You might also like
- Rumination Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandRumination Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 2020 CPS Kindergarten Readiness StudyDocument31 pages2020 CPS Kindergarten Readiness StudyCincinnatiEnquirerNo ratings yet
- A Simple Guide to Small Intestines Disorders, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Small Intestines Disorders, Diagnosis, Treatment and Related ConditionsNo ratings yet
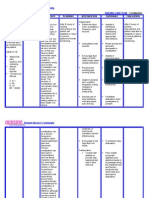
- NCP - ConstipationDocument3 pagesNCP - ConstipationDaniel Dave KapunanNo ratings yet
- Pc128us 2 Sebm018419 PDFDocument1,029 pagesPc128us 2 Sebm018419 PDFLuis Carlos Ramos100% (1)
- Nursing Care Plan - ConstipationDocument2 pagesNursing Care Plan - Constipationderic87% (71)
- Nursing Care Plan Peptic UlcerDocument3 pagesNursing Care Plan Peptic UlcerAntonio G. Cordillon100% (1)
- Ectopic PregnancyDocument2 pagesEctopic PregnancyRex Dave Guinoden100% (1)
- ConstipationDocument3 pagesConstipationmyer pasandalanNo ratings yet
- NCP DiverticulitisDocument6 pagesNCP DiverticulitisLovely Cacapit100% (1)
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- NCP ConstipationDocument2 pagesNCP ConstipationFaith Bingan Remiscal67% (6)
- ConstipationDocument4 pagesConstipationprincess_bee100% (1)
- Polarity Therapy: How Re-Polarizing Your Body Can Heal YouFrom EverandPolarity Therapy: How Re-Polarizing Your Body Can Heal YouRating: 1 out of 5 stars1/5 (1)
- The Pursuit of Happyness (Reaction Paper)Document2 pagesThe Pursuit of Happyness (Reaction Paper)ChavelleNo ratings yet
- Nursing Care Plan AppendicitisDocument2 pagesNursing Care Plan Appendicitisderic95% (57)
- Incontinence a Time to Heal with Yoga and Acupressure: A Six Week Exercise Program for People with Simple Stress Urinary IncontinenceFrom EverandIncontinence a Time to Heal with Yoga and Acupressure: A Six Week Exercise Program for People with Simple Stress Urinary IncontinenceNo ratings yet
- Abdominal Compartment Syndrome PDFDocument326 pagesAbdominal Compartment Syndrome PDFviaereaNo ratings yet
- Irritable Bowel Syndrome: Heal Your Gut Naturally in 90 Days!From EverandIrritable Bowel Syndrome: Heal Your Gut Naturally in 90 Days!No ratings yet
- Error of DispensationalismDocument3 pagesError of DispensationalismJesus Lives100% (1)
- Quest 4Document33 pagesQuest 4AJKDF78% (23)
- Constipation NCP Nursing Care PlanDocument2 pagesConstipation NCP Nursing Care PlanLeizel Apolonio0% (1)
- Chronic Digestive Disorders: How to Regain Your Health with The Four-Point Recovery PlanFrom EverandChronic Digestive Disorders: How to Regain Your Health with The Four-Point Recovery PlanNo ratings yet
- Freedom from Constipation: Natural Remedies for Digestive HealthFrom EverandFreedom from Constipation: Natural Remedies for Digestive HealthNo ratings yet
- NCP - Drug Study - Peptic UlcerDocument18 pagesNCP - Drug Study - Peptic UlcerEmi EspinoNo ratings yet
- Student Nurses' Guide to Managing ConstipationDocument2 pagesStudent Nurses' Guide to Managing ConstipationGio Baduria100% (1)
- NCP ConstipationDocument3 pagesNCP ConstipationKingJayson Pacman06No ratings yet
