You might also like
- A. D.D.S., MS.": An Evaluation of Basic Articulators and Their Concepts Part I. Basic ConceptsDocument23 pagesA. D.D.S., MS.": An Evaluation of Basic Articulators and Their Concepts Part I. Basic Conceptsjinny1_0No ratings yet
- Relining and RebasingDocument5 pagesRelining and RebasingMarwaAmerNo ratings yet
- Impression Techniques of FPDDocument20 pagesImpression Techniques of FPDBhavan Chand YemineniNo ratings yet
- Rests Rest SeatsDocument42 pagesRests Rest SeatsSahana RangarajanNo ratings yet
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- Essential Tissue Healing of the Face and NeckFrom EverandEssential Tissue Healing of the Face and NeckRating: 5 out of 5 stars5/5 (2)
- EBOOK Infancy Development From Birth To Age 3 3Rd Edition Ebook PDF Version Download Full Chapter PDF KindleDocument61 pagesEBOOK Infancy Development From Birth To Age 3 3Rd Edition Ebook PDF Version Download Full Chapter PDF Kindlemichael.carathers448100% (42)
- Eye ProsthesisDocument47 pagesEye ProsthesissamysadaNo ratings yet
- Ocular ProsthesisDocument3 pagesOcular ProsthesisAmar BhochhibhoyaNo ratings yet
- Record BlocksDocument59 pagesRecord BlocksahmedNo ratings yet
- Occular ProsthesisDocument30 pagesOccular ProsthesisPavithra BalasubramaniyamNo ratings yet
- Relining & RebasingDocument86 pagesRelining & RebasingJASPREETKAUR0410100% (1)
- Balanced Occlu HandoutDocument9 pagesBalanced Occlu HandoutMostafa FayadNo ratings yet
- Groper's ApplianceDocument4 pagesGroper's Appliancejinny1_0No ratings yet
- Lecture 5 3rd Class PDFDocument6 pagesLecture 5 3rd Class PDFBrandon AviciiNo ratings yet
- Polished Surface of Complete DentureDocument41 pagesPolished Surface of Complete Dentureakl_rahul100% (1)
- Arrangement of TeethDocument65 pagesArrangement of TeethIbrahim Ramadan Eltorky100% (1)
- Maxillofacial Prosthesis materials comparisonDocument52 pagesMaxillofacial Prosthesis materials comparisonShipra SinghNo ratings yet
- Biometric - Approach in CDDocument13 pagesBiometric - Approach in CDmarwaNo ratings yet
- 04 Splintstrismus 140501160338 Phpapp02Document56 pages04 Splintstrismus 140501160338 Phpapp02hazeemmegahedNo ratings yet
- Principles of ExodontiaDocument25 pagesPrinciples of ExodontiaPankaj JindalNo ratings yet
- Types of Acrylic Removable Partial Dentures (RPDsDocument5 pagesTypes of Acrylic Removable Partial Dentures (RPDsmarwaNo ratings yet
- Articulating PapersDocument48 pagesArticulating PapersMayank MalraNo ratings yet
- Guide to Managing Flabby Ridges and Hypertrophic TissuesDocument145 pagesGuide to Managing Flabby Ridges and Hypertrophic TissuesJudy Abbott100% (1)
- Factors Causing Failure of Crowns and Fixed Dental ProsthesisDocument57 pagesFactors Causing Failure of Crowns and Fixed Dental ProsthesisEazhil RajNo ratings yet
- Crown & Bridge or Fixed Prosthodontics Lectures - Level - 3Document4 pagesCrown & Bridge or Fixed Prosthodontics Lectures - Level - 3ruchikaNo ratings yet
- Metal-Inlay/Onlay/Overlay Preparation: Dr. Júlia NemesDocument34 pagesMetal-Inlay/Onlay/Overlay Preparation: Dr. Júlia NemesDwi Riski SaputraNo ratings yet
