You might also like
- Articulo 1 Trastornos MentalesDocument12 pagesArticulo 1 Trastornos MentalesEileen PérezNo ratings yet
- COVID-19-Related Mental Health E Workplace: A Narrative ReviewDocument22 pagesCOVID-19-Related Mental Health E Workplace: A Narrative ReviewDariaNo ratings yet
- Psychological Health and COVID-19Document22 pagesPsychological Health and COVID-19carl jason talanNo ratings yet
- Assignmnet Topic: Psychological and Social Effects of COVID On Health Care WorkersDocument11 pagesAssignmnet Topic: Psychological and Social Effects of COVID On Health Care WorkershassanNo ratings yet
- Chapter 1 FINALDocument5 pagesChapter 1 FINALYoonah FlaminiaNo ratings yet
- Burnout Impact of COVID-19 Pandemic On Health-Care Professionals at Assiut University Hospitals, 2020Document12 pagesBurnout Impact of COVID-19 Pandemic On Health-Care Professionals at Assiut University Hospitals, 2020Ulfa Nur RohmahNo ratings yet
- The Effects of Covid 19 On Healthcare Workers - EditedDocument20 pagesThe Effects of Covid 19 On Healthcare Workers - EditedSepide FarahiNo ratings yet
- The Psychological Impact of COVID-19 On Front Line NursesDocument17 pagesThe Psychological Impact of COVID-19 On Front Line NursesPetar PanNo ratings yet
- APA Research Proposal 2021Document14 pagesAPA Research Proposal 2021med wardNo ratings yet
- Preti Et Al 2020Document22 pagesPreti Et Al 2020Carlos muñozNo ratings yet
- Mental Helath Implications On Covid-19Document6 pagesMental Helath Implications On Covid-19FIRDA SULAINI100% (1)
- Ijerph 18 00861Document10 pagesIjerph 18 00861shameless.No ratings yet
- Editorial: Scand J Work Environ Health Doi:10.5271/sjweh.3893Document3 pagesEditorial: Scand J Work Environ Health Doi:10.5271/sjweh.3893Paúl EnríquezNo ratings yet
- Covid 19 Psychological Effects and Associated Factors in Mexican NursesDocument7 pagesCovid 19 Psychological Effects and Associated Factors in Mexican NursesDelgado Valdez AndrésNo ratings yet
- Innovative Work Shift For Health Workers in The Health Service Providers in Handling COVID-19 CasesDocument6 pagesInnovative Work Shift For Health Workers in The Health Service Providers in Handling COVID-19 CasesDiego Sergio Giasia LumbantobingNo ratings yet
- Mental Health of Nurses During The Fourth Wave of The COVID-19 Pandemic in PolandDocument12 pagesMental Health of Nurses During The Fourth Wave of The COVID-19 Pandemic in PolandLency CahyaningsihNo ratings yet
- Exploring Mental Health Status of Covid-19 Frontliners: A Phenomenological InquiryDocument16 pagesExploring Mental Health Status of Covid-19 Frontliners: A Phenomenological InquiryPsychology and Education: A Multidisciplinary JournalNo ratings yet
- The Fear of COVID-19 Familial Infection ScaleDocument24 pagesThe Fear of COVID-19 Familial Infection ScalefaisalNo ratings yet
- Effects of Covid 19 On Health Care WorkersDocument7 pagesEffects of Covid 19 On Health Care WorkersbaisonjoeNo ratings yet
- UntitledDocument5 pagesUntitledBolanle OlaNo ratings yet
- Fragile Heroes. The Psychological Effect of Covid19Document17 pagesFragile Heroes. The Psychological Effect of Covid19Deanne Morris-DeveauxNo ratings yet
- Emerging of Covid-19 Pandemic Crisis: Its Impact To The Mental Health Among Young and Adult People of Barangay Boniao The Problem and Its BackgroundDocument79 pagesEmerging of Covid-19 Pandemic Crisis: Its Impact To The Mental Health Among Young and Adult People of Barangay Boniao The Problem and Its BackgroundRaymar MacarayanNo ratings yet
- RBMT-850 AE Paragalley ENDocument7 pagesRBMT-850 AE Paragalley ENmiguelNo ratings yet
