You might also like
- Vitamin Water - Arnel Ricafranca PDFDocument32 pagesVitamin Water - Arnel Ricafranca PDFAlaa EssamNo ratings yet
- BlsDocument62 pagesBlspaediatrica89% (19)
- Insurance Fraud PPT (Final)Document30 pagesInsurance Fraud PPT (Final)Gaurav Savlani83% (6)
- Acute Complications of Diabetes MellitusDocument1 pageAcute Complications of Diabetes MellitusGerardLum100% (1)
- Small-Sided Games and Integrating Physical PreparationDocument196 pagesSmall-Sided Games and Integrating Physical Preparationbolebs1475% (4)
- Lactose Intolerance Among Severely Malnourished Children With Diarrhoea Admitted To The Nutrition Unit, Mulago Hospital, UgandaDocument10 pagesLactose Intolerance Among Severely Malnourished Children With Diarrhoea Admitted To The Nutrition Unit, Mulago Hospital, UgandaSuci Joe ArmstrongNo ratings yet
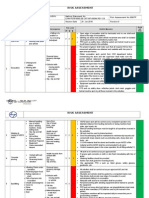
- Hse Risk Assessment - 006 Ra - Hdpe Duct LayingDocument7 pagesHse Risk Assessment - 006 Ra - Hdpe Duct Layingbinunalukandam83% (12)
- Change Your Life in 7 Days With NLP - Paul Mckenna BrochureDocument2 pagesChange Your Life in 7 Days With NLP - Paul Mckenna Brochureapi-385316675% (4)
- Question and AnswerDocument4 pagesQuestion and AnswerShaf AbubakarNo ratings yet
- CPG AID - Pocket Guide.v7 PDFDocument31 pagesCPG AID - Pocket Guide.v7 PDFR ParkNo ratings yet
- SpitzDocument30 pagesSpitzprabhatNo ratings yet
- Toddler's Diarrhea: Is It An Under-Recognized Entity in Developing Countries?Document6 pagesToddler's Diarrhea: Is It An Under-Recognized Entity in Developing Countries?deonardNo ratings yet
- Efficacy of Probiotics in Acute Diarrhoea in Children: Original Research ArticleDocument5 pagesEfficacy of Probiotics in Acute Diarrhoea in Children: Original Research ArticledwimellyndaNo ratings yet
- Paediatrica Indonesiana: Teny Tjitrasari, MD Agus Firmansyah, MD, PHD Imral Chair, MDDocument7 pagesPaediatrica Indonesiana: Teny Tjitrasari, MD Agus Firmansyah, MD, PHD Imral Chair, MDakreditasi rsunhNo ratings yet
- Prolonged Acute Diarrhea in Adults: Decades of Observation From Epidemiological Perspective in Urban BangladeshDocument7 pagesProlonged Acute Diarrhea in Adults: Decades of Observation From Epidemiological Perspective in Urban BangladeshDefi MerisaNo ratings yet
- Saccharomyces boulardii May Shorten Diarrhea in ChildrenDocument5 pagesSaccharomyces boulardii May Shorten Diarrhea in ChildrenShankar YadavNo ratings yet
- Efficacy of Zinc Therapy in Acute Diarrhea in ChilDocument4 pagesEfficacy of Zinc Therapy in Acute Diarrhea in ChilKusuma IntanNo ratings yet
- Journal Reading Diare - Dea DickytaDocument7 pagesJournal Reading Diare - Dea DickytaDea DickytaNo ratings yet
- Clinical Profile of Functional Constipation in ChildrenDocument4 pagesClinical Profile of Functional Constipation in ChildrenIJAR JOURNALNo ratings yet
- The Clinical Spectrum of Chronic Diarrhea in ChildrenDocument15 pagesThe Clinical Spectrum of Chronic Diarrhea in ChildrenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Askep KomplementerDocument14 pagesAskep KomplementernatiyaNo ratings yet
- 1 s2.0 S168719792100040X MainDocument4 pages1 s2.0 S168719792100040X MainfelipetheNo ratings yet
