You might also like
- What's New in Oxygen Therapy?: EditorialDocument3 pagesWhat's New in Oxygen Therapy?: EditorialmilleralselmoNo ratings yet
- Oxygen in The ICU Too Much of A Good Thing?: EditorialDocument2 pagesOxygen in The ICU Too Much of A Good Thing?: Editorialdella psNo ratings yet
- Seteo de Oxigenoterapia en El HospitalDocument5 pagesSeteo de Oxigenoterapia en El HospitalSofia SoharNo ratings yet
- Oxygenation Target in Acute Respiratory Distress Syndrome, 2023Document8 pagesOxygenation Target in Acute Respiratory Distress Syndrome, 2023Jonathan Fierro MedinaNo ratings yet
- Acute Life-Threatening Hypoxemia During Mechanical VentilationDocument8 pagesAcute Life-Threatening Hypoxemia During Mechanical VentilationCesar Rivas CamposNo ratings yet
- Central Venous CO2 Gap Guides ResuscitationDocument8 pagesCentral Venous CO2 Gap Guides Resuscitationrodolfo riosNo ratings yet
- E006812 FullDocument8 pagesE006812 FullabhiNo ratings yet
- Oxygen Saturation Targets in Critical Care - LITFL - CCCDocument30 pagesOxygen Saturation Targets in Critical Care - LITFL - CCCnonieshzNo ratings yet
- s13054 020 03409 0Document13 pagess13054 020 03409 0Sidik SyafaatullahNo ratings yet
- HFCN IgdDocument6 pagesHFCN IgdayuniNo ratings yet
- Metas de Oxigeno 2021Document11 pagesMetas de Oxigeno 2021Javier López CastellanosNo ratings yet
- ARBR 2806 Edit ReportDocument5 pagesARBR 2806 Edit ReportJosé Manuel Valencia GallardoNo ratings yet
- High Flow Nasal Cannula For Acute Respiratory Distress Syndrome Due To Covid 19Document5 pagesHigh Flow Nasal Cannula For Acute Respiratory Distress Syndrome Due To Covid 19Cesar C SNo ratings yet
- Use of High-Flow Nasal Cannula Oxygen Therapy To Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate HypoxemiaDocument10 pagesUse of High-Flow Nasal Cannula Oxygen Therapy To Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate HypoxemiaLingga AniNo ratings yet
- Review ArticleDocument9 pagesReview ArticleAyu SuwarayuNo ratings yet
- Nebulized Dexmedetomidine-Lidocaine Inhalation As A Premedication For Flexible Bronchoscopy: A Randomized TrialDocument8 pagesNebulized Dexmedetomidine-Lidocaine Inhalation As A Premedication For Flexible Bronchoscopy: A Randomized TrialRichard PhoNo ratings yet
- Year in Review 2019: High-Flow Nasal Cannula Oxygen Therapy For Adult SubjectsDocument13 pagesYear in Review 2019: High-Flow Nasal Cannula Oxygen Therapy For Adult SubjectsRicardoNo ratings yet
- Erxiang Gao, Chi Zhang, Jianping Wang : Research ArticleDocument8 pagesErxiang Gao, Chi Zhang, Jianping Wang : Research ArticleZuhairatul khairaNo ratings yet
- Metrics of Arterial Hyperoxia and Associated Outcomes in Critical CareDocument9 pagesMetrics of Arterial Hyperoxia and Associated Outcomes in Critical CarehdNo ratings yet
- Prone Ventilation in Acute Respiratory Distress SyndromeDocument10 pagesProne Ventilation in Acute Respiratory Distress Syndromecelma44No ratings yet
- Outcomes of COPDDocument6 pagesOutcomes of COPDRISKINo ratings yet
- The Liberal Use of Oxygen Is It JustifiedDocument3 pagesThe Liberal Use of Oxygen Is It Justifiedipe.jacobNo ratings yet
- Effectiveness of High-Flow Nasal Cannula Oxygen Therapy For Acute Respiratory Failure With HypercapniaDocument7 pagesEffectiveness of High-Flow Nasal Cannula Oxygen Therapy For Acute Respiratory Failure With Hypercapniarahma_husna_1No ratings yet
- Jurnal Dari Aak 4Document8 pagesJurnal Dari Aak 4rifqi rizalNo ratings yet
- Adhf 3Document8 pagesAdhf 3dindasaviraNo ratings yet
- Prolonged Prone Position Ventilation For Sars-Cov-2 Patients Is Feasible and EffectiveDocument3 pagesProlonged Prone Position Ventilation For Sars-Cov-2 Patients Is Feasible and Effectivecarlos_julianNo ratings yet
- 10 1111@resp 13469Document10 pages10 1111@resp 13469César Avila JimenezNo ratings yet
- 393fb8d1f65033129998006911894128Document15 pages393fb8d1f65033129998006911894128archivelalaaNo ratings yet
- Adult Oxygen Therapy GuidelinesDocument29 pagesAdult Oxygen Therapy Guidelinesjembut300100% (2)