- Covid-19: Its Impact To The Healthcare Workers' Physical and Mental HealthDocument7 pagesCovid-19: Its Impact To The Healthcare Workers' Physical and Mental HealthJovilyn AjosteNo ratings yet
- The Influence of The Urban EnvDocument14 pagesThe Influence of The Urban EnvAnanya MishraNo ratings yet
- Psychological Intervention and COVID-19 - Final 02042020Document21 pagesPsychological Intervention and COVID-19 - Final 02042020Carolina RojasNo ratings yet
- Background of The StudyDocument15 pagesBackground of The StudyAhra Jhane CarolloNo ratings yet
- AnxietyDocument43 pagesAnxietyام محمد القحطانيNo ratings yet
- Orca Share Media1682588605040 7057288116474940411Document13 pagesOrca Share Media1682588605040 7057288116474940411Yuji itadoriNo ratings yet
- Referensi 47Document7 pagesReferensi 47SaebaNo ratings yet
- Keywords: COVID-19 Pandemic, Fear, Turnover Intentions, Psychological Well-Being, NursingDocument27 pagesKeywords: COVID-19 Pandemic, Fear, Turnover Intentions, Psychological Well-Being, NursingAkhirah MagkilatNo ratings yet
- CovidpsychiatryDocument5 pagesCovidpsychiatryDaniel MacioneNo ratings yet
- Mental Stress post-COVID-19Document8 pagesMental Stress post-COVID-19IJPHSNo ratings yet
- Psychiatry Research: Review ArticleDocument11 pagesPsychiatry Research: Review ArticledominiakzsoltNo ratings yet
- Journal of Psychiatric Research: Yunus Hacimusalar, Aybeniz Civan Kahve, Alisan Burak Yasar, Mehmet Sinan AydinDocument8 pagesJournal of Psychiatric Research: Yunus Hacimusalar, Aybeniz Civan Kahve, Alisan Burak Yasar, Mehmet Sinan AydinAmaury Enrique Frías DotelNo ratings yet
- Aiz ProposalDocument11 pagesAiz ProposalsawadjaanalrazzNo ratings yet
- Oamjms 9t3 330Document5 pagesOamjms 9t3 330Dhilah DhilahhNo ratings yet
- Referensi 52Document19 pagesReferensi 52SaebaNo ratings yet
- 02-Talevi (137-144)Document8 pages02-Talevi (137-144)Rebeca Olmedo AntolínNo ratings yet
- Occupational Stress and Burnout Among Frontline Egyptian Anesthesiologists During COVID 19 Outbreak in EgyptDocument10 pagesOccupational Stress and Burnout Among Frontline Egyptian Anesthesiologists During COVID 19 Outbreak in EgyptReham BINo ratings yet
- The Prevalence and Influencing Factors in Anxiety in Medical Workers Fighting COVID-19 in China: A Cross-Sectional SurveyDocument7 pagesThe Prevalence and Influencing Factors in Anxiety in Medical Workers Fighting COVID-19 in China: A Cross-Sectional SurveyLudwig CaceresNo ratings yet
- Psychological Impact Among Health Workers in Effort To Facing The COVID-19 in IndonesiaDocument8 pagesPsychological Impact Among Health Workers in Effort To Facing The COVID-19 in IndonesiaIJPHSNo ratings yet
- Vanguards of Duty Exploring The Lived Experiences of Healthcare Frontliners During Pandemic SurgeDocument15 pagesVanguards of Duty Exploring The Lived Experiences of Healthcare Frontliners During Pandemic SurgeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Akk Jurnal Internasional 1Document7 pagesAkk Jurnal Internasional 1Onnii SltrNo ratings yet
- China y Covid 2Document3 pagesChina y Covid 2MariaNo ratings yet
- Can Psychological Resilience Protect The Mental Health of Healthcare Professionals During The COVID-19 Pandemic Period?Document7 pagesCan Psychological Resilience Protect The Mental Health of Healthcare Professionals During The COVID-19 Pandemic Period?Jenefer AntoNo ratings yet
- Job Demands, Resources and Strains of Outpatient Caregivers During The COVID-19 Pandemic in Germany: A Qualitative StudyDocument26 pagesJob Demands, Resources and Strains of Outpatient Caregivers During The COVID-19 Pandemic in Germany: A Qualitative StudySylvia ThohariNo ratings yet