- Pattern of Acute Parasitic Diarrhea in Children Under Five Years of Age in Kathmandu, NepalDocument6 pagesPattern of Acute Parasitic Diarrhea in Children Under Five Years of Age in Kathmandu, NepalDaniel EvansNo ratings yet
- Diare Rotavirus Pada Anak Dibawah Usia 3 Tahun Yang Dirawat Di Rsu Dr. Saiful Anwar Malang Tahun 2005 (Preliminary Study)Document3 pagesDiare Rotavirus Pada Anak Dibawah Usia 3 Tahun Yang Dirawat Di Rsu Dr. Saiful Anwar Malang Tahun 2005 (Preliminary Study)Lala SyahaabNo ratings yet
- As URO Disfunção InfantilDocument5 pagesAs URO Disfunção InfantilKelvin CelliNo ratings yet
- Cochrane BVS: Oral Zinc For Treating Diarrhoea in ChildrenDocument25 pagesCochrane BVS: Oral Zinc For Treating Diarrhoea in ChildrenLaura AnguloNo ratings yet
- Lactose Intolerance Among Severely Malnourished Children With Diarrhoea Admitted To The Nutrition Unit, Mulago Hospital, UgandaDocument9 pagesLactose Intolerance Among Severely Malnourished Children With Diarrhoea Admitted To The Nutrition Unit, Mulago Hospital, UgandaArsy Mira PertiwiNo ratings yet
- Hubungan Diare Dengan Status Gizi Pada Balita Di Rumah Sakit Umum Daerah Dr. H. Chasan BoesoirieDocument6 pagesHubungan Diare Dengan Status Gizi Pada Balita Di Rumah Sakit Umum Daerah Dr. H. Chasan BoesoirieRippie RifdahNo ratings yet
- Jurnal AnakDocument7 pagesJurnal AnakNurul SahanaNo ratings yet
- Dokumen Tanpa JudulDocument10 pagesDokumen Tanpa JudulZakia AmeliaNo ratings yet
- Hubungan Pengetahuan Ibu Tentang Hygiene Makanan dan Diare pada BalitaDocument6 pagesHubungan Pengetahuan Ibu Tentang Hygiene Makanan dan Diare pada BalitaKoco Totok SugiartoNo ratings yet
- Natural evolution of regurgitation in children aged 12-24 monthsDocument6 pagesNatural evolution of regurgitation in children aged 12-24 monthsTianKaunangNo ratings yet
- HUBUNGAN SANITASI LINGKUNGAN DAN PERILAKU HIDUP BERSIH SEHAT DENGAN KEJADIAN DIARE PADA BALITADocument19 pagesHUBUNGAN SANITASI LINGKUNGAN DAN PERILAKU HIDUP BERSIH SEHAT DENGAN KEJADIAN DIARE PADA BALITAjumowoNo ratings yet
- Spectrum of Dysentery in Children Presenting To A Tertiary Level Teaching Hospital in New DelhiDocument5 pagesSpectrum of Dysentery in Children Presenting To A Tertiary Level Teaching Hospital in New DelhiNasNo ratings yet
- Influence of Nutritional Status On Clinical Outcomes in Critically Ill ChildrenDocument5 pagesInfluence of Nutritional Status On Clinical Outcomes in Critically Ill ChildrenAnonymous h0DxuJTNo ratings yet
- Influence of Nutritional Status On Clinical Outcomes in Critically Ill ChildrenDocument5 pagesInfluence of Nutritional Status On Clinical Outcomes in Critically Ill ChildrenIvana YunitaNo ratings yet
- 12933-Article Text-16095-1-10-20191208Document11 pages12933-Article Text-16095-1-10-20191208jaskiran kaurNo ratings yet
- Prevalence of Diarrhea and Malnutrition in Bangladeshi ChildrenDocument6 pagesPrevalence of Diarrhea and Malnutrition in Bangladeshi ChildrenSukmaNo ratings yet
- Analisis Jurnal Pico GeaDocument3 pagesAnalisis Jurnal Pico GeaMuhammad Robi Al BanjariNo ratings yet
- Submit Ijbs EditedDocument10 pagesSubmit Ijbs Editedpuannita santosoNo ratings yet
- Bacillus Clausii As An Adjuvant Therapy in Acute Childhood DiarrhoeaDocument3 pagesBacillus Clausii As An Adjuvant Therapy in Acute Childhood DiarrhoeaIOSRjournalNo ratings yet
