument12 pagesBrush Up On Your Drug Calculation SkillsMichael Baylon DueñasNo ratings yet
- Chapter 41 - Thoracic Outlet Syndrome SynonymsDocument8 pagesChapter 41 - Thoracic Outlet Syndrome SynonymsPiero Massafra100% (1)
- MULTIPLE ORGAN DYSFUNCTIONDocument16 pagesMULTIPLE ORGAN DYSFUNCTIONrefika rahmiNo ratings yet
- Stretching - Inservice - Final Eddie PizzoDocument18 pagesStretching - Inservice - Final Eddie PizzoMatthew PuglieseNo ratings yet
- Acute Liver Disease: Causes and Types of Acute Hepatitis (38 charactersDocument22 pagesAcute Liver Disease: Causes and Types of Acute Hepatitis (38 characterszakria100100No ratings yet
- 11.EVALUATION OF ANTIBACTERIAL AND ANTIFUNGAL ACTIVITY OF ALOE VERA GEL CH.V.S Gautam, M. Rekha, P. Mourya, S. Sukanya, Habeeba UnissaDocument6 pages11.EVALUATION OF ANTIBACTERIAL AND ANTIFUNGAL ACTIVITY OF ALOE VERA GEL CH.V.S Gautam, M. Rekha, P. Mourya, S. Sukanya, Habeeba UnissaBaru Chandrasekhar RaoNo ratings yet
- Psychoanalytic & Cognitive Child Development Theories - Freud, Erikson, PiagetDocument2 pagesPsychoanalytic & Cognitive Child Development Theories - Freud, Erikson, PiagetRomelyn AngadolNo ratings yet
- ETP Assessment Refreshment PDFDocument21 pagesETP Assessment Refreshment PDFFindora InternusaNo ratings yet
- Manila Adventist College: REFERENCE For Your Answers. Best If You Will Use Your Book ReferenceDocument6 pagesManila Adventist College: REFERENCE For Your Answers. Best If You Will Use Your Book Referencedia diaNo ratings yet
- Unit 11 Arterial PunctureDocument34 pagesUnit 11 Arterial PunctureZoe Rodriguez100% (1)
- 1.dr. Hingki - Noso Role in PPRA HIPPI PIT 050419 PDFDocument47 pages1.dr. Hingki - Noso Role in PPRA HIPPI PIT 050419 PDFPrimawatiNo ratings yet
- Bene Ts of Using Fluorescence Induced Theragnosis in Fixed Orthodontic Therapy: Status, Technology and Future TrendsDocument7 pagesBene Ts of Using Fluorescence Induced Theragnosis in Fixed Orthodontic Therapy: Status, Technology and Future TrendsTiagoNo ratings yet
- AHA Guidelines For CPR and ECC Comparison Chart of Key Changes (2010)Document8 pagesAHA Guidelines For CPR and ECC Comparison Chart of Key Changes (2010)PhilippineNursingDirectory.comNo ratings yet
- C 5 ProteinDocument20 pagesC 5 ProteinChristina HalderNo ratings yet
- Lower Eyelid Entropion Repair ReferencesDocument2 pagesLower Eyelid Entropion Repair ReferencesSherly WahyuniNo ratings yet
- Initial Assessment of Emergency Department PatientsDocument11 pagesInitial Assessment of Emergency Department PatientsDen Sinyo0% (1)
- Physiotherapy in Shoulder Impigement SyndromeDocument181 pagesPhysiotherapy in Shoulder Impigement SyndromePraneeth KumarNo ratings yet
- Depression Article LancetDocument13 pagesDepression Article LancetDjamil DamryNo ratings yet
- TMBU Cleaning and Disinfection Policy 2012Document10 pagesTMBU Cleaning and Disinfection Policy 2012ver_at_workNo ratings yet
- The DASH Diet PlanDocument50 pagesThe DASH Diet PlanNiar Marhali67% (3)
- Nebulizer Therapy A Platform For Pulmonary Drug Delivery (1 7)Document7 pagesNebulizer Therapy A Platform For Pulmonary Drug Delivery (1 7)Talha Go SindalleNo ratings yet
- Cytomegalovirus Infection and Disease in The New Era of Immunosuppression Following Solid Organ TransplantationDocument9 pagesCytomegalovirus Infection and Disease in The New Era of Immunosuppression Following Solid Organ TransplantationReza Firmansyah IINo ratings yet
- PP Dokter Setia Putra Tarigan MASSIVE PLEURAL EFFUSIONS BPLS Maret 2015Document19 pagesPP Dokter Setia Putra Tarigan MASSIVE PLEURAL EFFUSIONS BPLS Maret 2015zhafran ritongaNo ratings yet
- AntidepressantsDocument4 pagesAntidepressantsSalman HabeebNo ratings yet
- Pediatric Case 2: Jackson Weber (Complex) : Guided Reflection QuestionsDocument4 pagesPediatric Case 2: Jackson Weber (Complex) : Guided Reflection QuestionsJacqueline LamNo ratings yet
- U.S. Equal Employment Opportunity Commission v. Norfolk Southern Corp.Document33 pagesU.S. Equal Employment Opportunity Commission v. Norfolk Southern Corp.Ryan CaneNo ratings yet
- Gateway B2+ Test Unit 3 BDocument5 pagesGateway B2+ Test Unit 3 Bana maria csalinas67% (3)
- Intro to Fixed Partial DenturesDocument5 pagesIntro to Fixed Partial DenturesThesdave SinghNo ratings yet
- Records and Reports DocumentationDocument18 pagesRecords and Reports DocumentationJomarNo ratings yet