You might also like
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- Chapter 9. Bronchial Asthma: Khaled O Hadeli MD, FCCPDocument19 pagesChapter 9. Bronchial Asthma: Khaled O Hadeli MD, FCCPgireeshsachinNo ratings yet
- The Toxicant Induction of Irritant Asthma, Rhinitis, and Related ConditionsFrom EverandThe Toxicant Induction of Irritant Asthma, Rhinitis, and Related ConditionsNo ratings yet
- Asma Exacerbacioes EpidemiologiaDocument7 pagesAsma Exacerbacioes Epidemiologiahebert ramosNo ratings yet
- Asthma: (Assignment 2)Document8 pagesAsthma: (Assignment 2)nuraNo ratings yet
- Epoc FisiopatologíaDocument10 pagesEpoc FisiopatologíaAndrea Roman chavezNo ratings yet
- Broncoespasmo AsmaDocument9 pagesBroncoespasmo AsmaLUIS FERNANDO GOMEZ CANONo ratings yet
- Consequences of severe asthma exacerbationsDocument7 pagesConsequences of severe asthma exacerbationsteranrobleswaltergabrielNo ratings yet
- Bronchial Asthma GuideDocument59 pagesBronchial Asthma GuideJb TlntinoNo ratings yet
- Medicine Card 2Document4 pagesMedicine Card 2Theodore LiwonganNo ratings yet
- Pa Tho Physiology of AsthmaDocument18 pagesPa Tho Physiology of AsthmaNeil-Vince ConejosNo ratings yet
- Etiology of asthma exacerbationsDocument4 pagesEtiology of asthma exacerbationsVasincuAlexandruNo ratings yet
- Section 2: Diseases of The Respiratory SystemDocument13 pagesSection 2: Diseases of The Respiratory SystemMishael Octaviany JirehNo ratings yet
- Classification of AsthmaDocument4 pagesClassification of AsthmaAlejandro LugoNo ratings yet
- The Common Cold Current Therapy and Natural HistoDocument6 pagesThe Common Cold Current Therapy and Natural HistoNur Wahdania PutriNo ratings yet
- Asthma Patofisiologi 1Document8 pagesAsthma Patofisiologi 1Maulana Aufar Firwanda DriveNo ratings yet
- Childhood Asthma Etiology and EpidemiologyDocument24 pagesChildhood Asthma Etiology and EpidemiologyEstella100% (1)
- SEMINARSKI RAD EnglDocument10 pagesSEMINARSKI RAD EngljuliNo ratings yet
- Asthma in The Primary Care Setting 2019 Medical Clinics of North AmericaDocument18 pagesAsthma in The Primary Care Setting 2019 Medical Clinics of North AmericaYony Morales LeonNo ratings yet
- Estado Asmatico: September 2015Document12 pagesEstado Asmatico: September 2015Jaeline Arleth Macias EscobarNo ratings yet
- AsthmaDocument5 pagesAsthmaabenezer isayasNo ratings yet
- Asma AnestesiaDocument9 pagesAsma AnestesiaGilCasanovaNo ratings yet
- Etiology of AsthmaDocument7 pagesEtiology of AsthmaDoc JT BylnNo ratings yet
- Asthma: Signs and SymptomsDocument7 pagesAsthma: Signs and SymptomsPavitrra SubbramaniyamNo ratings yet
- CRS ASMA - DeaDocument40 pagesCRS ASMA - Deadella srNo ratings yet
- Allergic BronchitisDocument18 pagesAllergic BronchitisTeresa EvansNo ratings yet
- AsthmaDocument118 pagesAsthmaDaroo D.TNo ratings yet
- ASTHMA DIAGNOSIS AND TREATMENT GUIDEDocument4 pagesASTHMA DIAGNOSIS AND TREATMENT GUIDEeverydayisagift9999No ratings yet
- Pulmonary Aspergillosis, What The Generalist Needs To Know - Am J Med 2020Document7 pagesPulmonary Aspergillosis, What The Generalist Needs To Know - Am J Med 2020MICHAEL AMARILLO CORREANo ratings yet
- Relationship Between Asthma and Rhinitis: Epidemiologic, Pathophysiologic, and Therapeutic AspectsDocument7 pagesRelationship Between Asthma and Rhinitis: Epidemiologic, Pathophysiologic, and Therapeutic AspectsStanley SuhermanNo ratings yet
- Asthma 2Document8 pagesAsthma 2Evangelist Stephen NziokaNo ratings yet
- Jurnal CDCDocument9 pagesJurnal CDCPutri WafiroNo ratings yet
- EditorialDocument2 pagesEditorialcarloscano1994No ratings yet
- Chronic Dry Cough in Allergic Respiratory Diseases: Diagnostic and Management ApproachDocument6 pagesChronic Dry Cough in Allergic Respiratory Diseases: Diagnostic and Management ApproachAaron HongreiNo ratings yet
