You might also like
- Thyroid Storm Anatomy Physiology Diagnosis TreatmentDocument17 pagesThyroid Storm Anatomy Physiology Diagnosis TreatmentFebriliana Mao-maoNo ratings yet
- A Disease Study of Cushing's DiseaseDocument13 pagesA Disease Study of Cushing's DiseaseKristine AlejandroNo ratings yet
- Anatomy of The Female Pelvis FinalDocument209 pagesAnatomy of The Female Pelvis FinalMignot Aniley86% (14)
- Endocrinology PDFDocument73 pagesEndocrinology PDFRafique C0% (2)
- Etextbook PDF For Principles of Anatomy and Physiology 15th EditionDocument61 pagesEtextbook PDF For Principles of Anatomy and Physiology 15th Editionkarla.woodruff227100% (43)
- Science 10: Self-Learning Module1Document31 pagesScience 10: Self-Learning Module1Mark KevinNo ratings yet
- PHD Thesis in Pancreatic CancerDocument7 pagesPHD Thesis in Pancreatic Cancerzxtccvgld100% (2)
- Galectin CancerDocument6 pagesGalectin CancermaniiiiiiiiNo ratings yet
- 2015 - Raynal Et Al - Targeting Calcium Signaling Induces Epigenetic Reactivation of Tumor Suppressor Genes in CancerDocument13 pages2015 - Raynal Et Al - Targeting Calcium Signaling Induces Epigenetic Reactivation of Tumor Suppressor Genes in Cancermarej312No ratings yet
- 14 AndrusiewiczDocument6 pages14 AndrusiewiczIzmer BhaiNo ratings yet
- Adipokines and Systemic Inflammation in Weight-Losing Lung Cancer PatientsDocument6 pagesAdipokines and Systemic Inflammation in Weight-Losing Lung Cancer PatientsAnna GozaliNo ratings yet
- Cregan. 2016. KAT5 (Tip60) Is A Potential Therapeutic TargetDocument7 pagesCregan. 2016. KAT5 (Tip60) Is A Potential Therapeutic TargetAnonymous lXHxUzdc3No ratings yet
- Jover JC PEGfilgrastimDocument7 pagesJover JC PEGfilgrastimCheli GarciaNo ratings yet
- NLR Marker for Papillary Thyroid MicrocarcinomasDocument6 pagesNLR Marker for Papillary Thyroid MicrocarcinomasagusNo ratings yet
- HUQ2014Document5 pagesHUQ2014MonikaNo ratings yet
- Abstract. Vascular Endothelial Growth Factor (VEGF) Report-: ONCOLOGY LETTERS 5: 1682-1686, 2013Document5 pagesAbstract. Vascular Endothelial Growth Factor (VEGF) Report-: ONCOLOGY LETTERS 5: 1682-1686, 2013yuliaNo ratings yet
- tmpD126 TMPDocument9 pagestmpD126 TMPFrontiersNo ratings yet
- Transplant International Special Issue: Abstracts of The 14th Congress of The European Society For Organ Transplantation Volume 22, Issue Supplement s2, Pages 95-222, August 2009Document128 pagesTransplant International Special Issue: Abstracts of The 14th Congress of The European Society For Organ Transplantation Volume 22, Issue Supplement s2, Pages 95-222, August 2009Enrique Moreno GonzálezNo ratings yet
- Journal Pone 0027074Document7 pagesJournal Pone 0027074AngelaNo ratings yet
- Kim 2005Document5 pagesKim 2005cristina_zaharia865440No ratings yet
- Apigenin Parsley Melanoma PD-1 PD-L1Document15 pagesApigenin Parsley Melanoma PD-1 PD-L1valgurNo ratings yet
- Knockdown of NUPR1 Inhibits The Proliferation of Glioblastoma Cells Via ERK1 - 2, p38 MAPK and Caspase-3Document12 pagesKnockdown of NUPR1 Inhibits The Proliferation of Glioblastoma Cells Via ERK1 - 2, p38 MAPK and Caspase-3郭耿良No ratings yet
- 15-Li Chen (531-538)Document8 pages15-Li Chen (531-538)Nguyễn Thanh TùngNo ratings yet
