You might also like
- Public Service Satisfaction Survey ReportDocument25 pagesPublic Service Satisfaction Survey ReportCenter for Urban Research, CUNY100% (1)
- United States Patent Application Publication No .: US 2021/0082583 A1Document53 pagesUnited States Patent Application Publication No .: US 2021/0082583 A1Tim Brown100% (7)
- Effects of Covid 19 Pandemic On International Financial ManagementDocument3 pagesEffects of Covid 19 Pandemic On International Financial ManagementEditor IJTSRDNo ratings yet
- COVID-19 and Smoking: What Evidence Needs Our Attention?Document9 pagesCOVID-19 and Smoking: What Evidence Needs Our Attention?elguyoNo ratings yet
- Covid 19 Dan Rokok PDFDocument7 pagesCovid 19 Dan Rokok PDFkkn tematik uho kendariNo ratings yet
- The Controversial Effect of Smoking and Nicotine in Sars-Cov-2 InfectionDocument29 pagesThe Controversial Effect of Smoking and Nicotine in Sars-Cov-2 Infectionemmanuel AndemNo ratings yet
- National Smoking Rates Correlate Inversely With COVID-19 MortalityDocument17 pagesNational Smoking Rates Correlate Inversely With COVID-19 MortalityCipiwon DaisukiNo ratings yet
- 14Document12 pages14Marcela MahechaNo ratings yet
- Vaksin Influenza COVID MortalityDocument17 pagesVaksin Influenza COVID MortalityAndi SusiloNo ratings yet
- Reflections On Passive Smoking and COVID-19: Point of ViewDocument4 pagesReflections On Passive Smoking and COVID-19: Point of ViewCibelly CorreiaNo ratings yet
- Smoking - SARS - CoV - 2 andDocument11 pagesSmoking - SARS - CoV - 2 andJeremiah Tanjuakio MarasiganNo ratings yet
- Pi Is 0196655320306374Document9 pagesPi Is 0196655320306374Akhmad HidayatNo ratings yet
- Journal of Medical Virology - 2020 - Reddy - The Effect of Smoking On COVID 19 Severity A Systematic Review andDocument12 pagesJournal of Medical Virology - 2020 - Reddy - The Effect of Smoking On COVID 19 Severity A Systematic Review andAisah AisahNo ratings yet
- Reduce Your Risk of Serious Lung Disease Caused by Corona Virus by Quitting Smoking and Vaping - Center For Tobacco Control Research and EducationDocument13 pagesReduce Your Risk of Serious Lung Disease Caused by Corona Virus by Quitting Smoking and Vaping - Center For Tobacco Control Research and EducationJesse DanzigNo ratings yet
- Obesity Chronic Disease Age and in - Hospital Mortality in Patients With Covid-19 - Analysis of ISARIC Clinical Characterisation Protocol UK CohortDocument9 pagesObesity Chronic Disease Age and in - Hospital Mortality in Patients With Covid-19 - Analysis of ISARIC Clinical Characterisation Protocol UK CohortJesusNo ratings yet
- Similar COVID-19 Incidence To The General Population in People With Opioid Use Disorder Receiving Integrated Outpatient Clinical CareDocument21 pagesSimilar COVID-19 Incidence To The General Population in People With Opioid Use Disorder Receiving Integrated Outpatient Clinical CareCamilo Andrés CastroNo ratings yet
- COVID - Risk of Hospitaization IF-1.6Document20 pagesCOVID - Risk of Hospitaization IF-1.6Manal Haj HamadNo ratings yet
- Research ProposalDocument13 pagesResearch Proposalmehak fatimaNo ratings yet
- S Moking and COVID-19: Is There A S Moker's Paradox in COVID-19?Document6 pagesS Moking and COVID-19: Is There A S Moker's Paradox in COVID-19?Kervy Jay AgraviadorNo ratings yet
- Association of Procalcitonin Levels With The Progression and Prognosis of Hospitalized Patients With COVID-19Document9 pagesAssociation of Procalcitonin Levels With The Progression and Prognosis of Hospitalized Patients With COVID-19Dian Putri NingsihNo ratings yet
- Covid 19Document9 pagesCovid 19abuumaiyoNo ratings yet
- Tuberculosis and COVID-19 Interaction - A Review of BiolDocument15 pagesTuberculosis and COVID-19 Interaction - A Review of BiolMatvey SprindzukNo ratings yet