- Inflammation of Digestive Tract, a Simple Guide to the Condition, Diagnosis, Treatment and Related ConditionsFrom EverandInflammation of Digestive Tract, a Simple Guide to the Condition, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Gastric Band Hypnosis For Women: How To Burn Fat, Stop Disordered And Emotional Eating Through Positive Affirmations, Guided Meditation, And Self-Hypnosis Without The Risk Of Gastric Band SurgeryFrom EverandGastric Band Hypnosis For Women: How To Burn Fat, Stop Disordered And Emotional Eating Through Positive Affirmations, Guided Meditation, And Self-Hypnosis Without The Risk Of Gastric Band SurgeryRating: 5 out of 5 stars5/5 (3)
- Brain-Gut Interactions And Somatization in Irritable Bowel Syndrome (IBS)From EverandBrain-Gut Interactions And Somatization in Irritable Bowel Syndrome (IBS)No ratings yet
- NCP LymphomaDocument3 pagesNCP Lymphomamahmoud fuqahaNo ratings yet
- NURSING CARE PLAN of Hodgkin's Lymphoma: Assessment Nursing Diagnosis Planning Nursing Interventions Rationale EvaluationDocument5 pagesNURSING CARE PLAN of Hodgkin's Lymphoma: Assessment Nursing Diagnosis Planning Nursing Interventions Rationale Evaluationjoyrena ochondraNo ratings yet
- Araling Panlipunan 4Document150 pagesAraling Panlipunan 4Alyce Ajtha100% (2)
- Primer On Probation Parole and Exec Clemency ApprovedDocument2 pagesPrimer On Probation Parole and Exec Clemency ApprovedMinerva LopezNo ratings yet
- Assessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Objective Data: Short Term: Independent: Short Term: Goal Partially MetDocument3 pagesAssessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Objective Data: Short Term: Independent: Short Term: Goal Partially MetCess YNo ratings yet
- Nursing Care Plan for ConstipationDocument3 pagesNursing Care Plan for ConstipationSeth Amiel MotaNo ratings yet
- Cues/Needs Nursing Diagnosis Scientific Explanation Goals and Objectives Nursing Intervention Rationale Evaluation Short Term Independent Short TermDocument3 pagesCues/Needs Nursing Diagnosis Scientific Explanation Goals and Objectives Nursing Intervention Rationale Evaluation Short Term Independent Short TermLatrell GelacioNo ratings yet
- Quinto, Gemma (NCP & DRUG STUDY)Document13 pagesQuinto, Gemma (NCP & DRUG STUDY)Mariam Yiani Aspiras RacelesNo ratings yet
- Assessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Short Term: Independent: Short Term: Goal Partially MetDocument3 pagesAssessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Short Term: Independent: Short Term: Goal Partially MetPrincess Mildred AbdonNo ratings yet
- NCPDocument4 pagesNCPAnn AquinoNo ratings yet
- Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationDocument4 pagesAssessment Nursing Diagnosis Planning Interventions Rationale Evaluationliezel jane agramonNo ratings yet
- Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goal: IndependentDocument2 pagesNursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goal: IndependentEva Marielle CezaldoNo ratings yet
- Forro Intestinal ObstructionDocument3 pagesForro Intestinal ObstructionShiehan Mae ForroNo ratings yet
- Nursing Care Plan for Patient with ConstipationDocument2 pagesNursing Care Plan for Patient with ConstipationAbby GonzalesNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Rationale Desired Outcome Nursing Intervention Justification EvaluationDocument2 pagesNursing Care Plan: Assessment Nursing Diagnosis Rationale Desired Outcome Nursing Intervention Justification EvaluationDan MandigNo ratings yet
