You might also like
- n597 Psychiatric Soap Note 2Document7 pagesn597 Psychiatric Soap Note 2api-532870494No ratings yet
- Occupational Noise Exposure and Hypertension: A Case-Control StudyDocument7 pagesOccupational Noise Exposure and Hypertension: A Case-Control StudycrsscribdNo ratings yet
- Cardiovascular Risks Associated With Incident and Prevalent Periodontal DiseaseDocument8 pagesCardiovascular Risks Associated With Incident and Prevalent Periodontal DiseaseAlyaefkageNo ratings yet
- Association of Occupational Noise Exposure Bilateral Hearing Loss WithDocument6 pagesAssociation of Occupational Noise Exposure Bilateral Hearing Loss WithKaty Marlen GongoraNo ratings yet
- Ehp.1002640 PDFDocument6 pagesEhp.1002640 PDFFeiky HerfandiNo ratings yet
- Preventive Medicine 118 (2019) 73-80Document8 pagesPreventive Medicine 118 (2019) 73-80helioNo ratings yet
- Pulpal Inflammation and Incidence of Coronary Heart Disease Joshipura 2006Document5 pagesPulpal Inflammation and Incidence of Coronary Heart Disease Joshipura 2006Jing XueNo ratings yet
- Brachial Artery Responses to Pollution and Weather in DiabeticsDocument8 pagesBrachial Artery Responses to Pollution and Weather in DiabeticsRivaldo RuffNo ratings yet
- Celis-Morales 2018Document14 pagesCelis-Morales 2018allyssa rahmadittaNo ratings yet
- Research: Exposure To Greenness and Mortality in A Nationwide Prospective Cohort Study of WomenDocument9 pagesResearch: Exposure To Greenness and Mortality in A Nationwide Prospective Cohort Study of WomenmanuelNo ratings yet
- Ehp 1206136Document7 pagesEhp 1206136SaiKai54No ratings yet
- Disparities in Periodontitis Prevalence Among Chronic Kidney Disease PatientsDocument5 pagesDisparities in Periodontitis Prevalence Among Chronic Kidney Disease PatientsKristelle HernandezNo ratings yet
- Heart Rate Variability in Association With Frequent Use of Household Sprays and Scented Products in SAPALDIADocument8 pagesHeart Rate Variability in Association With Frequent Use of Household Sprays and Scented Products in SAPALDIAMayeNo ratings yet
- Kulick Et Al 2020-Long-Term Exposure To Ambient Air PollutionDocument10 pagesKulick Et Al 2020-Long-Term Exposure To Ambient Air PollutionJulius DewaldNo ratings yet
- Long Term Survival After On Pump Coronary Artery Bypass GR 2023 Aging and HeDocument4 pagesLong Term Survival After On Pump Coronary Artery Bypass GR 2023 Aging and Hebz52dk7jvdNo ratings yet
- 10 1002@msc 1498Document13 pages10 1002@msc 1498Ricardo PietrobonNo ratings yet
- Ahl N DepressionDocument7 pagesAhl N DepressionDr Pavina RayamajhiNo ratings yet
- Hearing Problems in Indonesia Attention To Hypertensive AdultsDocument11 pagesHearing Problems in Indonesia Attention To Hypertensive AdultsAdinda Raihana SitorusNo ratings yet
- Decreased Reaction Time Variability Is Associated With Greater Cardiovascular Responses To Acute StressDocument10 pagesDecreased Reaction Time Variability Is Associated With Greater Cardiovascular Responses To Acute StressFitra AlfaniNo ratings yet
- Cardio Metabolic Risk in Individuals Prescribed Long Acting - 2019 - PsychiatryDocument7 pagesCardio Metabolic Risk in Individuals Prescribed Long Acting - 2019 - PsychiatryBelen MatteNo ratings yet
- 2017 Article 4050Document7 pages2017 Article 4050Liramesti LiramestiNo ratings yet
- A Comparison of Effects of Systemic and Intratympanic Steroid Therapies For Sudden Sensorineural Hearing Loss: A Meta-AnalysisDocument6 pagesA Comparison of Effects of Systemic and Intratympanic Steroid Therapies For Sudden Sensorineural Hearing Loss: A Meta-AnalysisIndahEkaPutriNo ratings yet
- Periodontitis Predicts Elevated C-Reactive Protein Levels in Chronic Kidney DiseaseDocument5 pagesPeriodontitis Predicts Elevated C-Reactive Protein Levels in Chronic Kidney DiseaseKristelle HernandezNo ratings yet