- Meta Analysis 043 Niageng DzakiyahDocument12 pagesMeta Analysis 043 Niageng Dzakiyahniageng wardaniNo ratings yet
- Association of COVID 19 With Diabetes: A Systematic Review and Meta AnalysisDocument8 pagesAssociation of COVID 19 With Diabetes: A Systematic Review and Meta AnalysisAgatha GeraldyneNo ratings yet
- Impact of Covid-19Document8 pagesImpact of Covid-19melkyNo ratings yet
- COVID-19 Economic Impact Payments and Opioid Overdose DeathsDocument6 pagesCOVID-19 Economic Impact Payments and Opioid Overdose DeathsMatt ThomasNo ratings yet
- Biomarkers of Ageing and Frailty May Predict COVID-19 SeverityDocument13 pagesBiomarkers of Ageing and Frailty May Predict COVID-19 SeverityPPDS Rehab Medik UnhasNo ratings yet
- 1 s2.0 S0033062022001384 MainDocument28 pages1 s2.0 S0033062022001384 MainAnnisa MulyaniNo ratings yet
- Jurnal Bahan ReveiwDocument11 pagesJurnal Bahan ReveiwmnoorallthetimeNo ratings yet
- Diabetes Metabolism Res - 2020 - Zhou - Obesity and Diabetes As High Risk Factors For Severe Coronavirus Disease 2019Document14 pagesDiabetes Metabolism Res - 2020 - Zhou - Obesity and Diabetes As High Risk Factors For Severe Coronavirus Disease 2019syifa yustianaNo ratings yet
- BidirectionalDocument12 pagesBidirectionalLSGNo ratings yet
- TC1 Response To A Live Employer Brief Employer Brief: Student Name: Student Code: Submission DateDocument16 pagesTC1 Response To A Live Employer Brief Employer Brief: Student Name: Student Code: Submission Datesyeda maryemNo ratings yet
- Hypertension and Its Severity or Mortality in Coronavirus Disease 2019 (COVID-19) : A Pooled AnalysisDocument22 pagesHypertension and Its Severity or Mortality in Coronavirus Disease 2019 (COVID-19) : A Pooled AnalysisAnis FaradhinaNo ratings yet
- Adaptation and Evaluation of Turkish Version of The Fear of COVID 19 ScaleDocument10 pagesAdaptation and Evaluation of Turkish Version of The Fear of COVID 19 ScaleGiiszs AlvarezNo ratings yet
- Public Policy Lessons From The Covid 19 Outbreak: How To Deal With It in The Post Pandemic World?Document14 pagesPublic Policy Lessons From The Covid 19 Outbreak: How To Deal With It in The Post Pandemic World?MeemNo ratings yet
- The Impact of The COVID-19 Pandemic On Suicide Rates: Leo SherDocument6 pagesThe Impact of The COVID-19 Pandemic On Suicide Rates: Leo SherLuciusMessiasNo ratings yet
- Case Control - Angga AdnyanaDocument9 pagesCase Control - Angga AdnyanaLalu FarosNo ratings yet
- 6.hypertension in Patients With CoronavirusDocument6 pages6.hypertension in Patients With Coronavirusmary samaniegoNo ratings yet
- HIV and COVID 19 Comorbidity Current EviDocument7 pagesHIV and COVID 19 Comorbidity Current EviM.ALDI RIZALDINo ratings yet
- The Relationship Between Age Groups and Knowledge and Understanding of Covid-19 VaccineDocument5 pagesThe Relationship Between Age Groups and Knowledge and Understanding of Covid-19 VaccineIJAR JOURNALNo ratings yet
- Bijaya Nanda Naik Et Al - Tobacco Use Pattern and Quitting Behaviour Among Healthcare Professionals - India - PDFDocument8 pagesBijaya Nanda Naik Et Al - Tobacco Use Pattern and Quitting Behaviour Among Healthcare Professionals - India - PDFNicolae-Sorin DrăganNo ratings yet
- The Effects of COVID 19 Pandemic Outbreak On Food Consumption Preferences and Their Causes-With-Cover-Page-V2Document6 pagesThe Effects of COVID 19 Pandemic Outbreak On Food Consumption Preferences and Their Causes-With-Cover-Page-V2Jecel LazarraNo ratings yet
- Risk For Newly Diagnosed Diabetes After COVID-19: A Systematic Review and Meta-AnalysisDocument10 pagesRisk For Newly Diagnosed Diabetes After COVID-19: A Systematic Review and Meta-AnalysisDarshan GandhiNo ratings yet
- Diabetes Epidemiology in The COVID-19 Pandemic: Elizabeth Selvin and Stephen P. JuraschekDocument5 pagesDiabetes Epidemiology in The COVID-19 Pandemic: Elizabeth Selvin and Stephen P. JuraschekやたなあはあやたNo ratings yet