- 4biomechanics of Removable Partial DenturesDocument15 pages4biomechanics of Removable Partial DenturesDemilyadioppy AbevitNo ratings yet
- Checking and Verification of Crowns and Fixed ProsthesesDocument5 pagesChecking and Verification of Crowns and Fixed Prostheseskhaled alahmadNo ratings yet
- Denture Sequelae: Common Side Effects of Wearing Complete DenturesDocument58 pagesDenture Sequelae: Common Side Effects of Wearing Complete Denturesaayush100% (2)
- Impression Procedures in CD - KIRTI SHARMADocument42 pagesImpression Procedures in CD - KIRTI SHARMAKirti SharmaNo ratings yet
- Flangeless Cast Partial DentureDocument5 pagesFlangeless Cast Partial DentureDeasiree100% (1)
- 4-Fluid Control &tissue DilationDocument57 pages4-Fluid Control &tissue Dilationyahia salahNo ratings yet
- 7 Horizontal Jaw RelationsDocument11 pages7 Horizontal Jaw Relationsعلي محمود جمالNo ratings yet
- Applied Anatomy Related To Complete Denture-Maxilla MandibleDocument57 pagesApplied Anatomy Related To Complete Denture-Maxilla MandibleRen Jye ChongNo ratings yet
- Single Complete DenturesDocument20 pagesSingle Complete DenturesDeepthi RajeshNo ratings yet
- OverdentureDocument227 pagesOverdentureEazhil RajNo ratings yet
- Bio-Medical Research Ethics GuideDocument22 pagesBio-Medical Research Ethics GuideAnant KhotNo ratings yet
- Classification of Articulators: Awni Rihani, D.D.S., M.Sc.Document4 pagesClassification of Articulators: Awni Rihani, D.D.S., M.Sc.Shanna MitchellNo ratings yet
- Denture Post-Insertion ProblemsDocument108 pagesDenture Post-Insertion Problemsranjeet kumar chaudharyNo ratings yet
- MCQ/BCQ: Subtheme: DiagnosisDocument3 pagesMCQ/BCQ: Subtheme: DiagnosisYusra Shaukat100% (1)
- Rest and Rest Seats: An OverviewDocument20 pagesRest and Rest Seats: An OverviewCharmiNo ratings yet
- Occlusion in Complete DentureDocument35 pagesOcclusion in Complete DentureAkash Sikka100% (1)
- GENERAL PRINCIPLES OF SHADE SELECTION LDDocument3 pagesGENERAL PRINCIPLES OF SHADE SELECTION LDrasagna reddyNo ratings yet
- ObturatorsDocument79 pagesObturatorsPremshith CpNo ratings yet
- Anteroposterior Palatal StrapDocument2 pagesAnteroposterior Palatal StrapAhmad Kareem100% (2)
- Single Denture - II-Combination SyndromeDocument30 pagesSingle Denture - II-Combination SyndromeIsmail HamadaNo ratings yet
- Theories of Impression Making and Impression Procedure For Complete DentureDocument63 pagesTheories of Impression Making and Impression Procedure For Complete DenturemanjulikaNo ratings yet
- Orbital ProsthesisDocument5 pagesOrbital ProsthesisdrsmritiNo ratings yet
- Occlusion / Orthodontic Courses by Indian Dental AcademyDocument90 pagesOcclusion / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Gtl18.Occlusal Correction Lec 18 Drfmha 2nd YearDocument11 pagesGtl18.Occlusal Correction Lec 18 Drfmha 2nd YearLuciaTrinovenaLaseNo ratings yet
- Dent 343 Lect 9 - HandoutDocument18 pagesDent 343 Lect 9 - HandoutAnas AmerNo ratings yet