- Predictors of Intubation in COVID-19 Patients Treated With out-of-ICU Continuous Positive Airway PressureDocument8 pagesPredictors of Intubation in COVID-19 Patients Treated With out-of-ICU Continuous Positive Airway PressureLucatntNo ratings yet
- Control of Respiratory Drive by Extracorporeal CO Removal in Acute Exacerbation of COPD Breathing On Non-Invasive NAVADocument9 pagesControl of Respiratory Drive by Extracorporeal CO Removal in Acute Exacerbation of COPD Breathing On Non-Invasive NAVAMileth GonzalezNo ratings yet
- Near Infrared Spectroscopy For Assessing OxygenDocument6 pagesNear Infrared Spectroscopy For Assessing OxygenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Oxigenoterapia Parte 2 Indicaciones y ToxicidadDocument9 pagesOxigenoterapia Parte 2 Indicaciones y ToxicidadyeseyeseprimisNo ratings yet
- Aarc 2002Document10 pagesAarc 2002Yolanda ShintaNo ratings yet
- Brochardrespmonitconsof 16 CC 2012Document15 pagesBrochardrespmonitconsof 16 CC 2012Leandro VillamilNo ratings yet
- International ImmunopharmacologyDocument6 pagesInternational ImmunopharmacologyMarvin Huanca MartinezNo ratings yet
- Guia OxigenoterapiaDocument10 pagesGuia OxigenoterapiaJonathan AlvaradoNo ratings yet
- Review ArticleDocument8 pagesReview Articledella psNo ratings yet
- Jurnal AnestesiDocument6 pagesJurnal AnestesiMarest AskynaNo ratings yet
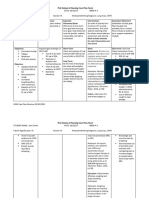
- Nursing Care PlanDocument4 pagesNursing Care PlannamitaNo ratings yet
- Young2022 Article OxygenTargetsDocument4 pagesYoung2022 Article OxygenTargetsBrenda Serrano LaraNo ratings yet
- Oxygen Therapy GuidelinesDocument19 pagesOxygen Therapy GuidelinesAyuna Rahmani0% (1)
- Redefining ARDS: A Paradigm Shift: Perspective Open AccessDocument7 pagesRedefining ARDS: A Paradigm Shift: Perspective Open Accesseyobhabtamu3No ratings yet
- Proning in Non-Intubated (PINI) in Times of COVID-19: Case Series and A ReviewDocument7 pagesProning in Non-Intubated (PINI) in Times of COVID-19: Case Series and A ReviewCarlos ZepedaNo ratings yet
- Clinical Profile and Outcome of Covid-19 Patients With Requirement of Oxygen Therapy For Greater Than One WeekDocument3 pagesClinical Profile and Outcome of Covid-19 Patients With Requirement of Oxygen Therapy For Greater Than One WeekIJAR JOURNALNo ratings yet
- Medi 101 E29940Document5 pagesMedi 101 E29940Bella FebriantiNo ratings yet
- JCM 07 00205Document8 pagesJCM 07 00205IzzyNo ratings yet
- COPD Patients Effectively Treated with BiPAP through Endotracheal TubeDocument5 pagesCOPD Patients Effectively Treated with BiPAP through Endotracheal TubeMayco BiasibettiNo ratings yet
- (2020) Oxygen-Ozone (O2-O3) Immunoceutical Therapy For Patients With COVID-19 Preliminary Evidence ReportedDocument5 pages(2020) Oxygen-Ozone (O2-O3) Immunoceutical Therapy For Patients With COVID-19 Preliminary Evidence ReportedVu TranNo ratings yet
- (PULMO) 2012 ARDS - The New Berlin DefinitionDocument4 pages(PULMO) 2012 ARDS - The New Berlin DefinitionerikaNo ratings yet
- Helmet CPAP Vs HFNC Clinical TrialDocument19 pagesHelmet CPAP Vs HFNC Clinical TrialTaufik RiansyahNo ratings yet
- Ventilación en SDRA - Guia ClinicaDocument18 pagesVentilación en SDRA - Guia ClinicaPablo PradoNo ratings yet
- SLED Vs CRRT PDFDocument9 pagesSLED Vs CRRT PDFquilino2012No ratings yet
- ARDS Patients Exhibiting A "Hyperinflammatory Anasarca" Phenotype Could Benefit From A Conservative Fluid Management StrategyDocument7 pagesARDS Patients Exhibiting A "Hyperinflammatory Anasarca" Phenotype Could Benefit From A Conservative Fluid Management StrategyPIR BanjarmasinNo ratings yet
- Postresuscitation ManagementDocument8 pagesPostresuscitation ManagementGabriela PachecoNo ratings yet
- Effects of Fluid Balance On Prognosis of Acute Respiratory Distress Syndrome Patients Secondary To SepsisDocument7 pagesEffects of Fluid Balance On Prognosis of Acute Respiratory Distress Syndrome Patients Secondary To SepsisPIR BanjarmasinNo ratings yet
- Early HyperoxiaDocument7 pagesEarly HyperoxiacarloshgmedeirosNo ratings yet