- Asthma and COPD in Alpha 1 Antitrypsin Deficiency Evidence For The Dutch HypothesisDocument10 pagesAsthma and COPD in Alpha 1 Antitrypsin Deficiency Evidence For The Dutch HypothesisMohammed SaleetNo ratings yet
- Sam CD Asthma ReciveredDocument36 pagesSam CD Asthma ReciveredDr. Muha. Hasan Mahbub-Ur-RahmanNo ratings yet
- AsthmaDocument79 pagesAsthmaraj patel100% (1)
- Physical Therapy For Children With ChronDocument11 pagesPhysical Therapy For Children With ChronGauravNo ratings yet
- New Insights Into The Relationship Between Airway Inflammation and AsthmaDocument11 pagesNew Insights Into The Relationship Between Airway Inflammation and Asthmaapi-3736350No ratings yet
- Lepto Spiros IsDocument11 pagesLepto Spiros IsagathageraldyneNo ratings yet
- Bronchial Asthma GuideDocument72 pagesBronchial Asthma GuidePrincewill SeiyefaNo ratings yet
- Bronchial Asthma: Medicine II 5.5Document5 pagesBronchial Asthma: Medicine II 5.5Deann RoscomNo ratings yet
- Asthma: Allergy Asthma and Clinical Immunology November 2011Document10 pagesAsthma: Allergy Asthma and Clinical Immunology November 2011Sarmad AlwardiNo ratings yet
- The Role of Viral Infections in The Natural HistorDocument12 pagesThe Role of Viral Infections in The Natural HistorrepaladavidrajNo ratings yet
- Complications of Allergic Rhinitis: David P. Skoner, MD Pittsburgh, PaDocument5 pagesComplications of Allergic Rhinitis: David P. Skoner, MD Pittsburgh, PawurifreshNo ratings yet
- Aspergiloma 4Document11 pagesAspergiloma 4Nova PurbaNo ratings yet
- Evaluation of Anti-Asthmatic Activity in Animal ModelDocument69 pagesEvaluation of Anti-Asthmatic Activity in Animal ModelShaikh AyyubNo ratings yet
- Chest Radiography Radiographers: An Introduction To For StudentDocument29 pagesChest Radiography Radiographers: An Introduction To For StudentDragan YottNo ratings yet
- Acute Severe AsthmaDocument5 pagesAcute Severe AsthmaRizsa Aulia DanestyNo ratings yet
- Pathophysiological Mechanisms of Asthma: Andrew BushDocument17 pagesPathophysiological Mechanisms of Asthma: Andrew BushDianNo ratings yet
- 4 - AsthmaDocument14 pages4 - AsthmaAmmar AlnajjarNo ratings yet
- AshtmaDocument95 pagesAshtmaObsa JemalNo ratings yet
- ASTHMADocument17 pagesASTHMAvinda astri permatasariNo ratings yet
- "Year of Universalization of Health": I.S.T.P: Course: Especiality: Cycle: Topic: Teacher: StudentDocument8 pages"Year of Universalization of Health": I.S.T.P: Course: Especiality: Cycle: Topic: Teacher: StudentKarina DiazNo ratings yet
- Bronhial AsthmaDocument63 pagesBronhial AsthmaGreeshma Shaji100% (1)
- Definisi AsmaDocument12 pagesDefinisi AsmaDayu Punik ApsariNo ratings yet
- Do Not Copy: Chronic Sinusitis Pathophysiology: The Role of AllergyDocument5 pagesDo Not Copy: Chronic Sinusitis Pathophysiology: The Role of AllergyFaridaHayatiNo ratings yet
- OkanoDocument8 pagesOkanostanleyNo ratings yet
- An Understanding of The Genetic Basis of Asthma: Review ArticleDocument13 pagesAn Understanding of The Genetic Basis of Asthma: Review ArticlerastiooNo ratings yet
- HHS Public Access: Asthma in The Primary Care SettingDocument20 pagesHHS Public Access: Asthma in The Primary Care SettingKarina UtariNo ratings yet
- Ppul 24579Document3 pagesPpul 24579Andi Kumalasari MappaNo ratings yet
- High Dose Antipsychotic Polypharmacy and Dopamine Partial Agonists - Time To Rethink Guidelines?Document7 pagesHigh Dose Antipsychotic Polypharmacy and Dopamine Partial Agonists - Time To Rethink Guidelines?Andi Kumalasari MappaNo ratings yet
- 2023 02 14 Case LeeDocument3 pages2023 02 14 Case LeeAndi Kumalasari MappaNo ratings yet
- Ajpgi 00173 2022Document9 pagesAjpgi 00173 2022Andi Kumalasari MappaNo ratings yet
- Hypertensionaha 120 15026Document24 pagesHypertensionaha 120 15026Andi Kumalasari MappaNo ratings yet
