You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Our EnvironmentDocument11 pagesOur EnvironmentHVBCBMNZNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Civil Green ConcreteDocument18 pagesCivil Green Concretesharukh88% (8)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Composting ProcessDocument5 pagesComposting ProcessjueliiyaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- ACt 6Document6 pagesACt 6Joshua de JesusNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- BMWInspection ReportDocument4 pagesBMWInspection Reportab505450No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Complete The Sentences With The Words or Phrases in Part IDocument3 pagesComplete The Sentences With The Words or Phrases in Part IĐỗ Trần Bảo ThyNo ratings yet
- PESA KarachiDocument68 pagesPESA KarachiAzmatNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Nike Vs AdidasDocument25 pagesNike Vs AdidasSandhyaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- E I A ReportDocument213 pagesE I A ReportWTF entertrainmentNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- City Vs VillageDocument4 pagesCity Vs VillageAyuni Warhamni100% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Land PollutionDocument2 pagesLand PollutionmoniqueNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- EMPDocument24 pagesEMPYexiong YIALENGNo ratings yet
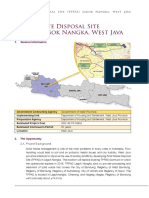
- Final Waste Disposal Site TPPAS Legok Nangka West JavaDocument3 pagesFinal Waste Disposal Site TPPAS Legok Nangka West JavaDavid SoehartonoNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Unit 1-Step 1 - Implement Cleaner Production Opportunities in The Home StepDocument6 pagesUnit 1-Step 1 - Implement Cleaner Production Opportunities in The Home StepRosario CastañedaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Food Lab Safety ContractDocument3 pagesFood Lab Safety Contractapi-439595804No ratings yet
- Lebanon Environmental Assessment of The Syrian Conflict & Priority InterventionsDocument182 pagesLebanon Environmental Assessment of The Syrian Conflict & Priority InterventionsMarco GiallonardiNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Green BuildingDocument16 pagesThe Green BuildingDeanNo ratings yet
- T TP 2550077 Ocean Pollution Single Use Plastics Quick Facts ks2 Powerpoint - Ver - 1Document8 pagesT TP 2550077 Ocean Pollution Single Use Plastics Quick Facts ks2 Powerpoint - Ver - 1carrie929ukNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Barangay Solid Waste Management Annual Action Plan 1Document2 pagesBarangay Solid Waste Management Annual Action Plan 1Janis SuperoNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- S11ES Ii 20Document6 pagesS11ES Ii 20allanrnmanalotoNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- BBA AssignmentDocument2 pagesBBA Assignmentarchana agarwalNo ratings yet
- (123doc) - De-Thi-Hoc-Sinh-Gioi-Tieng-Anh-9-Huyen-Tam-Duong-Nam-Hoc-2010-2011-Co-Dap-AnDocument5 pages(123doc) - De-Thi-Hoc-Sinh-Gioi-Tieng-Anh-9-Huyen-Tam-Duong-Nam-Hoc-2010-2011-Co-Dap-AnNaruto SakuraNo ratings yet
- CONCLUSION EnvDocument3 pagesCONCLUSION EnvNoor FatihahNo ratings yet
- Urban Feildwork Finale ReportDocument27 pagesUrban Feildwork Finale ReportOjullaIsaac100% (1)
- Approach in Developing Environmental Management Plan (EMP) : AbstractDocument12 pagesApproach in Developing Environmental Management Plan (EMP) : AbstractAnandhuMANo ratings yet
- A.1 Site Development Including Minor Excavation: Batching and Crushing PlantDocument4 pagesA.1 Site Development Including Minor Excavation: Batching and Crushing PlantJaja BarredoNo ratings yet
- Productivity: Prof. Christian TerwieschDocument46 pagesProductivity: Prof. Christian TerwieschSabila SanjraniNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Response To Public Concerns About RumpkeDocument32 pagesResponse To Public Concerns About RumpkeCameron Knight100% (1)
- Role of An Individual in Prevention of PollutionDocument6 pagesRole of An Individual in Prevention of PollutionSafaaNo ratings yet
- Narrative Solid Waste ManagementDocument3 pagesNarrative Solid Waste ManagementJenyhl Lara Enriquez100% (3)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)