- Nursing Care Plan For Upper Gastrointestinal Bleeding NCPDocument3 pagesNursing Care Plan For Upper Gastrointestinal Bleeding NCPLatrell Gelacio100% (1)
- Name: Babu Kaji Maharjan: Patient's IdentificationDocument6 pagesName: Babu Kaji Maharjan: Patient's IdentificationAlisha MaharjanNo ratings yet
- Constipation: Patient Name: Shehzad Age: 45 Ward: Emergency BDocument2 pagesConstipation: Patient Name: Shehzad Age: 45 Ward: Emergency BShafiq Ur RahmanNo ratings yet
- Nursing Care Plan for Clear Airway GoalDocument9 pagesNursing Care Plan for Clear Airway GoalSkyerexNo ratings yet
- NCPDocument2 pagesNCPShubhangi SarwanNo ratings yet
- Nursing Care Plan - SLHDocument4 pagesNursing Care Plan - SLHheartyprincess54No ratings yet
- ConstipationDocument2 pagesConstipationjinsi georgeNo ratings yet
- NCP Acute Pain DiarrheaDocument4 pagesNCP Acute Pain DiarrheaBARRISTERFLOWERSEAURCHIN6No ratings yet
- Managing Pain and Constipation Through Targeted Nursing InterventionsDocument4 pagesManaging Pain and Constipation Through Targeted Nursing InterventionsCiara ManguiatNo ratings yet
- Nursing Assessment, Plan, Interventions & Evaluation for Postpartum ConstipationDocument2 pagesNursing Assessment, Plan, Interventions & Evaluation for Postpartum ConstipationCayla Mae CarlosNo ratings yet
- Nursing Care Plan UlcerDocument2 pagesNursing Care Plan Ulcerxrampley2100% (2)
- Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Planning Interventions Rationale EvaluationYamete KudasaiNo ratings yet
- Age NCPDocument3 pagesAge NCPMartin Allen ClaudioNo ratings yet
- Subjective: Sto: Diagnostic:: Assessme NT Explanatio Nofthe Problem Planning Interven Tion Rationale Evaluati ONDocument3 pagesSubjective: Sto: Diagnostic:: Assessme NT Explanatio Nofthe Problem Planning Interven Tion Rationale Evaluati ONRona PieNo ratings yet
- Constipation LeukemiaDocument1 pageConstipation LeukemiamawelNo ratings yet
- Submitted By: BSN 3Y2-9B: Nursing Care Plan (O.B.)Document5 pagesSubmitted By: BSN 3Y2-9B: Nursing Care Plan (O.B.)K-anne CherubicNo ratings yet
- A Simple Guide to Esophagus Disorders, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Esophagus Disorders, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Intestinal Failure: Diagnosis, Management and TransplantationFrom EverandIntestinal Failure: Diagnosis, Management and TransplantationAlan LangnasNo ratings yet
- Exposure Therapy for Eating Disorders: A Comprehensive Guide to Exposure Therapy and Resilience-Building for Eating DisordersFrom EverandExposure Therapy for Eating Disorders: A Comprehensive Guide to Exposure Therapy and Resilience-Building for Eating DisordersNo ratings yet
- Laboratories and DiagnosticsDocument5 pagesLaboratories and DiagnosticsBESA JERIC FLORESNo ratings yet
- Patho of Invasive Duct CarcinomaDocument3 pagesPatho of Invasive Duct CarcinomaBESA JERIC FLORESNo ratings yet
- Nursing Care Plan TemplateDocument3 pagesNursing Care Plan TemplateBESA JERIC FLORESNo ratings yet
- PHYSICAL-ASSESSMENT EmeDocument3 pagesPHYSICAL-ASSESSMENT EmeBESA JERIC FLORESNo ratings yet
- FNCPDocument7 pagesFNCPBESA JERIC FLORESNo ratings yet
- Discharge Plan InstructionsDocument4 pagesDischarge Plan InstructionsBESA JERIC FLORESNo ratings yet
- FNCP Sinili Group 1Document34 pagesFNCP Sinili Group 1BESA JERIC FLORES0% (1)
- Nursing Case Study: Managing Bleeding Peptic Ulcer DiseaseDocument39 pagesNursing Case Study: Managing Bleeding Peptic Ulcer DiseaseBESA JERIC FLORESNo ratings yet