- PD-L1 Expression in Triple-Negative Breast Cancer: Research ArticleDocument14 pagesPD-L1 Expression in Triple-Negative Breast Cancer: Research ArticleFebrian Parlangga MuisNo ratings yet
- Ni Hms 561057Document19 pagesNi Hms 561057Muhammad Reza IrzantoNo ratings yet
- Neoadjuvant Paclitaxel For Operable Breast Cancer: Multicenter Phase II Trial With Clinical OutcomesDocument6 pagesNeoadjuvant Paclitaxel For Operable Breast Cancer: Multicenter Phase II Trial With Clinical OutcomesSubhash SugathanNo ratings yet
- Thno 54961r2 3Document45 pagesThno 54961r2 3Eduardo JuarezNo ratings yet
- INCLUIDOS-clusianone and Cancer - Search Results - PubMedDocument6 pagesINCLUIDOS-clusianone and Cancer - Search Results - PubMedLidiaAmorimNo ratings yet
- Cisplatin Cell Cicle ArrestDocument7 pagesCisplatin Cell Cicle ArrestGabriele KrauseNo ratings yet
- TILSDocument12 pagesTILSFlaviu Ionuț FaurNo ratings yet
- Clinical Benefit in Patients With Advanced Solid Tumors Treated With Modified Citrus Pectin: A Prospective Pilot StudyDocument8 pagesClinical Benefit in Patients With Advanced Solid Tumors Treated With Modified Citrus Pectin: A Prospective Pilot Studyyafit_armon5854No ratings yet
- Jiang 2019Document5 pagesJiang 2019Ali Halim YILMAZNo ratings yet
- 2010-High-Sensitivoty of C-Reactive Protein and CancerDocument8 pages2010-High-Sensitivoty of C-Reactive Protein and CancerThalia KarampasiNo ratings yet
- Kanker TumorDocument11 pagesKanker TumorRENTI NOVITANo ratings yet
- Fungi & Cancer TherapyDocument18 pagesFungi & Cancer TherapyLynn McdonaldNo ratings yet
- 9 Randomized Phase III Evaluation of Cisplatin PlusDocument6 pages9 Randomized Phase III Evaluation of Cisplatin Plustrifamonika23No ratings yet
- Glypican-3 As A Useful Diagnostic Marker That Distinguishes Hepatocellular Carcinoma From Benign Hepatocellular Mass LesionsDocument6 pagesGlypican-3 As A Useful Diagnostic Marker That Distinguishes Hepatocellular Carcinoma From Benign Hepatocellular Mass LesionsBlake_jjNo ratings yet
- Ol 23 5 13275 PDFDocument9 pagesOl 23 5 13275 PDFSRIBDE STANLEYNo ratings yet
- Phase II Trial of Curcumin in Patients With Advanced Pancreatic Cancer.Document10 pagesPhase II Trial of Curcumin in Patients With Advanced Pancreatic Cancer.João FrancoNo ratings yet
- Feik 2009Document7 pagesFeik 2009JOSE PORTILLONo ratings yet
- Ito 2021Document9 pagesIto 2021wachoNo ratings yet
- tmpD747 TMPDocument16 pagestmpD747 TMPFrontiersNo ratings yet
- Fundamental SciencesDocument23 pagesFundamental SciencesRoxana Alexandra BogosNo ratings yet
- Poster Viewing I Tuesday 1 May 2018 Iii75Document2 pagesPoster Viewing I Tuesday 1 May 2018 Iii75Firdaus Septhy ArdhyanNo ratings yet
- Euromedlab 2013 Abstracts 211 and 219Document103 pagesEuromedlab 2013 Abstracts 211 and 219Jagannadha Rao PeelaNo ratings yet
- Medi 98 E15449Document7 pagesMedi 98 E15449m8f5mwpzwyNo ratings yet
- Nihms 1760542Document19 pagesNihms 1760542Sobek1789No ratings yet
- Or 26 1 185 PDFDocument7 pagesOr 26 1 185 PDFRoland_IINo ratings yet
- Wu 2016Document8 pagesWu 2016Anonymous n2DPWfNuNo ratings yet
- 2848-Article Text-5618-1-10-20221227Document7 pages2848-Article Text-5618-1-10-20221227Mahdi AkbariNo ratings yet
