You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- PTNS Incontinencia UrinariaDocument12 pagesPTNS Incontinencia UrinariaSantiago Mondragon RiosNo ratings yet
- Oxford Knee ScoreDocument2 pagesOxford Knee ScoreSantiago Mondragon RiosNo ratings yet
- Part 2 - Knee Society ScoreDocument1 pagePart 2 - Knee Society ScoreSantiago Mondragon RiosNo ratings yet
- The Knee Society Short Form Reduces Respondent Burden in The Assessment of Patient-Reported OutcomesDocument9 pagesThe Knee Society Short Form Reduces Respondent Burden in The Assessment of Patient-Reported OutcomesSantiago Mondragon RiosNo ratings yet
- Psychometric Properties of Four Common Clinical Tests For Assessing Hamstring Flexibility in Young Adults.Document8 pagesPsychometric Properties of Four Common Clinical Tests For Assessing Hamstring Flexibility in Young Adults.Santiago Mondragon RiosNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Control Panel Space OptimizationDocument12 pagesControl Panel Space Optimizationyopy_yogieNo ratings yet
- Decision Theory Tutorial 1Document13 pagesDecision Theory Tutorial 1JakubNo ratings yet
- Kimya 3 - RaporuDocument4 pagesKimya 3 - RaporuFiras 01No ratings yet
- The Logstash BookDocument239 pagesThe Logstash Bookavira100% (1)
- A GCE Physics B 2865 01 January 2006 Question PaperDocument24 pagesA GCE Physics B 2865 01 January 2006 Question PaperMitul KaziNo ratings yet
- Preston Blair - Cartoon AnimationDocument202 pagesPreston Blair - Cartoon AnimationMirthyn96% (76)
- MN Mining EngineeringDocument2 pagesMN Mining EngineeringsahithkumarNo ratings yet
- Jose Raul Capablanca With White (1901-1941)Document249 pagesJose Raul Capablanca With White (1901-1941)Odysseas 57No ratings yet
- Unit TestDocument28 pagesUnit TestyogashankarNo ratings yet
- IEO Syllabus Third Year-Computer Science EngineeringDocument2 pagesIEO Syllabus Third Year-Computer Science EngineeringsusmitaNo ratings yet
- Flashing Routerboards With OpenWRT PDFDocument11 pagesFlashing Routerboards With OpenWRT PDFdamianuskrowinNo ratings yet
- DSP Flash Programming TutorialDocument3 pagesDSP Flash Programming TutorialSeth HarrisNo ratings yet
- Metaphysics by DefaultDocument210 pagesMetaphysics by DefaultHadi HusainNo ratings yet
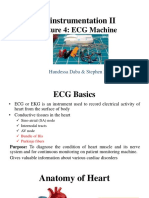
- Bioinstrumentation II: Lecture 4: ECG MachineDocument30 pagesBioinstrumentation II: Lecture 4: ECG MachineHundessa DabaNo ratings yet
- MMW Chapter 3 Practice Activity - CAMACHO PDFDocument7 pagesMMW Chapter 3 Practice Activity - CAMACHO PDFJustin Maree CamachoNo ratings yet
- Ilyte: Automated Electrolyte AnalyzersDocument6 pagesIlyte: Automated Electrolyte AnalyzersAlejandro CabreraNo ratings yet
- Dka GuidelineDocument16 pagesDka GuidelineGhada HusseinNo ratings yet
- Forms PDFDocument18 pagesForms PDFRavi ShankarNo ratings yet
- Tromp Curve ExampleDocument3 pagesTromp Curve Examplesempatik721100% (5)
- Final Step-A Answer KeyDocument7 pagesFinal Step-A Answer KeyVansh Jain100% (1)
- Proximate Analysis of CoalDocument2 pagesProximate Analysis of CoalManna PintoNo ratings yet
- Complex PrimerDocument29 pagesComplex PrimerMaxiene Andrei GuintoNo ratings yet
- 2012 - Partial Discharge Testing - ResumeDocument4 pages2012 - Partial Discharge Testing - Resumediogoufrn-1No ratings yet
- WTL Developer's GuideDocument225 pagesWTL Developer's GuideIvan Martyushov100% (1)
- Cs6659-Artificial IntelligenceDocument44 pagesCs6659-Artificial IntelligenceprakashNo ratings yet
- Product CatalogueDocument24 pagesProduct Cataloguerupa thakkarNo ratings yet
- Group 8, Welding AssignmentDocument11 pagesGroup 8, Welding AssignmentKavish ChandraNo ratings yet
- Data Management TURBANDocument39 pagesData Management TURBANArwie H. FernandoNo ratings yet
- 10Z 3Document95 pages10Z 3ZMCONTROLNo ratings yet
- B.Sc. (IT) (Bachelor of Science in Information Technology) : Syllabus 2011 (Term 2)Document6 pagesB.Sc. (IT) (Bachelor of Science in Information Technology) : Syllabus 2011 (Term 2)Manish ShresthaNo ratings yet