You might also like
- Post Polypectomy Electrocoagulation Syndrome A Rare Cause of Acute Abdominal PainDocument5 pagesPost Polypectomy Electrocoagulation Syndrome A Rare Cause of Acute Abdominal PainCom DigfulNo ratings yet
- Hematochezia Case Report on Crohn's Disease in Young MaleDocument3 pagesHematochezia Case Report on Crohn's Disease in Young Maleseptian_tjayaNo ratings yet
- Hiding in The Water: Clinical Problem-SolvingDocument6 pagesHiding in The Water: Clinical Problem-SolvingtabareeNo ratings yet
- Colonoscopy Induced Ischemic Colitis: An Endoscopic and Histological AssayDocument3 pagesColonoscopy Induced Ischemic Colitis: An Endoscopic and Histological AssayArfania LailyNo ratings yet
- Residents' Clinic: 22-Year-Old Man With Abdominal Pain and RashDocument4 pagesResidents' Clinic: 22-Year-Old Man With Abdominal Pain and RashAkhtar AliNo ratings yet
- Intestinal Tuberculosis: A Diagnostic Challenge: Open Access Case DOI: 10.7759/cureus.13058Document4 pagesIntestinal Tuberculosis: A Diagnostic Challenge: Open Access Case DOI: 10.7759/cureus.13058ATIKA INDAH SARINo ratings yet
- Life-Threatening Lower Gastrointestinal Hemorrhage in Pediatric Crohn's DiseaseDocument8 pagesLife-Threatening Lower Gastrointestinal Hemorrhage in Pediatric Crohn's DiseasePeregrine Albertus Ricco AzaliNo ratings yet
- Potential Role of Thermography in Evaluation of Disease Activity in Inflammatory Bowel Disease A Case ReportDocument3 pagesPotential Role of Thermography in Evaluation of Disease Activity in Inflammatory Bowel Disease A Case ReportChristian MarchiNo ratings yet
- Pi Is 0016508500545053Document5 pagesPi Is 0016508500545053Abdullah KhanNo ratings yet
- Pi Is 0016508500545053Document5 pagesPi Is 0016508500545053Abdullah KhanNo ratings yet
- Poliadenitis NodosaDocument5 pagesPoliadenitis NodosaRicardo Uzcategui ArreguiNo ratings yet
- Inflammatory Bowel DiseaseDocument41 pagesInflammatory Bowel DiseaseAbdul hadiNo ratings yet
- Typhoid Fever Case Presenting with Multiple ComplicationsDocument4 pagesTyphoid Fever Case Presenting with Multiple ComplicationsCleo CaminadeNo ratings yet
- Severe Systemic Cytomegalovirus Infection in An Immunocompetent Patient Outside The Intensive Care Unit: A Case ReportDocument4 pagesSevere Systemic Cytomegalovirus Infection in An Immunocompetent Patient Outside The Intensive Care Unit: A Case ReportSebastián Garay HuertasNo ratings yet
- Case Report: Streptococcus AnginosusDocument4 pagesCase Report: Streptococcus AnginosusIesanu MaraNo ratings yet
- Jha2 2 118Document3 pagesJha2 2 118Renato DantasNo ratings yet
- What Is The Gastrointestinal Tract?: Ulcerative Colitis Microscopic Colitis: Collagenous Colitis and Lymphocytic ColitisDocument16 pagesWhat Is The Gastrointestinal Tract?: Ulcerative Colitis Microscopic Colitis: Collagenous Colitis and Lymphocytic ColitissakuraleeshaoranNo ratings yet
- Granulomatous Appendicitis in A 12-Year-Old Boy: Derya Yayla, Bedriye Nuray Alpman, Yasemin DolekDocument3 pagesGranulomatous Appendicitis in A 12-Year-Old Boy: Derya Yayla, Bedriye Nuray Alpman, Yasemin Dolekansar ahmedNo ratings yet
- Amj 23 2 235 240Document7 pagesAmj 23 2 235 240Czar Alexis FernandezNo ratings yet
- Klebsiella Pneumoniae Case ReportDocument3 pagesKlebsiella Pneumoniae Case ReportMaria Chacón CarbajalNo ratings yet
- Upadacitinib Treatment Improves Symptoms of Bowel Urgency and Abdominal Pain, and Correlates With Quality of Life Improvements in Patients With Moderate To Severe Ulcerative ColitisDocument9 pagesUpadacitinib Treatment Improves Symptoms of Bowel Urgency and Abdominal Pain, and Correlates With Quality of Life Improvements in Patients With Moderate To Severe Ulcerative Colitisslt.hi468No ratings yet