- Hesitation and Refusal Factors in Individuals' Decision-Making Processes Regarding A Coronavirus Disease 2019 VaccinationDocument14 pagesHesitation and Refusal Factors in Individuals' Decision-Making Processes Regarding A Coronavirus Disease 2019 VaccinationFachry RahmanNo ratings yet
- Social Science & Medicine: Bethany Griffin, Mark Conner, Paul NormanDocument8 pagesSocial Science & Medicine: Bethany Griffin, Mark Conner, Paul NormanMónika MikeNo ratings yet
- SUD and CovidDocument10 pagesSUD and CovidGadisa DejeneNo ratings yet
- Organization, W.H. (2020) - Smoking and COVID-19: Scientific Brief. (Online) JSTOR. Available AtDocument3 pagesOrganization, W.H. (2020) - Smoking and COVID-19: Scientific Brief. (Online) JSTOR. Available AtlilianabouibrahimNo ratings yet
- Multi Level Drivers Of Tobacco Use And Purchasing Behaviors During Covid 19 Lockdownz A Qualitative Study In The United States Daniel P Giovenco Torra E Spillane Rachel M Maggi Esth download 2024 full chapterDocument24 pagesMulti Level Drivers Of Tobacco Use And Purchasing Behaviors During Covid 19 Lockdownz A Qualitative Study In The United States Daniel P Giovenco Torra E Spillane Rachel M Maggi Esth download 2024 full chaptergary.wesley812100% (9)
- DocumentDocument2 pagesDocumentJoshua GrantNo ratings yet
- Vaccine 2021Document17 pagesVaccine 2021cdsaludNo ratings yet
- Understanding COVID-19 Misinformation and Vaccine Hesitancy in Context - Findings From A Qualitative Study Involving Citizens in Bradford, UKDocument10 pagesUnderstanding COVID-19 Misinformation and Vaccine Hesitancy in Context - Findings From A Qualitative Study Involving Citizens in Bradford, UKMYNo ratings yet
- Inequalities in The Impact of COVID-19-associated Disruptions On Tuberculosis Diagnosis by Age and Sex in 45 High TB Burden CountriesDocument9 pagesInequalities in The Impact of COVID-19-associated Disruptions On Tuberculosis Diagnosis by Age and Sex in 45 High TB Burden CountriesDarshan GandhiNo ratings yet
- Articles: BackgroundDocument10 pagesArticles: BackgroundmitahafsahNo ratings yet
- 3rd R.LDocument14 pages3rd R.LWilliam Tac anNo ratings yet
- Factors Associated With COVID-19 Vaccine HesitancyDocument14 pagesFactors Associated With COVID-19 Vaccine HesitancyksmidhilaNo ratings yet
- TB COVID Global Cohort ERJ 2022Document16 pagesTB COVID Global Cohort ERJ 2022The SangeNo ratings yet
- News Events and Their Relationship With US Vape SaDocument9 pagesNews Events and Their Relationship With US Vape SaRobby RanidoNo ratings yet
- Addictive Behaviors in The COVID-19 Era: Ceva Despre Efectele Izolarii SocialeDocument10 pagesAddictive Behaviors in The COVID-19 Era: Ceva Despre Efectele Izolarii SocialeAdriana OlaruNo ratings yet
- 2 Addictive Behaviors DuringDocument10 pages2 Addictive Behaviors DuringAdriana OlaruNo ratings yet
- DepressionDocument3 pagesDepressionemilpauloquibilanNo ratings yet
- Demystifying COVID-19: Understanding the Disease, Its Diagnosis. and TreatmentFrom EverandDemystifying COVID-19: Understanding the Disease, Its Diagnosis. and TreatmentNo ratings yet
- PMG MediaMeter Services and Rates PDFDocument2 pagesPMG MediaMeter Services and Rates PDFNicolae-Sorin DrăganNo ratings yet
- Umberto Ecoand Semiotic CreativityDocument6 pagesUmberto Ecoand Semiotic CreativityNicolae-Sorin DrăganNo ratings yet
- Petrilli and Ponzio - About StorytellingDocument18 pagesPetrilli and Ponzio - About StorytellingNicolae-Sorin DrăganNo ratings yet
- Van Westen-Lagerweij Et Al - Are Smoker Protected Against SAR-COV2 - PDFDocument3 pagesVan Westen-Lagerweij Et Al - Are Smoker Protected Against SAR-COV2 - PDFNicolae-Sorin DrăganNo ratings yet
- Motivations Toward Smoking Cessation - PDFDocument12 pagesMotivations Toward Smoking Cessation - PDFNicolae-Sorin DrăganNo ratings yet