- Dapuz OkDocument6 pagesDapuz OkAndi Kumalasari MappaNo ratings yet
- Cefepime: Ellie Marie F. Royales - PH-3ADocument10 pagesCefepime: Ellie Marie F. Royales - PH-3AEllie Marie RoyalesNo ratings yet
- Ophthalmology Review Manual 2nd EditionDocument538 pagesOphthalmology Review Manual 2nd EditionAnonymous 4OnqyBErNo ratings yet
- Anxiety Disorders: Powerpoint Lecture Notes PresentationDocument43 pagesAnxiety Disorders: Powerpoint Lecture Notes PresentationErsido SamuelNo ratings yet
- PTB Case-StudyDocument64 pagesPTB Case-StudyBeverly DatuNo ratings yet
- Mrunal Emotional Intelligence:Meaning, Benefits, Models, Case StudiesDocument8 pagesMrunal Emotional Intelligence:Meaning, Benefits, Models, Case StudiesPrateek BayalNo ratings yet
- ACHAI DLaboratory Actiivty 11 - The HeartDocument6 pagesACHAI DLaboratory Actiivty 11 - The HeartSYDNEY JILL ACHAINo ratings yet
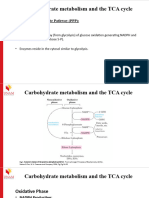
- Carbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Document17 pagesCarbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Frolian MichaelNo ratings yet
- Chapter 25 - Acquired Conditions and CongenitalDocument6 pagesChapter 25 - Acquired Conditions and CongenitalEunice CortésNo ratings yet
- Segamat District Muet Final Year Lower 6 Exam-Govin2Document20 pagesSegamat District Muet Final Year Lower 6 Exam-Govin2govinjementah100% (1)
- ACEM PostersDocument2 pagesACEM PostersDr.KHAJA SHAFIUDDINNo ratings yet
- Document - Isk ..Document8 pagesDocument - Isk ..Karyn GloriaNo ratings yet
- Memory Reconsolidation Applied - Calm Your Past To Live Your FutureDocument177 pagesMemory Reconsolidation Applied - Calm Your Past To Live Your Futureiskieh100% (7)
- Articulo Receptor H4Document12 pagesArticulo Receptor H4anaNo ratings yet
- Gram Positive Cocci Bacteriology ChartDocument2 pagesGram Positive Cocci Bacteriology ChartIsabella CeaNo ratings yet
- Desiree Anggia LAPAKHIR2021 DrDesiree DosenMuda KedokteranDocument48 pagesDesiree Anggia LAPAKHIR2021 DrDesiree DosenMuda KedokteranWahyu IndraNo ratings yet
- Sample of Journal & Critique PresenationDocument42 pagesSample of Journal & Critique PresenationMonika shankarNo ratings yet
- Maintaining Homeostasis: The Coordinated Functions of the Nervous and Endocrine SystemsDocument15 pagesMaintaining Homeostasis: The Coordinated Functions of the Nervous and Endocrine SystemsZahra Alexä DavidsonNo ratings yet
- Issam Abouliatim, MDDocument19 pagesIssam Abouliatim, MDNaser Hamdi ZalloumNo ratings yet
- Air PollutionDocument5 pagesAir PollutionDiane AbsalonNo ratings yet
- Α Α Α Α-Amylase-Eps: Biosystems S.ADocument1 pageΑ Α Α Α-Amylase-Eps: Biosystems S.ARisqon Anjahiranda AdiputraNo ratings yet
- Human Skeleton NotesDocument29 pagesHuman Skeleton NotesSoumyajit DasNo ratings yet
- HOAXESDocument2 pagesHOAXESRovelyn S DupraNo ratings yet
- C Difficile SporesDocument3 pagesC Difficile SporesEda SopNo ratings yet
- Drug Education, Prevention and ControlDocument18 pagesDrug Education, Prevention and ControlMaurene MendozaNo ratings yet
- VBMC Heparin Protocol FINAL May2004Document3 pagesVBMC Heparin Protocol FINAL May2004Pharmacy OneSource100% (1)
- Artigo ApoioDocument11 pagesArtigo ApoioNayanne CunhaNo ratings yet
- Recommendations For The Use of Immunoglobulin Therapy For Immunomodulation and Antibody ReplacementDocument7 pagesRecommendations For The Use of Immunoglobulin Therapy For Immunomodulation and Antibody ReplacementChih-I LeeNo ratings yet
- 14th Forum Program Rundown Final v2Document2 pages14th Forum Program Rundown Final v2Ray Li Shing KitNo ratings yet
- Insulin MinDocument23 pagesInsulin MinLukasNo ratings yet
- 17 Effective Ways To Lower Your Blood PressureDocument9 pages17 Effective Ways To Lower Your Blood PressureRani AndréNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)