You might also like
- Preliminary Findings of The Minimally-Invasive Surgery Plus Rtpa For Intracerebral Hemorrhage Evacuation (Mistie) Clinical TrialDocument5 pagesPreliminary Findings of The Minimally-Invasive Surgery Plus Rtpa For Intracerebral Hemorrhage Evacuation (Mistie) Clinical TrialOmer AhmedNo ratings yet
- HIM6Document2 pagesHIM6Romeo GuevaraNo ratings yet
- ASH CaplacizumabDocument4 pagesASH CaplacizumabMagdalena Górska-KosickaNo ratings yet
- UntitledDocument4 pagesUntitledMohammad HamidNo ratings yet
- 1 s2.0 S0741521496702665 MainDocument7 pages1 s2.0 S0741521496702665 MainMau MillanNo ratings yet
- Erasu 2020Document1 pageErasu 2020jerryNo ratings yet
- Use of Tranexamic Acid To Reduce Blood Loss in Liposuction: Rio de Janeiro, Brazil Newark, N.J. and New York, N.YDocument4 pagesUse of Tranexamic Acid To Reduce Blood Loss in Liposuction: Rio de Janeiro, Brazil Newark, N.J. and New York, N.YVictor Andre PeraltaNo ratings yet
- In-Stent Restenosis After Carotid Angioplasty-Stenting: Incidence and ManagementDocument7 pagesIn-Stent Restenosis After Carotid Angioplasty-Stenting: Incidence and ManagementRicardo Novoa AlvarezNo ratings yet
- 2020middle Meningeal Artery Embolization For Chronic Subdural HematomaDocument5 pages2020middle Meningeal Artery Embolization For Chronic Subdural HematomaJulio Cesar Velasco CastroNo ratings yet
- Journal Club TemplateDocument5 pagesJournal Club TemplateAnonymous zyHbTsybDXNo ratings yet
- Acute Promyelocytic LeukemiaDocument46 pagesAcute Promyelocytic LeukemiaKartthik ShanmugamNo ratings yet
- Abstract 4Document7 pagesAbstract 4Sead RizvanovićNo ratings yet
- Tranexamic Acid Use in Prehospital Uncontrolled HeDocument11 pagesTranexamic Acid Use in Prehospital Uncontrolled Hechou youNo ratings yet
- Measurement of Troponin T To Detect Cardioprotective Effect of Trimetazidine During Coronary Artery Bypass GraftingDocument4 pagesMeasurement of Troponin T To Detect Cardioprotective Effect of Trimetazidine During Coronary Artery Bypass GraftingSabri AbyNo ratings yet
- GP I PCIDocument7 pagesGP I PCISofija VukadinovićNo ratings yet
- Onodera 2012Document4 pagesOnodera 2012jerryNo ratings yet
- Seizure Txa 1Document9 pagesSeizure Txa 1PeriUmardianaNo ratings yet
- Doppler Atlas SonothrombolysisDocument4 pagesDoppler Atlas SonothrombolysisdanielNo ratings yet
- Early and Late Results of Total Correction of Tetralogy of FallotDocument6 pagesEarly and Late Results of Total Correction of Tetralogy of FallotResiden KardiologiNo ratings yet
- Wu2017 PDFDocument6 pagesWu2017 PDFPavel SebastianNo ratings yet
- The Efficacy and Safety of Tranexamic Acid Treatment in Orthopaedic Trauma Surgery.Document8 pagesThe Efficacy and Safety of Tranexamic Acid Treatment in Orthopaedic Trauma Surgery.GabrielNo ratings yet
- Gliomas PosterDocument2 pagesGliomas PosterAnil Kumar ReddyNo ratings yet
- Acido Tranexamico 2Document7 pagesAcido Tranexamico 2Paola SanchezNo ratings yet
- Tranexamico en TraumaDocument6 pagesTranexamico en TraumaAdrian CroesNo ratings yet
- 00000164-jth 12878 PDFDocument5 pages00000164-jth 12878 PDFfachrizal zaleNo ratings yet
- 681 FullDocument6 pages681 FullKurnia AnharNo ratings yet
- Efectos de La Administración Temprana de Ácido Tranexámico en La Mortalidad, Histerectomías y Otras MorbilidadesDocument4 pagesEfectos de La Administración Temprana de Ácido Tranexámico en La Mortalidad, Histerectomías y Otras MorbilidadesDamiolis Cabrera AmézquitaNo ratings yet
- Tranexamic Acid RCTDocument10 pagesTranexamic Acid RCTIan HuangNo ratings yet