- Hematemesis Melena Due To Helicobacter Pylori Infection in Duodenal Ulcer: A Case Report and Literature ReviewDocument6 pagesHematemesis Melena Due To Helicobacter Pylori Infection in Duodenal Ulcer: A Case Report and Literature ReviewodiNo ratings yet
- s12887 021 02814 WDocument6 pagess12887 021 02814 WNovi OktaviantiNo ratings yet
- Managing IBD: A Case Study on Diagnosis and TreatmentDocument4 pagesManaging IBD: A Case Study on Diagnosis and TreatmentBejan CorinaNo ratings yet
- EMQs For Medical Students Volume 2 2eDocument30 pagesEMQs For Medical Students Volume 2 2ePasTestBooks50% (2)
- 1471 230X 12 174 PDFDocument5 pages1471 230X 12 174 PDFAila HinlogNo ratings yet
- Gastrointestinal Symptoms As The First Manifestation of Antiphospholipid SyndromeDocument5 pagesGastrointestinal Symptoms As The First Manifestation of Antiphospholipid SyndromeGraikos KonstantinosNo ratings yet
- 19Document3 pages19Elizabeth ToapantaNo ratings yet
- Esophageal Ulcers Associated With Ulcerative Colitis: A Case Series and Literature ReviewDocument7 pagesEsophageal Ulcers Associated With Ulcerative Colitis: A Case Series and Literature ReviewHendro GunawanNo ratings yet
- TOGADO - SEVERE PERITONITIS (Disorder Analysis and NCP)Document10 pagesTOGADO - SEVERE PERITONITIS (Disorder Analysis and NCP)John Paul TogadoNo ratings yet
- Acute Mesenteric Ischemia in COVID19 Patient - NAT FixedDocument10 pagesAcute Mesenteric Ischemia in COVID19 Patient - NAT FixedAde Tan RezaNo ratings yet
- Dafpus LiverDocument2 pagesDafpus LiverMenda JangWooyoung SooyoungsterNo ratings yet
- Hematemesis Melena Due To Helicobacter Pylori Infection in Duodenal Ulcer: A Case Report and Literature ReviewDocument6 pagesHematemesis Melena Due To Helicobacter Pylori Infection in Duodenal Ulcer: A Case Report and Literature ReviewWahyu Agung PribadiNo ratings yet
- Abcesele FicatuluiDocument4 pagesAbcesele FicatuluiMihaela AlinaNo ratings yet
- Pediatric Round PneumoniaDocument4 pagesPediatric Round PneumoniaSalwa Zahra TsamaraNo ratings yet
- Awuku 1552016 BJMMR26166Document4 pagesAwuku 1552016 BJMMR26166Kush GuptaNo ratings yet
- Gastrite Enfisematosa - InglêsDocument7 pagesGastrite Enfisematosa - Inglêsamanda.gomesNo ratings yet
- Acute PancreatitisDocument10 pagesAcute PancreatitisHarbin NicholsonNo ratings yet
- Colonoscopy Is Mandatory AfterDocument3 pagesColonoscopy Is Mandatory AfterLaurice BarronNo ratings yet
- Jurnal Literatur Case Series 1Document4 pagesJurnal Literatur Case Series 1Debby LadadoNo ratings yet
- Jejunojejunal Intussusception As Initial Presentation of Coeliac Disease: A Case Report and Review of LiteratureDocument6 pagesJejunojejunal Intussusception As Initial Presentation of Coeliac Disease: A Case Report and Review of Literatureellya theresiaNo ratings yet
- Coeliac Disease: John S. Leeds, Andrew D. Hopper, and David S. SandersDocument14 pagesCoeliac Disease: John S. Leeds, Andrew D. Hopper, and David S. Sandersbdalcin5512No ratings yet
- Ojsadmin, 1032Document4 pagesOjsadmin, 1032Jade CentinoNo ratings yet
- Abdominal Aortic Aneurysm and Gas in The Kidney inDocument2 pagesAbdominal Aortic Aneurysm and Gas in The Kidney inniluh suwasantiNo ratings yet
- Liver Abscess DissertationDocument4 pagesLiver Abscess DissertationPayForAPaperAtlanta100% (1)