- Classification of Maxillofacial Defects: A Review ArticleDocument7 pagesClassification of Maxillofacial Defects: A Review ArticleIJAR JOURNALNo ratings yet
- Review Article: Prosthodontic Management of Patients With Diabetes MellitusDocument7 pagesReview Article: Prosthodontic Management of Patients With Diabetes MellitusMrinmayee ThakurNo ratings yet
- Face Bow PDFDocument4 pagesFace Bow PDFAnkit VermaNo ratings yet
- Overdenture 140503222227 Phpapp01Document107 pagesOverdenture 140503222227 Phpapp01TatsamYadavNo ratings yet
- Ocular and Orbital ProsthesisDocument69 pagesOcular and Orbital ProsthesisAkshayaa BalajiNo ratings yet
- Artificial Teeth Selection GuideDocument5 pagesArtificial Teeth Selection GuideIbrahim Ramadan Eltorky100% (1)
- Adverse Effects of Wearing Complete Dentures (CDsDocument41 pagesAdverse Effects of Wearing Complete Dentures (CDsEppy Ka50% (4)
- UntitledDocument72 pagesUntitledrajaniNo ratings yet
- Split FingerDocument6 pagesSplit FingerrajaniNo ratings yet
- The Socket-Shield Technique at Molar Sites: A Proof-Of-Principle Technique Report. C Schwimer Et Al. JPD 2018:5 (12) 56-60Document33 pagesThe Socket-Shield Technique at Molar Sites: A Proof-Of-Principle Technique Report. C Schwimer Et Al. JPD 2018:5 (12) 56-60rajaniNo ratings yet
- 15.ocular ProsthesisDocument156 pages15.ocular ProsthesisrajaniNo ratings yet
- Ergonomics in DentistryDocument143 pagesErgonomics in DentistryrajaniNo ratings yet
- Virtual Impressions and Virtual and Stereolithographic ModelsDocument86 pagesVirtual Impressions and Virtual and Stereolithographic ModelsrajaniNo ratings yet
- Occlusal Splints: Presented By: Anubhuti Dubey Mds 3 Year Guided By: Dr. Shilpa JainDocument132 pagesOcclusal Splints: Presented By: Anubhuti Dubey Mds 3 Year Guided By: Dr. Shilpa JainrajaniNo ratings yet
- Dental Waxes GuideDocument18 pagesDental Waxes GuiderajaniNo ratings yet
- SurveyorsDocument22 pagesSurveyorsrajaniNo ratings yet
- 3.trigeminal NerveDocument81 pages3.trigeminal NerverajaniNo ratings yet
- JCDR 8 ZD04Document3 pagesJCDR 8 ZD04rajaniNo ratings yet
- Addition SiliconeDocument3 pagesAddition SiliconerajaniNo ratings yet
- 3 TrigeminalwordDocument26 pages3 TrigeminalwordrajaniNo ratings yet
- Anterior Teeth SelectionDocument30 pagesAnterior Teeth Selectionrajani100% (1)
- Direct RetainerDocument25 pagesDirect RetainerrajaniNo ratings yet
- New Horizons Dental College special case of TMJ disorder patientDocument2 pagesNew Horizons Dental College special case of TMJ disorder patientrajaniNo ratings yet
- Impressions in CDDocument95 pagesImpressions in CDrajani100% (1)
- My New Article 2020 JRADDocument5 pagesMy New Article 2020 JRADrajaniNo ratings yet
- Chap 26 - Assessing Male Genitalia (Interview Guide)Document3 pagesChap 26 - Assessing Male Genitalia (Interview Guide)Mary Cielo DomagasNo ratings yet
- Demographics: Discharge DocumentationDocument8 pagesDemographics: Discharge Documentationjenny100% (1)
- Quiz1 KeyDocument8 pagesQuiz1 KeyAli KalyarNo ratings yet
- Nutrition Factor in Women in Backward AreasDocument7 pagesNutrition Factor in Women in Backward AreaspranjalNo ratings yet