- Hearing LossDocument12 pagesHearing LossFirdha Aulia NisaNo ratings yet
- Hammer Et Al 2013 Environmental Noise Pollution in The United States Developing An Effective Public Health ResponseDocument5 pagesHammer Et Al 2013 Environmental Noise Pollution in The United States Developing An Effective Public Health Responsesara.gallegomNo ratings yet
- Commentary: Environmental Noise Pollution in The United States: Developing An Effective Public Health ResponseDocument5 pagesCommentary: Environmental Noise Pollution in The United States: Developing An Effective Public Health ResponseEdwin HansNo ratings yet
- Archives of Psychiatric NursingDocument4 pagesArchives of Psychiatric NursingRizky MhmmdNo ratings yet
- Smart Watch Screening For A FibDocument19 pagesSmart Watch Screening For A FibRuth CaldwellNo ratings yet
- Measuring Severity of Tinnitus With A Visual Analog ScaleDocument4 pagesMeasuring Severity of Tinnitus With A Visual Analog ScaleCamiloNo ratings yet
- 3 Impact of Diurnal Temperature Range On Human HealthDocument15 pages3 Impact of Diurnal Temperature Range On Human HealthBruno OliveiraNo ratings yet
- Vibrotactile Device Applied To The External Ear 2019Document11 pagesVibrotactile Device Applied To The External Ear 2019Alexya CavalcantiNo ratings yet
- Out 44Document12 pagesOut 44misscindy123rNo ratings yet
- 2016 Article 662Document8 pages2016 Article 662terminallllNo ratings yet
- Prediction Models For The Diagnosis of AsthmaDocument11 pagesPrediction Models For The Diagnosis of AsthmaIJRASETPublicationsNo ratings yet
- 2.study On Relationship Between Self-Recognition of Voice Disorder and Mental Health Status Korea National Health and Nutrition Examination SurveyDocument5 pages2.study On Relationship Between Self-Recognition of Voice Disorder and Mental Health Status Korea National Health and Nutrition Examination SurveyKENSIL TAIZ CORDOVA SANCHEZNo ratings yet
- Effects of Prolonged Unemployment and Reemployment On Psychological and Physical HealthDocument8 pagesEffects of Prolonged Unemployment and Reemployment On Psychological and Physical HealthpetrucciNo ratings yet
- CONICET Digital Nro. DDocument37 pagesCONICET Digital Nro. DGabriel GonzálezNo ratings yet
- A Prospective Study of Cardiovascular Risk Factors and Incident Hearing Loss in Men LaryngoscopeDocument5 pagesA Prospective Study of Cardiovascular Risk Factors and Incident Hearing Loss in Men LaryngoscopeGirish SubashNo ratings yet
- Journal of Affective DisordersDocument5 pagesJournal of Affective DisordersdrilaydacayNo ratings yet
- Abu Ruz 2015Document10 pagesAbu Ruz 2015Aini HiolaNo ratings yet
- Stress MortalitiyDocument11 pagesStress Mortalitiyerik gunawanNo ratings yet
- Age Differences in Associations Between Psychological Distress and Chronic ConditionsDocument10 pagesAge Differences in Associations Between Psychological Distress and Chronic ConditionsChristine HandayaniNo ratings yet
- Journal of Affective Disorders Volume 142 Issue 2012 (Doi 10.1016/s0165-0327 (12) 70004-6) Roy, Tapash Lloyd, Cathy E. - Epidemiology of Depression and Diabetes - A Systematic ReviewDocument14 pagesJournal of Affective Disorders Volume 142 Issue 2012 (Doi 10.1016/s0165-0327 (12) 70004-6) Roy, Tapash Lloyd, Cathy E. - Epidemiology of Depression and Diabetes - A Systematic ReviewSinta Rahmah SariNo ratings yet
- Sample Paraphrase Introd AbstractDocument4 pagesSample Paraphrase Introd AbstractAdyl SultanNo ratings yet
- Wildfire ExposureDocument35 pagesWildfire ExposureMichelleNo ratings yet
- Birkefeld (2022)Document14 pagesBirkefeld (2022)Nerea AlvarezNo ratings yet
- Follow-Up Shows No Adverse Outcomes of CNEP in Neonates: LancetDocument1 pageFollow-Up Shows No Adverse Outcomes of CNEP in Neonates: LancetajuliocNo ratings yet