- TCS Report 2021 Interactive V4Document36 pagesTCS Report 2021 Interactive V4Nicolae-Sorin DrăganNo ratings yet
- COVID-19 and Your Eye CareDocument4 pagesCOVID-19 and Your Eye CareZyla PaulineNo ratings yet
- HM 212 - Seatwork No. 1 (Abesia, Diana Mae)Document4 pagesHM 212 - Seatwork No. 1 (Abesia, Diana Mae)Diana AbesiaNo ratings yet
- Research Paper Chapter 1 3Document34 pagesResearch Paper Chapter 1 3Lyca jean PascuaNo ratings yet
- Civil Aviation Authority of Bangladesh: WWW - Caab.gov - BDDocument2 pagesCivil Aviation Authority of Bangladesh: WWW - Caab.gov - BDRisdiyanto Edy Saputro100% (1)
- HDFC UW Guidelines For Term Plan - ALL Channels Consolidated - JuneDocument35 pagesHDFC UW Guidelines For Term Plan - ALL Channels Consolidated - Junesandeep pimpalgaonkarNo ratings yet
- Special Entry Darshan (Rs.300) : Tirumala Tirupati DevasthanamsDocument1 pageSpecial Entry Darshan (Rs.300) : Tirumala Tirupati DevasthanamsSivakumarNo ratings yet
- Return To Work Coordinator Course NSWDocument7 pagesReturn To Work Coordinator Course NSWd0t1f1wujap3100% (2)
- MG625 - Leading and Managing ChanageDocument40 pagesMG625 - Leading and Managing ChanageDilaNo ratings yet
- Topdara Stupa: Libraries LockdownsDocument3 pagesTopdara Stupa: Libraries LockdownsMbongeniNo ratings yet
- Report of The Coalition For Equality and Other NGOSDocument22 pagesReport of The Coalition For Equality and Other NGOSOSGFNo ratings yet
- Feature WritingDocument2 pagesFeature WritingRoselle PangilinanNo ratings yet
- A Case AnalysisDocument3 pagesA Case AnalysisPaulo Gabriel Loquinario100% (1)
- Coronavirus Flow Chart Response Plan (Vessel - Site)Document2 pagesCoronavirus Flow Chart Response Plan (Vessel - Site)HSE PULAI ANo ratings yet
- China Healthcare Report - FinalDocument87 pagesChina Healthcare Report - FinalRishabh RajNo ratings yet
- Tiktok, Identity Struggles and Mental Health Issues: How Are The Youth of Today Coping?Document6 pagesTiktok, Identity Struggles and Mental Health Issues: How Are The Youth of Today Coping?Trúc NgânNo ratings yet
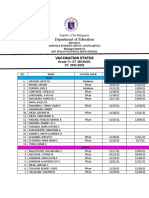
- Department of Education: Vaccination StatusDocument2 pagesDepartment of Education: Vaccination StatusKristelle BigawNo ratings yet
- HSE Bulletin # 84: Break The Chain of Corona Virus Transmission Stay Safe & Stay at HomeDocument1 pageHSE Bulletin # 84: Break The Chain of Corona Virus Transmission Stay Safe & Stay at HomeAbdus SamadNo ratings yet
- Extended Off Ace Conserve Covid Unit Outside RoomDocument1 pageExtended Off Ace Conserve Covid Unit Outside RoomJoselito P. PlatillaNo ratings yet
- Office: Directors FOR Health OF Health Region Directors Medical Treatment RehabilitationDocument4 pagesOffice: Directors FOR Health OF Health Region Directors Medical Treatment RehabilitationDiwata OndeNo ratings yet
- COVID-19 Community Quarantines in The PhilippinesDocument7 pagesCOVID-19 Community Quarantines in The PhilippinesBhosx KimNo ratings yet
- DM Editorials Magazine 12th April 2020Document177 pagesDM Editorials Magazine 12th April 2020joy burnNo ratings yet
- The Luxury IndustryDocument8 pagesThe Luxury IndustryShreeyaNo ratings yet
- Fascism EssayDocument8 pagesFascism EssayfatehbirsinghbrarNo ratings yet
- Essay Covid 19Document1 pageEssay Covid 19Jessabel AusaNo ratings yet
- Risk in Sports and Challenges For Sports OrganizationsDocument210 pagesRisk in Sports and Challenges For Sports OrganizationsHoa ThúyNo ratings yet
- Dogus Otomotiv FR - 2020 - EN - WEB-REVDocument72 pagesDogus Otomotiv FR - 2020 - EN - WEB-REVElif KeskinNo ratings yet
- DELOITTE DI CIO CIO Insider Maximizing The Impact of Tech Investments in The New NormalDocument20 pagesDELOITTE DI CIO CIO Insider Maximizing The Impact of Tech Investments in The New NormalLuis Paulo Senra HuberNo ratings yet