- Epidemiology of Mental Health Problems in COVID-19 - A ReviewDocument16 pagesEpidemiology of Mental Health Problems in COVID-19 - A ReviewIrinNo ratings yet
- Listening To Hospital Personnel's Narratives During The COVID-19 OutbreakDocument15 pagesListening To Hospital Personnel's Narratives During The COVID-19 OutbreakAshers NyawoNo ratings yet
- Field Methods in PsychologyDocument19 pagesField Methods in PsychologyHanny OlasoNo ratings yet
- Psychological Consequences of COVID-19 and Challenges For Post-Traumatic InterventionsDocument7 pagesPsychological Consequences of COVID-19 and Challenges For Post-Traumatic InterventionsCaterina MorosanuNo ratings yet
- COVID-19Paper 2020 PDFDocument7 pagesCOVID-19Paper 2020 PDFCaterina MorosanuNo ratings yet
- Progression of Mental Health Services During The COVID-19 Outbreak in ChinaDocument7 pagesProgression of Mental Health Services During The COVID-19 Outbreak in ChinaPelayocvNo ratings yet
- Mental Health and Psychosocial Well-Being During The COVID-19 Pandemic: The Invisible Elephant in The RoomDocument5 pagesMental Health and Psychosocial Well-Being During The COVID-19 Pandemic: The Invisible Elephant in The RoomViaNo ratings yet
- Mental Health and Psychosocial Well-Being During The COVID-19 Pandemic: The Invisible Elephant in The RoomDocument5 pagesMental Health and Psychosocial Well-Being During The COVID-19 Pandemic: The Invisible Elephant in The RoomQueenzee AsuncionNo ratings yet
- Psychological and Emotional Impact of COVID19 Pandemic On People Living With Chronic Disease HIV and Cancer2022AIDS and BehaviorDocument11 pagesPsychological and Emotional Impact of COVID19 Pandemic On People Living With Chronic Disease HIV and Cancer2022AIDS and Behaviorsarita anguloNo ratings yet
- Indicating A Gap Ba Ni?Document3 pagesIndicating A Gap Ba Ni?Reyana K' Marie PabutoyNo ratings yet
- Bachelor in Nursing Science With Honours SEMESTER 8/2021Document20 pagesBachelor in Nursing Science With Honours SEMESTER 8/2021Ranusha AnushaNo ratings yet
- COVID-19 Pandemicandhealthworkerstress: Themediating Effect of Emotional RegulationDocument13 pagesCOVID-19 Pandemicandhealthworkerstress: Themediating Effect of Emotional RegulationShukri RahmanNo ratings yet
- COVID-19 AFRICA, HAITI, AND THE U. S. VIRGIN ISLANDS:: The Response, the Aftermath, & Future ProjectionsFrom EverandCOVID-19 AFRICA, HAITI, AND THE U. S. VIRGIN ISLANDS:: The Response, the Aftermath, & Future ProjectionsNo ratings yet
- Weight Stigmatization and Binge Eating in Asian Americans With Overweight and ObesityDocument15 pagesWeight Stigmatization and Binge Eating in Asian Americans With Overweight and ObesityNatalia BettancourtNo ratings yet
- Intimate Partner Violence As A Risk Factor For Mental Disorders: A Meta-AnalysisDocument34 pagesIntimate Partner Violence As A Risk Factor For Mental Disorders: A Meta-AnalysisNatalia BettancourtNo ratings yet
- BF 03392162Document13 pagesBF 03392162Natalia BettancourtNo ratings yet
- Teaching The Mindful Self-Compassion Program A Guide For Professionals (Christopher Germer, Kristin Neff) (Z-Library)Document475 pagesTeaching The Mindful Self-Compassion Program A Guide For Professionals (Christopher Germer, Kristin Neff) (Z-Library)Natalia Bettancourt86% (14)
- Established and Emerging Perpectives On Violence in Intimate RelationshipsDocument34 pagesEstablished and Emerging Perpectives On Violence in Intimate RelationshipsNatalia BettancourtNo ratings yet