- The Problem and It'S Background: World Health OrganizationDocument26 pagesThe Problem and It'S Background: World Health OrganizationGio LlanosNo ratings yet
- Air Pollution and Mental Health Evidence From ChinaDocument54 pagesAir Pollution and Mental Health Evidence From ChinaNadiah IskandarNo ratings yet
- Article SidesDocument7 pagesArticle SidesAmadou GueyeNo ratings yet
- 1 s2.0 S0167527316326055 MainDocument5 pages1 s2.0 S0167527316326055 Mainparvez.anika91No ratings yet
- Out 3Document6 pagesOut 3Ilvita MayasariNo ratings yet
- ADHD Medications and Risk of Serious Cardiovascular Events in Young and Middle-Aged AdultsDocument11 pagesADHD Medications and Risk of Serious Cardiovascular Events in Young and Middle-Aged AdultsGary KatzNo ratings yet
- Jurnal KL - 1476-069x-8-38Document10 pagesJurnal KL - 1476-069x-8-38Vera FebriaNo ratings yet
- Hansford 2021Document12 pagesHansford 2021Acilino PortelaNo ratings yet
- Abstract: Objective: To Verify The Relationship Between Systemic ArterialDocument10 pagesAbstract: Objective: To Verify The Relationship Between Systemic Arterialprofesor conanNo ratings yet
- Clarifying Dementia Risk Factors: Treading in Murky Waters: CommentaryDocument3 pagesClarifying Dementia Risk Factors: Treading in Murky Waters: CommentaryVazia Rahma HandikaNo ratings yet
- Copd JournalDocument8 pagesCopd JournalKeanuNo ratings yet
- Cardiovascular Effects of Environmental Noise: Research in SwedenDocument7 pagesCardiovascular Effects of Environmental Noise: Research in SwedenAakash PawarNo ratings yet
- Neuroscience and Biobehavioral ReviewsDocument18 pagesNeuroscience and Biobehavioral ReviewsFaris AdrianNo ratings yet
- Telemedicine and Asthma: An innovative approach to improve morbidity and mortality rates for active adults.: Effects of Telemedicine in Asthma care for remote and inner-city underserved populations.From EverandTelemedicine and Asthma: An innovative approach to improve morbidity and mortality rates for active adults.: Effects of Telemedicine in Asthma care for remote and inner-city underserved populations.No ratings yet
- HSE Dashboard V4.1-1Document3 pagesHSE Dashboard V4.1-1Ioana UrsanNo ratings yet
- Bf Cmt Silic ShowDocument15 pagesBf Cmt Silic ShowIoana UrsanNo ratings yet
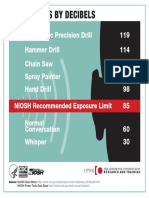
- 7 Noise Level by Decibles PDFDocument1 page7 Noise Level by Decibles PDFIoana UrsanNo ratings yet
- Welding FumesDocument1 pageWelding FumesIoana UrsanNo ratings yet
- Identifying Workplace Safety HazardsDocument5 pagesIdentifying Workplace Safety HazardsIoana UrsanNo ratings yet
- Information Sheet: Crystalline Silica DustDocument2 pagesInformation Sheet: Crystalline Silica DustIoana UrsanNo ratings yet
- Information Sheet: Crystalline Silica DustDocument2 pagesInformation Sheet: Crystalline Silica DustIoana UrsanNo ratings yet
- Risk Assessment EbookDocument13 pagesRisk Assessment EbookIoana UrsanNo ratings yet
- Traffic SafetyDocument2 pagesTraffic SafetyIoana UrsanNo ratings yet
- Ansell Comfort Whitepaper 2017-04-28 FDDocument8 pagesAnsell Comfort Whitepaper 2017-04-28 FDIoana UrsanNo ratings yet
- Materials Handling Drywall CPWRDocument2 pagesMaterials Handling Drywall CPWRIoana UrsanNo ratings yet
- 21 Preventing Falls Through Holes CPWRDocument2 pages21 Preventing Falls Through Holes CPWRIoana UrsanNo ratings yet
- SHP 2017 Health Compliance FinalDocument29 pagesSHP 2017 Health Compliance FinalIoana UrsanNo ratings yet
- Abstract TemplateDocument2 pagesAbstract TemplateIoana UrsanNo ratings yet
- HWC 2018 19 en Campaign GuideDocument36 pagesHWC 2018 19 en Campaign GuideIoana UrsanNo ratings yet