- Can We Reduce The Risk of Readmission For A Patient With An Exacerbation of COPDDocument3 pagesCan We Reduce The Risk of Readmission For A Patient With An Exacerbation of COPDtsiko111No ratings yet
- Implementation of A Non-Invasive Oxygenation Support Strategy During The COVID-19 Pandemic in An Ephemeral Respiratory Intermediate Care UnitDocument3 pagesImplementation of A Non-Invasive Oxygenation Support Strategy During The COVID-19 Pandemic in An Ephemeral Respiratory Intermediate Care UnitJHNo ratings yet
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
- Data, Big Data, and Metadata in AnesthesiologyDocument7 pagesData, Big Data, and Metadata in AnesthesiologySoumya DasNo ratings yet
- Ontario - Schedule of Benefits 2021Document970 pagesOntario - Schedule of Benefits 2021Raj LoganathanNo ratings yet
- Dr. Fernando P. Solidum, Petitioner, vs. People of The PhilippinesDocument2 pagesDr. Fernando P. Solidum, Petitioner, vs. People of The PhilippinesMarites regaliaNo ratings yet
- Devesh Mahajan ResumeDocument5 pagesDevesh Mahajan Resumejobs shahiNo ratings yet
- Anestesi RecordDocument1 pageAnestesi RecordWelmi Sulfatri IshakNo ratings yet
- ICU Criteria DuringDocument5 pagesICU Criteria DuringBaebee LouNo ratings yet
- List of Nationally Authorised Medicinal Products: Active Substance: Nimesulide (Systemic Formulations)Document7 pagesList of Nationally Authorised Medicinal Products: Active Substance: Nimesulide (Systemic Formulations)mcamilaarredondovelezNo ratings yet
- 2020 Dnb AnesthesiaDocument33 pages2020 Dnb AnesthesiasreesaichowdaryNo ratings yet
- Hipotension 6Document16 pagesHipotension 6arturo castilloNo ratings yet
- Anesthesia History Calendar PDFDocument91 pagesAnesthesia History Calendar PDFgoogle playNo ratings yet
- Baska MaskDocument8 pagesBaska MaskAnish H DaveNo ratings yet
- Job DescriptionsDocument139 pagesJob DescriptionsAbdullah Bin SaeedNo ratings yet
- Emergency Neurological Life Support: Airway, Ventilation, and SedationDocument50 pagesEmergency Neurological Life Support: Airway, Ventilation, and SedationastrianamaulidianiNo ratings yet
- NP 5Document16 pagesNP 5Tudlasan Kimmy100% (2)
- Situation 2Document8 pagesSituation 2Rodessa Mandac TarolNo ratings yet
- Key Points: Balanced Anesthesia in Small Animal Patients: Incorporating Cri'SDocument2 pagesKey Points: Balanced Anesthesia in Small Animal Patients: Incorporating Cri'SAlejandro Estrada RiosNo ratings yet
- List of Display Able Medical Qualifications (Jul 2010)Document11 pagesList of Display Able Medical Qualifications (Jul 2010)drvarun81No ratings yet
- Anaesthesia AS GuideDocument3 pagesAnaesthesia AS GuidethetNo ratings yet
- Final Anaesthesia QuestionsDocument23 pagesFinal Anaesthesia QuestionsRancesh FamoNo ratings yet
- Resep KapsulDocument6 pagesResep KapsulMas AwangNo ratings yet
- 81 FullDocument2 pages81 FullANGELICANo ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Surgical Safety Checklist PoliciesDocument3 pagesSurgical Safety Checklist PoliciesOHHC ORNo ratings yet
- Extubation After Difficult IntubationDocument3 pagesExtubation After Difficult Intubationramanrajesh83No ratings yet
- Joint statement on out-of-hours anaesthesia activityDocument4 pagesJoint statement on out-of-hours anaesthesia activityJane KoNo ratings yet
- Clinical Management For Patients Admitted To A Critical Care Unit With Severe Sepsis or Septic ShockDocument7 pagesClinical Management For Patients Admitted To A Critical Care Unit With Severe Sepsis or Septic ShockrizkaNo ratings yet
- Scientific TeamDocument4 pagesScientific TeampriyadikkalaNo ratings yet
- Planning and Management of Anesthesia DepartmentDocument20 pagesPlanning and Management of Anesthesia Departmentlokitoka zigNo ratings yet
- 1-Anesthetic Assesment & PremedicationDocument77 pages1-Anesthetic Assesment & PremedicationAnanth SusruthNo ratings yet
- Spinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDocument5 pagesSpinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDella Puspita SariNo ratings yet