- 10.1007@s00280 016 3133 4Document6 pages10.1007@s00280 016 3133 4Hector MaldonadoNo ratings yet
- Jurnal 1Document11 pagesJurnal 1Dyahsekarayupudak wangiNo ratings yet
- Original Article: High Expression of WDR1 in Primary Glioblastoma Is Associated With Poor PrognosisDocument12 pagesOriginal Article: High Expression of WDR1 in Primary Glioblastoma Is Associated With Poor PrognosisALINo ratings yet
- Wang 2018Document27 pagesWang 2018Raissa RezendeNo ratings yet
- Pharmaceutics 11 00336Document17 pagesPharmaceutics 11 00336Tyas PardedeNo ratings yet
- 1 s2.0 S0360301619310193 MainDocument2 pages1 s2.0 S0360301619310193 MainStem EducationNo ratings yet
- Influence of PEG-conjugated Hemoglobin On Tumor Oxygenation and Response To ChemotherapyDocument12 pagesInfluence of PEG-conjugated Hemoglobin On Tumor Oxygenation and Response To ChemotherapyIstván PortörőNo ratings yet
- 2018 Article 37340Document10 pages2018 Article 37340louisehip UFCNo ratings yet
- Antitumor Effects of Octreotide LAR, A Somatostatin AnalogDocument2 pagesAntitumor Effects of Octreotide LAR, A Somatostatin AnalogVmiguel LcastilloNo ratings yet
- Cox 2Document11 pagesCox 2Agnes WindyasariNo ratings yet
- Chen Et Al 2017Document11 pagesChen Et Al 2017Raul GamiñoNo ratings yet
- Ijms 25 00732Document26 pagesIjms 25 00732Alaa TahaNo ratings yet
- Physiology PharmacologyDocument126 pagesPhysiology PharmacologyuneedlesNo ratings yet
- Cam40002 0234Document9 pagesCam40002 0234Domenico LombardiniNo ratings yet
- Anticancer Activity of Phyllanthus Niruri Linn Extract in Colorectal Cancer Patients A Phase II Clinical TrialDocument5 pagesAnticancer Activity of Phyllanthus Niruri Linn Extract in Colorectal Cancer Patients A Phase II Clinical TrialAndi SaputraNo ratings yet
- AACR 2017 Proceedings: Abstracts 3063-5947From EverandAACR 2017 Proceedings: Abstracts 3063-5947No ratings yet
- Tadevosyan 2021Document26 pagesTadevosyan 2021W Antonio Rivera MartínezNo ratings yet
- Association Between The Finnish Diabetes Risk ScorDocument10 pagesAssociation Between The Finnish Diabetes Risk ScorW Antonio Rivera MartínezNo ratings yet
- Articulo DEF TIAMINA PACIENTE CRITICO PDFDocument6 pagesArticulo DEF TIAMINA PACIENTE CRITICO PDFIvonne D FloresNo ratings yet
- Clinical and Biochemical Response To The Management of Macroprolactinomas in Latin American Men, Cali, Colombia and Habana, CubaDocument12 pagesClinical and Biochemical Response To The Management of Macroprolactinomas in Latin American Men, Cali, Colombia and Habana, CubaW Antonio Rivera MartínezNo ratings yet
- 2020 Jama Chagas UpdateDocument15 pages2020 Jama Chagas UpdateW Antonio Rivera MartínezNo ratings yet
- Artigo 1 - Systemic Lupus ErythematosusDocument12 pagesArtigo 1 - Systemic Lupus ErythematosusKimã Barbosa MeiraNo ratings yet
- Jama Reale 2020 LD 200085 1600712111.15079Document3 pagesJama Reale 2020 LD 200085 1600712111.15079W Antonio Rivera MartínezNo ratings yet
- 2019 Chagas Review PDFDocument32 pages2019 Chagas Review PDFW Antonio Rivera MartínezNo ratings yet
- Biochemical Markers For Clinical Monitoring of Tissue PerfusionDocument14 pagesBiochemical Markers For Clinical Monitoring of Tissue PerfusionTrọng MPNo ratings yet