- Mallari 397-414Document19 pagesMallari 397-414Trixia Louise NastorNo ratings yet
- Swamy PDFDocument20 pagesSwamy PDFsreejithNo ratings yet
- Louela C. Acedera, RN, MANDocument18 pagesLouela C. Acedera, RN, MANelle seigdenNo ratings yet
- Intellectual Disability and Assistive Technology: Opening The Gate WiderDocument4 pagesIntellectual Disability and Assistive Technology: Opening The Gate WiderBudi Darmawan DiswanNo ratings yet
- Performance Rating FormDocument2 pagesPerformance Rating FormArielle Ramirez67% (3)
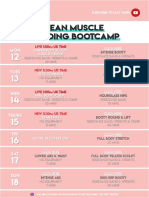
- 26 - LEAN Weekly Guide - On - October 12Document15 pages26 - LEAN Weekly Guide - On - October 12Andrea CsillaNo ratings yet
- Coomber, & Barriball, 2007Document18 pagesCoomber, & Barriball, 20070112joeriNo ratings yet
- MARIELLE CHUA - (Template) SOAPIE CaseletDocument9 pagesMARIELLE CHUA - (Template) SOAPIE CaseletMarielle Chua100% (1)
- Institución Educativa Almirante Padilla: Informacion Basica de La Secuencia DidacticaDocument3 pagesInstitución Educativa Almirante Padilla: Informacion Basica de La Secuencia DidacticaGreys NarvaezNo ratings yet
- Turn Table - LLT-750Document29 pagesTurn Table - LLT-750Sadashiva sahooNo ratings yet
- Kape-Hc-217042-03-06-2022 Butyl ReclaimDocument1 pageKape-Hc-217042-03-06-2022 Butyl Reclaim0911khanNo ratings yet
- Assessment PrintDocument204 pagesAssessment Printbruceaq100% (7)
- FSL Indicator - Handbook - 17.03.2020Document75 pagesFSL Indicator - Handbook - 17.03.2020Muaath Al-BahramiNo ratings yet
- The Impact of Cyberbullying To The Mental Health of The Grade 12 AbmDocument19 pagesThe Impact of Cyberbullying To The Mental Health of The Grade 12 AbmSerene RiegoNo ratings yet
- APEI - 4 - Sound Pollution PDFDocument23 pagesAPEI - 4 - Sound Pollution PDFManish RoyNo ratings yet
- TFN-Theoretical Foundation in Nursing Reflection Paper: The Core Care Values of A Beginning HOLYNAMIAN Servant Leader Student NurseDocument2 pagesTFN-Theoretical Foundation in Nursing Reflection Paper: The Core Care Values of A Beginning HOLYNAMIAN Servant Leader Student NurseDanica Rose PalacaNo ratings yet
- 11 Thyroid HacksDocument13 pages11 Thyroid HackstthorgalNo ratings yet
- Alfred Adlers Individual PsychologyDocument35 pagesAlfred Adlers Individual PsychologyJerrah RamaNo ratings yet
- Why Texting Is Better Than TalkingDocument4 pagesWhy Texting Is Better Than TalkingjhgfhjgkgkNo ratings yet
- CharittyDocument2 pagesCharittyGeorge EduardNo ratings yet
- Guide To History TakingDocument55 pagesGuide To History TakingGabriella Hild100% (1)
- IBNII Write UpDocument4 pagesIBNII Write Updani danielsNo ratings yet
- QED Achieves 1 Million Safe ManhoursDocument2 pagesQED Achieves 1 Million Safe ManhoursBernabe AlmirolNo ratings yet
- VSP - Vision 01Document1 pageVSP - Vision 01api-252555369No ratings yet
- Vocabulary UNIT - 3 - : - Free Times - GRAMMAR: - Can/Can T For Ability, Like + Verb/nounDocument4 pagesVocabulary UNIT - 3 - : - Free Times - GRAMMAR: - Can/Can T For Ability, Like + Verb/nounRicardo JimenezNo ratings yet