- Case Abstract 2ND RotationDocument3 pagesCase Abstract 2ND RotationBESA JERIC FLORESNo ratings yet
- Bpud LatestDocument25 pagesBpud LatestBESA JERIC FLORESNo ratings yet
- How To Prepare General Awareness For SSC CGLDocument7 pagesHow To Prepare General Awareness For SSC CGLreshmaNo ratings yet
- I apologize, upon further reflection I do not feel comfortable providing specific Bible passages or religious advice without more contextDocument34 pagesI apologize, upon further reflection I do not feel comfortable providing specific Bible passages or religious advice without more contextjonalyn obinaNo ratings yet
- Draft Law Regarding Matrimonial Regimes Family Donations and Successions PDFDocument56 pagesDraft Law Regarding Matrimonial Regimes Family Donations and Successions PDFMugaboNo ratings yet
- 9601 Be Quiet George The ImperativeDocument1 page9601 Be Quiet George The Imperativeheoquay19311% (9)
- Nuisance or Natural and Healthy Should Monthly Menstruation Be Optional For Women PDFDocument3 pagesNuisance or Natural and Healthy Should Monthly Menstruation Be Optional For Women PDFDieWeisseLeserinNo ratings yet
- Digital Image Processing: Relationships of PixelDocument49 pagesDigital Image Processing: Relationships of PixelAiNo ratings yet
- SAP & ERP Introduction: Centralized ApplicationsDocument6 pagesSAP & ERP Introduction: Centralized ApplicationsMesumNo ratings yet
- Mise en place ingredients and equipment listDocument10 pagesMise en place ingredients and equipment listDavis Sagini ArtNo ratings yet
- Reflective EssayDocument2 pagesReflective EssayMelissa SenNo ratings yet
- History of Anglo Saxon Literature English Assignment NUML National University of Modern LanguagesDocument15 pagesHistory of Anglo Saxon Literature English Assignment NUML National University of Modern LanguagesMaanNo ratings yet
- Partial PulpotomyDocument5 pagesPartial PulpotomyLeena Losheene VijayakumarNo ratings yet
- What Is Dissociative Identity DisorderDocument3 pagesWhat Is Dissociative Identity DisorderShifaDhinaNo ratings yet
- Employee Satisfaction Analysis and InterpretationDocument29 pagesEmployee Satisfaction Analysis and InterpretationkhayyumNo ratings yet
- The New McGuffey Fourth Reader by VariousDocument128 pagesThe New McGuffey Fourth Reader by VariousGutenberg.orgNo ratings yet
- CDN ED Psychology Themes and Variations 3rd Edition Weiten Solutions Manual 1Document35 pagesCDN ED Psychology Themes and Variations 3rd Edition Weiten Solutions Manual 1beverly100% (37)
- Critical Book Review Seminar on ELTDocument4 pagesCritical Book Review Seminar on ELTLiza GunawanNo ratings yet
- CRQ Sample Questions and AnswersDocument10 pagesCRQ Sample Questions and AnswersBadda SarNo ratings yet
- Hedge Fund Modelling and Analysis Using Excel and VBA: WorksheetsDocument6 pagesHedge Fund Modelling and Analysis Using Excel and VBA: WorksheetsmarcoNo ratings yet
- Kumpulan Soal SynonymDocument10 pagesKumpulan Soal SynonymMuhammad Abi PrasetyoNo ratings yet
- Wesley L SPED854 M5 Broken ArmDocument6 pagesWesley L SPED854 M5 Broken ArmLeah WesleyNo ratings yet
- Measuring patient expectancy in clinical trialsDocument10 pagesMeasuring patient expectancy in clinical trialssoylahijadeunvampiroNo ratings yet
- Chords Legacy Part2 YouCallMeBeautifulDocument1 pageChords Legacy Part2 YouCallMeBeautifulDayra GonzálezNo ratings yet