- Historia Jrsocmed00119 0063Document1 pageHistoria Jrsocmed00119 0063W Antonio Rivera MartínezNo ratings yet
- Comparative Effectiveness of SGLT2 Inhibitors, GLP-1 Receptor Agonists, DPP-4 Inhibitors, and Sulfonylureas On Risk of Kidney Outcomes Emulation of A Target Trial Using Health Care DatabasesDocument11 pagesComparative Effectiveness of SGLT2 Inhibitors, GLP-1 Receptor Agonists, DPP-4 Inhibitors, and Sulfonylureas On Risk of Kidney Outcomes Emulation of A Target Trial Using Health Care DatabasesW Antonio Rivera MartínezNo ratings yet
- We Lko Witz 1991Document6 pagesWe Lko Witz 1991W Antonio Rivera MartínezNo ratings yet
- Openhrt 2021 001719Document8 pagesOpenhrt 2021 001719W Antonio Rivera MartínezNo ratings yet
- 10.1097@HJH.0b013e328332c353 CarmelaDocument11 pages10.1097@HJH.0b013e328332c353 CarmelaW Antonio Rivera MartínezNo ratings yet
- We Lko Witz 1991Document6 pagesWe Lko Witz 1991W Antonio Rivera MartínezNo ratings yet
- Historia Jrsocmed00119 0063Document1 pageHistoria Jrsocmed00119 0063W Antonio Rivera MartínezNo ratings yet
- Openhrt 2021 001719Document8 pagesOpenhrt 2021 001719W Antonio Rivera MartínezNo ratings yet
- Pruebas de Función Pulmonar CecilDocument16 pagesPruebas de Función Pulmonar CecilW Antonio Rivera MartínezNo ratings yet
- 10.1097@HJH.0b013e328332c353 CarmelaDocument11 pages10.1097@HJH.0b013e328332c353 CarmelaW Antonio Rivera MartínezNo ratings yet
- Metformin-Induced Pancreatitis from Renal FailureDocument2 pagesMetformin-Induced Pancreatitis from Renal FailureW Antonio Rivera MartínezNo ratings yet
- Fatal Metformin Overdose Presenting With Progressive HyperglycemiaDocument5 pagesFatal Metformin Overdose Presenting With Progressive HyperglycemiaW Antonio Rivera MartínezNo ratings yet
- UtilityofTPApritotoEVT Neurology2021Document17 pagesUtilityofTPApritotoEVT Neurology2021W Antonio Rivera MartínezNo ratings yet
- Cuocoetal - Neurology For Medical Students (Brainstem Syndromes!)Document14 pagesCuocoetal - Neurology For Medical Students (Brainstem Syndromes!)Crystal AyalaNo ratings yet
- Severe Metformin Intoxication Treated With Prolonged Haemodialyses and Plasma ExchangeDocument3 pagesSevere Metformin Intoxication Treated With Prolonged Haemodialyses and Plasma ExchangeW Antonio Rivera MartínezNo ratings yet
- Pharmacotherapies For COPD: Clinical Medicine Insights: Circulatory, Respiratory and Pulmonary Medicine April 2013Document19 pagesPharmacotherapies For COPD: Clinical Medicine Insights: Circulatory, Respiratory and Pulmonary Medicine April 2013W Antonio Rivera MartínezNo ratings yet
- Brainstem Vascular Syndromes: A Practical Guide For Medical StudentsDocument14 pagesBrainstem Vascular Syndromes: A Practical Guide For Medical StudentsW Antonio Rivera MartínezNo ratings yet
- Parker2014 Interpretación de EspirometríasDocument15 pagesParker2014 Interpretación de EspirometríasW Antonio Rivera MartínezNo ratings yet
- PL Rápida Criterios SuecosDocument8 pagesPL Rápida Criterios SuecosW Antonio Rivera MartínezNo ratings yet
- Infectious Causes of StrokeDocument12 pagesInfectious Causes of StrokeW Antonio Rivera MartínezNo ratings yet