- ATA2023 Annual Conference & ExpoDocument3 pagesATA2023 Annual Conference & ExpoNatalia BettancourtNo ratings yet
- Get Out of Your Mind & Into Your Life For Teens - Ciarrochi - Hayes y BaileyDocument154 pagesGet Out of Your Mind & Into Your Life For Teens - Ciarrochi - Hayes y BaileyNatalia BettancourtNo ratings yet
- Journal of Interprofessional Education & Practice: Kristine Wood, Carolanne CariniDocument4 pagesJournal of Interprofessional Education & Practice: Kristine Wood, Carolanne CariniNatalia BettancourtNo ratings yet
- ASNJ-Volume 9-Issue 27 - Page 180-190Document11 pagesASNJ-Volume 9-Issue 27 - Page 180-190Natalia BettancourtNo ratings yet
- Functional Analytic Psychotherapy For Nursing Home Residents: A Single-Subject Investigation of Session-by-Session ChangesDocument8 pagesFunctional Analytic Psychotherapy For Nursing Home Residents: A Single-Subject Investigation of Session-by-Session ChangesNatalia BettancourtNo ratings yet
- Randomised Control Trial of A Proactive Intervention Supporting Recovery in Relation To Stress and Irregular Work Hours - Effects On Sleep, Burn-Out, Fatigue and Somatic SymptomsDocument10 pagesRandomised Control Trial of A Proactive Intervention Supporting Recovery in Relation To Stress and Irregular Work Hours - Effects On Sleep, Burn-Out, Fatigue and Somatic SymptomsNatalia BettancourtNo ratings yet
- Mindfulness at WorkDocument47 pagesMindfulness at WorkNatalia BettancourtNo ratings yet
- Nihms 564241Document33 pagesNihms 564241Natalia BettancourtNo ratings yet
- ACT For Interpersonal ProblemsDocument217 pagesACT For Interpersonal ProblemsNatalia BettancourtNo ratings yet
- Burnout, Compassion Fatigue and Psychological Flexibility Among Geriatric Nurses - A Multicenter Study in SpainDocument11 pagesBurnout, Compassion Fatigue and Psychological Flexibility Among Geriatric Nurses - A Multicenter Study in SpainNatalia BettancourtNo ratings yet
- How Other - and Self-Compassion Reduce Burnout Through Resource ReplenishmentDocument27 pagesHow Other - and Self-Compassion Reduce Burnout Through Resource ReplenishmentNatalia BettancourtNo ratings yet
- Behavior Therapy 42 (2011) 700 - 715: T Single Most Preventable Cause of Death, Contributing To Over 443,000 DeathsDocument16 pagesBehavior Therapy 42 (2011) 700 - 715: T Single Most Preventable Cause of Death, Contributing To Over 443,000 DeathsNatalia BettancourtNo ratings yet
- El Quebrantamiento de Las Órdenes de Protección en Violencia de Género - Análisis de Los Indicadores de Riesgo Mediante El Formulario VPRDocument12 pagesEl Quebrantamiento de Las Órdenes de Protección en Violencia de Género - Análisis de Los Indicadores de Riesgo Mediante El Formulario VPRNatalia BettancourtNo ratings yet
- 10 1080@0092623X 2019 1610125Document36 pages10 1080@0092623X 2019 1610125Natalia BettancourtNo ratings yet
- Reducing Inadvertent Clinical Errors - Guidelines From Functional Analytic PsychotherapyDocument5 pagesReducing Inadvertent Clinical Errors - Guidelines From Functional Analytic PsychotherapyNatalia BettancourtNo ratings yet
- The Functional Analytic Psychotherapy Rating Scale (FAPRS) : A Behavioral Psychotherapy Coding SystemDocument19 pagesThe Functional Analytic Psychotherapy Rating Scale (FAPRS) : A Behavioral Psychotherapy Coding SystemNatalia BettancourtNo ratings yet
- Exam Style Answers 20 Asal Chem CBDocument3 pagesExam Style Answers 20 Asal Chem CBhxuNo ratings yet