- Structure Diagnostic Pre-Test Section 2 LongmanDocument6 pagesStructure Diagnostic Pre-Test Section 2 LongmandanypamNo ratings yet
- Wessel 1984. The Agricultural Foundations of CivilizationDocument4 pagesWessel 1984. The Agricultural Foundations of CivilizationAndres Maria-ramirezNo ratings yet
- 4 Nutrition in InfancyDocument92 pages4 Nutrition in InfancyramszlaiNo ratings yet
- Scenario in EnglishDocument4 pagesScenario in Englishithanur316No ratings yet
- OPTHA 2.3 OPTIC NERVE - Dr. FerminDocument4 pagesOPTHA 2.3 OPTIC NERVE - Dr. FerminPatricia ManaliliNo ratings yet
- Guidelines IucnDocument24 pagesGuidelines IucnOjasvi SharmaNo ratings yet
- C+F-Overview of Supraventriculer Tachycardia in Dogs and CatsDocument11 pagesC+F-Overview of Supraventriculer Tachycardia in Dogs and Catstaner_soysurenNo ratings yet
- Morg Comm Clin Adv 0310Document1 pageMorg Comm Clin Adv 0310Virginia Savely DNPNo ratings yet
- Ulcerative Vs Chrons DseDocument25 pagesUlcerative Vs Chrons DseDan AmiscuaNo ratings yet
- Gramatica EnglezaDocument4 pagesGramatica EnglezaLore DanaNo ratings yet
- Neel Sharma (Author) - SBAs and EMQs in Paediatrics For Medical Students (2010, CRC Press) (10.1201 - b20735) - Libgen - LiDocument132 pagesNeel Sharma (Author) - SBAs and EMQs in Paediatrics For Medical Students (2010, CRC Press) (10.1201 - b20735) - Libgen - LiDANIEL SIMASIKUNo ratings yet
- Dermatology Slides - Introduction To Clinical DermatologyDocument34 pagesDermatology Slides - Introduction To Clinical DermatologyAzry Mustapa100% (1)
- Neuro-pharmacological and analgesic effects of Arnica montana extractDocument4 pagesNeuro-pharmacological and analgesic effects of Arnica montana extractCristina Elena NicuNo ratings yet
- Bandaging: by C Kohn, Waterford, WIDocument17 pagesBandaging: by C Kohn, Waterford, WISurya AdhikariNo ratings yet
- Material Safety Data Sheet Date of Preparation: 2/11/11 6393000Document2 pagesMaterial Safety Data Sheet Date of Preparation: 2/11/11 6393000sebaversaNo ratings yet
- Marshall Community Letter: Person at Middle School Tests Positive For CoronavirusDocument1 pageMarshall Community Letter: Person at Middle School Tests Positive For CoronavirusJoy M. HosfordNo ratings yet
- Importance of Mycotoxin's Analysis inDocument36 pagesImportance of Mycotoxin's Analysis inusaeswotiNo ratings yet
- Death Row GrannyDocument8 pagesDeath Row Grannyapi-719543705No ratings yet
- Managing hospitals during public health emergenciesDocument25 pagesManaging hospitals during public health emergenciesRahma YunitaNo ratings yet
- Research Article TMJ and Hearing LossDocument8 pagesResearch Article TMJ and Hearing LossMusthafa Afif WardhanaNo ratings yet
- Apha Pharmacy-Based: Module 1. Pharmacists, Vaccines, and Public HealthDocument18 pagesApha Pharmacy-Based: Module 1. Pharmacists, Vaccines, and Public HealthbobNo ratings yet
- African EveDocument230 pagesAfrican EveIstván Sárándi100% (1)
- Hhis Obe MidtermDocument5 pagesHhis Obe MidtermHANNAH DARLED BALIADNo ratings yet
- Welcome To The Family Of: Advance Polyclinic & Path CareDocument19 pagesWelcome To The Family Of: Advance Polyclinic & Path Caredipendra kumarNo ratings yet
- Supplements Who Needs Them?: A Behind The Headlines Report June 2011Document34 pagesSupplements Who Needs Them?: A Behind The Headlines Report June 2011Sa AsNo ratings yet
- PKL Geri RevDocument3 pagesPKL Geri RevKurniati NiaNo ratings yet
- Lacquer Thinner Safety Data SheetDocument8 pagesLacquer Thinner Safety Data SheetM.FAIZAN ARSHADNo ratings yet
- Obat antithiroid: New England Medical Journal review of antithyroid drugsDocument52 pagesObat antithiroid: New England Medical Journal review of antithyroid drugsYeyen MusainiNo ratings yet
- Migraine Diaries PDFDocument4 pagesMigraine Diaries PDFDr.Gopinath SaravananNo ratings yet