- Menopause Diagnosis and Management PDF 1837330217413Document31 pagesMenopause Diagnosis and Management PDF 1837330217413Mona HelouNo ratings yet
- Pathophysiology of Heart Failure - Neurohumoral Adaptations PDFDocument10 pagesPathophysiology of Heart Failure - Neurohumoral Adaptations PDFcristianamihailaNo ratings yet
- MCQ ThyroidDocument6 pagesMCQ ThyroidFaridOrahaNo ratings yet
- Science 5 2nd Quarter ExamDocument3 pagesScience 5 2nd Quarter ExamLouie Ric FiscoNo ratings yet
- Congenital Hypopituitarism During The Neonatal Period: Epidemiology, Pathogenesis, Therapeutic Options, and OutcomeDocument17 pagesCongenital Hypopituitarism During The Neonatal Period: Epidemiology, Pathogenesis, Therapeutic Options, and OutcomeEsteban LopezNo ratings yet
- Hormonal RegulationDocument20 pagesHormonal Regulationel shilohNo ratings yet
- General Adaptation Syndrome TheoriesDocument4 pagesGeneral Adaptation Syndrome TheoriesHema JothyNo ratings yet
- Product CatalogueDocument20 pagesProduct CatalogueNguyễn Khang KhangNo ratings yet
- Emergency Contaception by James TrussellDocument37 pagesEmergency Contaception by James TrussellAdityaWijayaNo ratings yet
- MCQ PDF 5 PDFDocument3 pagesMCQ PDF 5 PDFshakeelNo ratings yet
- Cushings Vs Addisons in DogsDocument4 pagesCushings Vs Addisons in Dogshenry famNo ratings yet
- A CASE STUDY ON Chronic Renal FailureDocument2 pagesA CASE STUDY ON Chronic Renal FailureJake Yvan DizonNo ratings yet
- Pancreas Structure and FunctionsDocument10 pagesPancreas Structure and FunctionsPunx RamoneNo ratings yet
- (1479683X - European Journal of Endocrinology) European Society of Endocrinology Clinical Practice Guideline: Endocrine Work-Up in ObesityDocument32 pages(1479683X - European Journal of Endocrinology) European Society of Endocrinology Clinical Practice Guideline: Endocrine Work-Up in ObesityAbdiNo ratings yet
- FBA Untuk Obat DMDocument17 pagesFBA Untuk Obat DMKhoirunnisa MuslimawatiNo ratings yet
- (17417899 - Reproduction) Understanding The Regulation of Pituitary Progesterone Receptor Expression and PhosphorylationDocument9 pages(17417899 - Reproduction) Understanding The Regulation of Pituitary Progesterone Receptor Expression and Phosphorylationتقوى اللهNo ratings yet
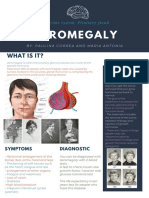
- Acromegaly: What Is It?Document1 pageAcromegaly: What Is It?Paulina CorreaaNo ratings yet
- FIA Meter Plus: Fluorescence Immunoassay Rapid Quantitative TestDocument4 pagesFIA Meter Plus: Fluorescence Immunoassay Rapid Quantitative TestWawan HardjomulionoNo ratings yet
- Reabsorption of SodiumDocument19 pagesReabsorption of Sodiumpriya shettyNo ratings yet
- Early Puberty: How Young Is Too Young?Document3 pagesEarly Puberty: How Young Is Too Young?Ryūō Takeru No MikotoNo ratings yet
- Studi Prevalensi Risiko Diabetes Melitus Pada Remaja Usia 15-20 Tahun Di Kabupaten SidoarjoDocument8 pagesStudi Prevalensi Risiko Diabetes Melitus Pada Remaja Usia 15-20 Tahun Di Kabupaten Sidoarjofardiah tilawatiNo ratings yet
- Endocrine System and Adolescence ChangesDocument22 pagesEndocrine System and Adolescence Changesnia tombriNo ratings yet
- Curs 1 2015 DZDocument44 pagesCurs 1 2015 DZIoana DiaconuNo ratings yet
- Bio 132 Chapter 18 NotesDocument8 pagesBio 132 Chapter 18 Noteslovelyc95100% (1)