You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- With AnswersDocument14 pagesWith AnswersHarsha Vipin100% (1)
- Impaired Urinary EliminationDocument2 pagesImpaired Urinary EliminationSiafei RabeNo ratings yet
- grp52 UTI PathoDocument3 pagesgrp52 UTI Pathokcdgrvn100% (3)
- Critical AppraisalDocument5 pagesCritical Appraisalfadhil03No ratings yet
- (Tugas) Bedah Dan Orthopaedi Journal FractureDocument4 pages(Tugas) Bedah Dan Orthopaedi Journal Fracturefadhil03No ratings yet
- Consultant On Site:: Emergency Surgical Services Wednesday, April 12 2023Document39 pagesConsultant On Site:: Emergency Surgical Services Wednesday, April 12 2023fadhil03No ratings yet
- Shalter HarrisDocument9 pagesShalter Harrisfadhil03No ratings yet
- Crush InjuryDocument8 pagesCrush Injuryfadhil03No ratings yet
- Management of Fingertip Injuries: A Survey of Opinions of Surgeons WorldwideDocument7 pagesManagement of Fingertip Injuries: A Survey of Opinions of Surgeons Worldwidefadhil03No ratings yet
- TG18 MondayDocument34 pagesTG18 Mondayfadhil03No ratings yet
- Pathogeneesis and Current Treatment of Osteosarcoma (4) 2Document17 pagesPathogeneesis and Current Treatment of Osteosarcoma (4) 2fadhil03No ratings yet
- Prosedur Tindakan Yang Sering Dilakukan Sesuai ICD9CMDocument13 pagesProsedur Tindakan Yang Sering Dilakukan Sesuai ICD9CMadefcesyoNo ratings yet
- Navkar Surgical Hospital in AhmedabadDocument3 pagesNavkar Surgical Hospital in AhmedabadNavkar SurgicalNo ratings yet
- BPH Guideline 2019Document10 pagesBPH Guideline 2019Nun AdeninNo ratings yet
- Submental Intubation.20150306120342Document5 pagesSubmental Intubation.20150306120342dini anitaNo ratings yet
- POLITRAUMATISMODocument13 pagesPOLITRAUMATISMOJOSENo ratings yet
- Hifu MachineDocument6 pagesHifu MachineShawn SimpsonNo ratings yet
- Ijcmsr 312 v1Document7 pagesIjcmsr 312 v1AshliiqueNo ratings yet
- Urinary Catheter: IndwellingDocument3 pagesUrinary Catheter: IndwellingKevinNo ratings yet
- Achalasia: Dr. Yusmaidi, SPB - KBD Digestive Surgery, Lampung Medical School LampungDocument40 pagesAchalasia: Dr. Yusmaidi, SPB - KBD Digestive Surgery, Lampung Medical School LampungsitizahniaNo ratings yet
- The Privacy Isuues of AppleDocument7 pagesThe Privacy Isuues of Applephysicser15No ratings yet
- 990812 EUS教學 (4) 重點式急診泌尿系統超音波之應用Document77 pages990812 EUS教學 (4) 重點式急診泌尿系統超音波之應用juice119100% (2)
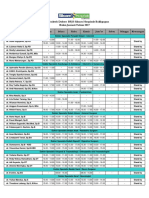
- Januari 2017 - Jadwal Praktek Klinik BPJS Kesehatan PDFDocument2 pagesJanuari 2017 - Jadwal Praktek Klinik BPJS Kesehatan PDFVirly EffendiNo ratings yet
- Gelombang Ii - Koordinator: Dr. Irra Rubianti Widarda, SPB - Spbp-Re (K) Tgl. 24 - 26 April 2-18Document2 pagesGelombang Ii - Koordinator: Dr. Irra Rubianti Widarda, SPB - Spbp-Re (K) Tgl. 24 - 26 April 2-18Andrian Sitompul0% (1)
- Daftar Pustaka Frozen ShoulderDocument3 pagesDaftar Pustaka Frozen ShoulderMuhammad Faza NaufalNo ratings yet
- Announcement Fiesta Urologi 2017Document8 pagesAnnouncement Fiesta Urologi 2017Alfin KamalNo ratings yet
- The Bucket-Handle Tear of The MeniscusDocument5 pagesThe Bucket-Handle Tear of The Meniscusich khuyNo ratings yet
- Bangladesh Eye Hospital PDFDocument3 pagesBangladesh Eye Hospital PDFShabbirul AlamNo ratings yet
- Enlarged Prostate BPH and The BladderDocument8 pagesEnlarged Prostate BPH and The BladderAndrej HNo ratings yet
- Kompetensi Bedah DigestifDocument5 pagesKompetensi Bedah DigestifOksayana Lutta100% (1)
- S2 FKU 2007 Hasmija Bibliography - PDFDocument3 pagesS2 FKU 2007 Hasmija Bibliography - PDFAngel KoteNo ratings yet
- CGHS RATE List PDFDocument42 pagesCGHS RATE List PDFNarain Kumar LangehNo ratings yet
- GonorrheaDocument9 pagesGonorrheaPencenk AzznewNo ratings yet
- SX TemplateDocument2 pagesSX Templatesjmc.surgeryresidentsNo ratings yet
- डॉक्टर स्केड्युल (मानव कल्याण केंद्र)Document6 pagesडॉक्टर स्केड्युल (मानव कल्याण केंद्र)Sudeep NikamNo ratings yet
- Medical Treatment Prices - ListDocument25 pagesMedical Treatment Prices - ListWellness Destination IndiaNo ratings yet
- Coding ExamplesDocument6 pagesCoding ExamplesKrishna KumarNo ratings yet
- Baumann 2018Document13 pagesBaumann 2018Sisca Dwi AgustinaNo ratings yet