- Tenecteplase For The Treatment of Acute Ischemic Stroke: A Review of Completed and Ongoing Randomized Controlled TrialsDocument8 pagesTenecteplase For The Treatment of Acute Ischemic Stroke: A Review of Completed and Ongoing Randomized Controlled TrialsyoggihermawanNo ratings yet
- Smith AXERDocument2 pagesSmith AXERDian NovitasariNo ratings yet
- Journal ClubDocument12 pagesJournal ClubMohammad NomanNo ratings yet
- Tsutsumi 1997Document6 pagesTsutsumi 1997Ahmad AlzawahrehNo ratings yet
- Bacaan PPT RebleedingDocument61 pagesBacaan PPT RebleedingseliNo ratings yet
- JURNAL READING - Asam TranexamatDocument45 pagesJURNAL READING - Asam TranexamatNurul fajriyatiNo ratings yet
- Garvey 2013Document6 pagesGarvey 2013Lavonia Berlina AdzalikaNo ratings yet
- Advances 017699Document9 pagesAdvances 017699Danang Bagus UntoroNo ratings yet
- 961 FullDocument5 pages961 FullWilliyoNo ratings yet
- CRASH-3 - Tranexamic Acid For The Treatment of Significant Traumatic Brain Injury: Study Protocol For An International Randomized, Double-Blind, Placebo-Controlled TrialDocument14 pagesCRASH-3 - Tranexamic Acid For The Treatment of Significant Traumatic Brain Injury: Study Protocol For An International Randomized, Double-Blind, Placebo-Controlled TrialfrankcoapNo ratings yet
- Management of Colorectal Anastomotic Leakage-Differences Between Salvage and Anastomotic TakedownDocument6 pagesManagement of Colorectal Anastomotic Leakage-Differences Between Salvage and Anastomotic TakedownDumitru RadulescuNo ratings yet
- Surveillance of Fistula Function by Frequent.12Document4 pagesSurveillance of Fistula Function by Frequent.12PatríciaNo ratings yet
- HemorragiaDocument10 pagesHemorragiaCesar ArmentaNo ratings yet
- AedaDocument3 pagesAedaFebey Arie MulyaNo ratings yet
- Pleural Empyema ManagementDocument51 pagesPleural Empyema ManagementredipudyantiNo ratings yet
- 1 s2.0 S0735109797859062 MainDocument2 pages1 s2.0 S0735109797859062 MainJuan David Arenas MendozaNo ratings yet
- 1 s2.0 S0735109797859025 MainDocument1 page1 s2.0 S0735109797859025 MainJuan David Arenas MendozaNo ratings yet
- Kim2012Document5 pagesKim2012Stefanie MelisaNo ratings yet
- Acido TranexamicoDocument8 pagesAcido TranexamicoVianey GarciaVillegasNo ratings yet
- Traumatic Rupture Aortic DX TXDocument6 pagesTraumatic Rupture Aortic DX TXprisselya anisaNo ratings yet
- Iqbal Et Al 2000 State of The Art Review Thrombolytic Drugs in Acute Myocardial InfarctionDocument13 pagesIqbal Et Al 2000 State of The Art Review Thrombolytic Drugs in Acute Myocardial Infarctionparkviewinternending2023No ratings yet
- Miller1991 (Justifica PQ Biopsia A Todos)Document4 pagesMiller1991 (Justifica PQ Biopsia A Todos)ouf81No ratings yet
- Metastatic ChoriocarcinomaDocument6 pagesMetastatic ChoriocarcinomaGeneda Camille SebialNo ratings yet
- Isetta 1993Document2 pagesIsetta 1993Betão AviãoNo ratings yet
- Version of Record:: ManuscriptDocument23 pagesVersion of Record:: Manuscriptmiko balisiNo ratings yet
- 10 1016@j Jmig 2020 08 075Document1 page10 1016@j Jmig 2020 08 075Sedeeq Al-KhazrajiNo ratings yet
- Asma AnsariDocument3 pagesAsma Ansariujjwal souravNo ratings yet
- Pharmacological Management of Acute Coronary Syndromes (ACS) and Acute Limb Ischemia (ALI)Document44 pagesPharmacological Management of Acute Coronary Syndromes (ACS) and Acute Limb Ischemia (ALI)hendratj90No ratings yet
- TR VS Minimamente InvasivaDocument5 pagesTR VS Minimamente Invasivamanuel barrientosNo ratings yet