- Nutritional Assessment of Children Admitted at The Children'S Ward of The Volta Regional HospitalDocument10 pagesNutritional Assessment of Children Admitted at The Children'S Ward of The Volta Regional HospitalClifford AfuNo ratings yet
- PrognosisDocument7 pagesPrognosispenyimpanankoas8No ratings yet
- PBL 2 KedkelDocument7 pagesPBL 2 KedkelDanindNo ratings yet
- Investigating Key Determinants of Childhood Diarrheal Incidence Among Patients at Hoima Regional Referral Hospital, Western UgandaDocument14 pagesInvestigating Key Determinants of Childhood Diarrheal Incidence Among Patients at Hoima Regional Referral Hospital, Western UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Synopsis Edited 3 - 073650 PDFDocument7 pagesSynopsis Edited 3 - 073650 PDFMohammad ShafiqNo ratings yet
- Comparison of Body Mass Index On Children With Functional Constipation and Healthy ControlsDocument5 pagesComparison of Body Mass Index On Children With Functional Constipation and Healthy ControlsGita TrisnawatiNo ratings yet
- 404 398 1 SMDocument4 pages404 398 1 SMfak youNo ratings yet
- Probiotics in Adolescent Prediabetes: A Pilot RCT On Glycemic Control and Intestinal BacteriomeDocument14 pagesProbiotics in Adolescent Prediabetes: A Pilot RCT On Glycemic Control and Intestinal BacteriomeKarina EkawidyaniNo ratings yet
- Jtstikesmuhgo GDL Wiwinpujia 1337 2 Hal.151 8Document8 pagesJtstikesmuhgo GDL Wiwinpujia 1337 2 Hal.151 8Bayou Fore YouNo ratings yet
- Electronic Physician (ISSN: 2008-5842)Document5 pagesElectronic Physician (ISSN: 2008-5842)Aldian DianNo ratings yet
- Acute Pyelonephritis in PregnancyDocument7 pagesAcute Pyelonephritis in PregnancyKvmLlyNo ratings yet
- Journal GastroenteritisDocument4 pagesJournal GastroenteritisRian KurniawanNo ratings yet
- Nutritional Assessment of Children With CHD CompareDocument9 pagesNutritional Assessment of Children With CHD CompareIntan Robi'ahNo ratings yet
- RCT Finds Gelatine Tannate Ineffective for Childhood GastroenteritisDocument39 pagesRCT Finds Gelatine Tannate Ineffective for Childhood Gastroenteritiszaky ariandyNo ratings yet
- 2305Document3 pages2305HelenCandyNo ratings yet
- 5 PBDocument5 pages5 PBluciaNo ratings yet
- Etiology of Acute Diarrhea in ChildrenDocument5 pagesEtiology of Acute Diarrhea in ChildrenZazaNo ratings yet
- Protective Effect of Breast Milk On Urinary Tract Infection in Children Aged 0-3 YearsDocument5 pagesProtective Effect of Breast Milk On Urinary Tract Infection in Children Aged 0-3 YearsChika FebrianiNo ratings yet
- Paediatric Appendicitis Scoring: A Useful Guide To Diagnose Acute Appendicitis in ChildrenDocument6 pagesPaediatric Appendicitis Scoring: A Useful Guide To Diagnose Acute Appendicitis in ChildrenFebrian Naranggi Aradia PutraNo ratings yet
- Knowledge Level and Determinants of Neonatal Jaundice A Cross-Sectional Study in The Effutu Municipality of GhanaDocument10 pagesKnowledge Level and Determinants of Neonatal Jaundice A Cross-Sectional Study in The Effutu Municipality of GhananicloverNo ratings yet
- E377 FullDocument6 pagesE377 FullBerliana SitanggangNo ratings yet
- Risk Correlates of Diarrhea in Children Under 5 Years of Age in Slums of Bankura, West BengalDocument8 pagesRisk Correlates of Diarrhea in Children Under 5 Years of Age in Slums of Bankura, West BengalSanaNo ratings yet