- Toshiba Air Conditioning Better Air Solutions: Dx-Coil Interface TrainingDocument57 pagesToshiba Air Conditioning Better Air Solutions: Dx-Coil Interface TrainingTín Nguyễn ThànhNo ratings yet
- C Programming Questions and AnswersDocument18 pagesC Programming Questions and AnswerschitranshpandeyNo ratings yet
- Oracle Database Appliance Bare Metal Restore StepsDocument7 pagesOracle Database Appliance Bare Metal Restore StepsKarthika TatiparthiNo ratings yet
- Preboard MsteDocument6 pagesPreboard MsteWinter DeeneNo ratings yet
- United States v. Juvenal Martinez Alvarado, 321 F.2d 336, 2d Cir. (1963)Document5 pagesUnited States v. Juvenal Martinez Alvarado, 321 F.2d 336, 2d Cir. (1963)Scribd Government DocsNo ratings yet
- Fluid IIDocument2 pagesFluid IIJefara 01No ratings yet
- Rishabh Malhotra - Offer LetterDocument4 pagesRishabh Malhotra - Offer LetterrishabhNo ratings yet
- Autodesk 2015 Products Direct Download LinksDocument2 pagesAutodesk 2015 Products Direct Download LinksALEXNo ratings yet
- MGT610-FinalTerm-By Rana Abubakar KhanDocument28 pagesMGT610-FinalTerm-By Rana Abubakar KhanAtif MubasharNo ratings yet
- SupplyPower Overview Presentation SuppliersDocument20 pagesSupplyPower Overview Presentation SuppliersCarlos CarranzaNo ratings yet
- Følstad & Brandtzaeg (2020)Document14 pagesFølstad & Brandtzaeg (2020)Ijlal Shidqi Al KindiNo ratings yet
- TTMA RP 32 EngDocument3 pagesTTMA RP 32 Englinh caca huynhNo ratings yet
- Little ASP Net Core BookDocument124 pagesLittle ASP Net Core Booklauhom130% (1)
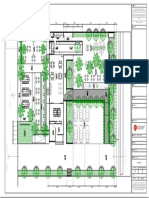
- Layout CitarasaDocument1 pageLayout CitarasaMuchammad Ugi SyahroniNo ratings yet
- PDS Class Test 2: Let Us Establish The Pointer From Autumn Break To PDS!!!Document26 pagesPDS Class Test 2: Let Us Establish The Pointer From Autumn Break To PDS!!!Abhinaba SahaNo ratings yet
- Rubber Loc Cleaner A Methyl Ethyl Ketone M.E.K. Conveyor Belt Repair Kit V1 PDFDocument8 pagesRubber Loc Cleaner A Methyl Ethyl Ketone M.E.K. Conveyor Belt Repair Kit V1 PDFOscar Giovani SosaNo ratings yet
- Master Formula New UpdateDocument5 pagesMaster Formula New UpdateAdhoNo ratings yet
- Ex3 Accounting For MaterialsDocument2 pagesEx3 Accounting For MaterialsCHACHACHANo ratings yet
- Photos - MV. Bahtera CemerlangDocument46 pagesPhotos - MV. Bahtera CemerlangEka Prasetya NugrahaNo ratings yet
- Pamas S4031 WG: Portable Particle Counting System For Water Based Hydraulic FluidsDocument2 pagesPamas S4031 WG: Portable Particle Counting System For Water Based Hydraulic FluidsSupriyaNathRayNo ratings yet
- Computer Science Lesson Plan Week 2-PracticalDocument3 pagesComputer Science Lesson Plan Week 2-PracticalIshrat JehanNo ratings yet
- 4140 HTDocument2 pages4140 HTwillys8No ratings yet
- Energy Audit of A 400-220 KV SubstationDocument8 pagesEnergy Audit of A 400-220 KV Substationabhishekrathi09100% (2)
- John Paulding MuseumDocument4 pagesJohn Paulding Museumapi-316020003No ratings yet
- Least Cost System Operation: Economic Dispatch 2: Smith College, EGR 325 March 10, 2006Document37 pagesLeast Cost System Operation: Economic Dispatch 2: Smith College, EGR 325 March 10, 2006DalessandroNo ratings yet
- Pre-Heater of Nat GasDocument12 pagesPre-Heater of Nat GasStl JoseNo ratings yet
- Siemens - Sitrans Lr200Document192 pagesSiemens - Sitrans Lr200Jonathan Olivier Salgado NesbetNo ratings yet
- January 01 To 31 2023 Rbi GR B Sebi GR A Nabard GR A Lyst3150Document95 pagesJanuary 01 To 31 2023 Rbi GR B Sebi GR A Nabard GR A Lyst3150kulvender singh100% (1)
- 09 Quotation For CC Kerb PDFDocument2 pages09 Quotation For CC Kerb PDFD V BHASKARNo ratings yet