- American Journal of Emergency Medicine: Yasuaki Mizushima, Shota Nakao, Koji Idoguchi, Tetsuya MatsuokaDocument4 pagesAmerican Journal of Emergency Medicine: Yasuaki Mizushima, Shota Nakao, Koji Idoguchi, Tetsuya MatsuokaRahmania Mutia RifaniNo ratings yet
- AsliDocument10 pagesAsliAngga HanantaNo ratings yet
- Acute Promyelocytic Leukemia: A Clinical GuideFrom EverandAcute Promyelocytic Leukemia: A Clinical GuideOussama AblaNo ratings yet
- ORIFDocument2 pagesORIFDaywalker PedragozaNo ratings yet
- Treatment and Management AppendicitisDocument3 pagesTreatment and Management Appendicitisruthjoy23upgirlNo ratings yet
- Transurethral Resection of The Prostate (TURP)Document16 pagesTransurethral Resection of The Prostate (TURP)Princess Brigitte R. PATE�ANo ratings yet
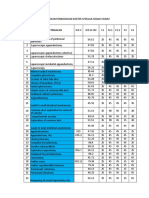
- Cghs Rates BangaloreDocument26 pagesCghs Rates Bangaloregr_viswanathNo ratings yet
- Dapus THTDocument2 pagesDapus THTAgung WahyudiNo ratings yet
- डॉक्टर स्केड्युल (मानव कल्याण केंद्र)Document6 pagesडॉक्टर स्केड्युल (मानव कल्याण केंद्र)Sudeep NikamNo ratings yet
- Pasay - Rle Lab InstrumentsDocument10 pagesPasay - Rle Lab InstrumentsTrishaNo ratings yet
- PCNL Tips and TricksDocument26 pagesPCNL Tips and TricksHafizur RashidNo ratings yet
- Surgical Management of Prolapse CasesDocument13 pagesSurgical Management of Prolapse CasesAlexandriah AlasNo ratings yet
- Open Appendisectomy: - Modul: - Ida Bagus Ananta WijayaDocument34 pagesOpen Appendisectomy: - Modul: - Ida Bagus Ananta WijayarudybisNo ratings yet
- Catalog OPTIKON Pulsar2 Phaco PDFDocument7 pagesCatalog OPTIKON Pulsar2 Phaco PDFAlim Sumon100% (1)
- Approach To Trauma PatientDocument49 pagesApproach To Trauma PatientHadinur Jufri100% (1)
- Bariatric Surgery: 1. Predominantly Malabsorptive ProceduresDocument9 pagesBariatric Surgery: 1. Predominantly Malabsorptive ProceduresmegangstaNo ratings yet
- Supracondylar Humerus FractureDocument13 pagesSupracondylar Humerus FracturedhapitstinNo ratings yet
- History of Hip Arthroplasty: From John R. Barton To John CharnleyDocument8 pagesHistory of Hip Arthroplasty: From John R. Barton To John CharnleyDenis AlexandruNo ratings yet
- BPHDocument38 pagesBPHAnna YulianaNo ratings yet
- What Is CryolipolysisDocument5 pagesWhat Is Cryolipolysisapi-457017927100% (1)
- Subbrow Blepharoplasty For Upper Eyelid Rejuvenation in AsiansDocument5 pagesSubbrow Blepharoplasty For Upper Eyelid Rejuvenation in AsiansdoctorbanNo ratings yet
- List of Videos To Watch On Wise MDDocument1 pageList of Videos To Watch On Wise MDalthrasherNo ratings yet
- Case 1 Case 2: Bladder Outlet ObstructionDocument2 pagesCase 1 Case 2: Bladder Outlet ObstructionHardiTariqHamma100% (1)
- Matsukawa 2017Document33 pagesMatsukawa 2017kanaNo ratings yet
- Prefinal ProgramDocument1 pagePrefinal ProgramHussein AhmedNo ratings yet
- Boaris FlapDocument6 pagesBoaris FlapNihal S KiranNo ratings yet
- Fast DPL CTDocument6 pagesFast DPL CTnmyza89No ratings yet
- NCP Urinary RetentionDocument3 pagesNCP Urinary RetentionKingJayson Pacman06No ratings yet
- Reten Modern Dressing 2023 PKDMTDocument51 pagesReten Modern Dressing 2023 PKDMTMasros TukiranNo ratings yet
- Principles of Fracture FixationDocument12 pagesPrinciples of Fracture FixationApolinar González HernándezNo ratings yet
- 20.daftar Kuantitas Dan Harga Produk Alat Kesehatan 2020 (Ok)Document1 page20.daftar Kuantitas Dan Harga Produk Alat Kesehatan 2020 (Ok)Ifan JayusdianNo ratings yet
- Surgery BoardsDocument16 pagesSurgery Boardscusom34100% (1)
- Penggolongan OperasiDocument32 pagesPenggolongan OperasiKARTIKANo ratings yet