- Effect of diarrhea management at home on parents' knowledge and skillsDocument7 pagesEffect of diarrhea management at home on parents' knowledge and skillsCut Qurrata A'yunNo ratings yet
- Gastrointestinal Flora and Gastrointestinal Status in Children With Autism - Comparisons To Typical Children and Correlation With Autism SeverityDocument14 pagesGastrointestinal Flora and Gastrointestinal Status in Children With Autism - Comparisons To Typical Children and Correlation With Autism SeverityapriliaNo ratings yet
- Scholl Hammer 2015Document7 pagesScholl Hammer 2015jesslynNo ratings yet
- Estreñimiento y TeaDocument9 pagesEstreñimiento y TeaElena Martin LopezNo ratings yet
- Tannuri 2016Document5 pagesTannuri 2016sytaNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- BPN Datangi MalaysiaDocument62 pagesBPN Datangi MalaysiaafandianddonkeyNo ratings yet
- Otto Chemie PVT LTD: Material Safety Data SheetDocument4 pagesOtto Chemie PVT LTD: Material Safety Data Sheetenes duhanNo ratings yet
- SIP Physical SCiDocument8 pagesSIP Physical SCiShane Catherine BesaresNo ratings yet
- UG MaharashtraNationalLawUniversityMNLUMumbaiDocument5 pagesUG MaharashtraNationalLawUniversityMNLUMumbaiArpan KushwahaNo ratings yet
- Unilag MSC Environmenatl Toxicology SampleDocument4 pagesUnilag MSC Environmenatl Toxicology SamplebdianNo ratings yet
- City of Peterborough 2023 Draft Capital BudgetDocument535 pagesCity of Peterborough 2023 Draft Capital BudgetPeterborough ExaminerNo ratings yet
- IELTS-Style Speaking Test Questions and Answers SportDocument4 pagesIELTS-Style Speaking Test Questions and Answers SportĐại Học Ôn ThiNo ratings yet
- MSDSDocument3 pagesMSDSSiti Nurjanah SeptianiNo ratings yet
- Theory Critique of Boundaries in MarriageDocument8 pagesTheory Critique of Boundaries in MarriagepatrickakingNo ratings yet
- Grain Legumes/Pulses Introduction and ImportanceDocument5 pagesGrain Legumes/Pulses Introduction and ImportancesumandhakalNo ratings yet
- Types of Solder FluxDocument6 pagesTypes of Solder Fluxpeter paulNo ratings yet
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- Empowering Women Key to Ending PovertyDocument25 pagesEmpowering Women Key to Ending PovertydassmbaNo ratings yet
- Chapt01 The Sudy of ChangeDocument34 pagesChapt01 The Sudy of ChangeIkhsan Abdul HanifNo ratings yet
- A Comparative Study of The Efficacy of Cedarwood Oil, Coconut Oil and Dish Wash Liquid As Alternatives To Xylene As Deparaffinizing AgentsDocument98 pagesA Comparative Study of The Efficacy of Cedarwood Oil, Coconut Oil and Dish Wash Liquid As Alternatives To Xylene As Deparaffinizing AgentszzzzNo ratings yet
- KPJ Pasir Gudang Covid Test ReportDocument1 pageKPJ Pasir Gudang Covid Test ReportNooh DinNo ratings yet
- Product SelectionDocument5 pagesProduct Selectionemmanuelgk100No ratings yet
- Cricket Academy Head Coach RoleDocument4 pagesCricket Academy Head Coach Roletauseef1716No ratings yet
- Autoimmune HepatitisDocument3 pagesAutoimmune HepatitisMohammed FaragNo ratings yet
- Maynilad Valenzuela Sewerage Project Environmental ReportDocument297 pagesMaynilad Valenzuela Sewerage Project Environmental ReportmarvilouNo ratings yet
- Apply teacher short leaveDocument1 pageApply teacher short leaveJean Claudine MandayNo ratings yet