- Ischemic Colitis: A Clinical Case and Concise ReviewDocument15 pagesIschemic Colitis: A Clinical Case and Concise ReviewDevi AmaraNo ratings yet
- Corrosive InjuryDocument6 pagesCorrosive InjuryCristian O. Saavedra RodriguezNo ratings yet
- Revista Gastroenterologia Mexico: Scientific LetterDocument4 pagesRevista Gastroenterologia Mexico: Scientific LetterPriyanshu SinghNo ratings yet
- Acute Surgical Abdomen: Unexpected Medical CauseDocument6 pagesAcute Surgical Abdomen: Unexpected Medical CauseIJAR JOURNALNo ratings yet
- Cistitis Enfosematosa 2020Document4 pagesCistitis Enfosematosa 2020alejandro montesNo ratings yet
- An Unusual Cause of Acute Abdomend Gas-Forming Liver Abscess Due To Salmonella EnteritidisDocument4 pagesAn Unusual Cause of Acute Abdomend Gas-Forming Liver Abscess Due To Salmonella EnteritidisMenda JangWooyoung SooyoungsterNo ratings yet
- 1534 5952 1 PBDocument4 pages1534 5952 1 PBUparsariya Pratik Sureshbhai (Student BSMU. Chernivtsi)No ratings yet
- A Rare Case Report of Spontaneous Resolution of Hepatic Portal Venous Gas Associated With Cocaineinduced Intestinal IschDocument3 pagesA Rare Case Report of Spontaneous Resolution of Hepatic Portal Venous Gas Associated With Cocaineinduced Intestinal IschShiva PNo ratings yet
- Multiple Liver Abscess Case ReportDocument5 pagesMultiple Liver Abscess Case ReportRizki HardianNo ratings yet
- GI Summer Review - Answers - Bosch (2013)Document16 pagesGI Summer Review - Answers - Bosch (2013)Jessica MooreNo ratings yet
- Enzymes in Feces: Useful Markers of Chronic Inflammatory Bowel DiseaseDocument6 pagesEnzymes in Feces: Useful Markers of Chronic Inflammatory Bowel DiseaseyostiNo ratings yet
- Signs, Symptoms and Treatment of AppendicitisDocument14 pagesSigns, Symptoms and Treatment of AppendicitisMary Joy BunuanNo ratings yet
- A Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportDocument4 pagesA Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportAbdullah KhanNo ratings yet
- Atlas of Inflammatory Bowel DiseasesFrom EverandAtlas of Inflammatory Bowel DiseasesWon Ho KimNo ratings yet
- Colitis: A Practical Approach to Colon and Ileum Biopsy InterpretationFrom EverandColitis: A Practical Approach to Colon and Ileum Biopsy InterpretationAnne Jouret-MourinNo ratings yet
- 13 Bittner Improve Visual Function CeDocument33 pages13 Bittner Improve Visual Function CeLija LajiNo ratings yet
- 200510-Article Text-503222-1-10-20201014Document7 pages200510-Article Text-503222-1-10-20201014BONGO John Ryan C.No ratings yet
- CPT Codes: Hepatitis CDocument2 pagesCPT Codes: Hepatitis CAnasNo ratings yet
- New Apollo Lab Standards Range Unit InferenceDocument1 pageNew Apollo Lab Standards Range Unit InferenceBhargavaNo ratings yet
- Abbreviations & Acronyms MeaningDocument15 pagesAbbreviations & Acronyms MeaningNathaniel PulidoNo ratings yet
- Ijsid: International Journal of Science Innovations and DiscoveriesDocument9 pagesIjsid: International Journal of Science Innovations and DiscoveriesijsidonlineinfoNo ratings yet
- IDEXX CBC Chem ExplainedDocument38 pagesIDEXX CBC Chem Explainedmmatthew74No ratings yet
- 5.01 Liver Function Test Plenary: OutlineDocument6 pages5.01 Liver Function Test Plenary: OutlineManila MedNo ratings yet
- St. Alexius College, Inc.: Clinic Chemistry 2 Laboratory ManualDocument91 pagesSt. Alexius College, Inc.: Clinic Chemistry 2 Laboratory ManualHasmyra C. Nul ÜNo ratings yet
- Doctor's orders and rationaleDocument4 pagesDoctor's orders and rationaleJes Cristy LindonganNo ratings yet
- Approach To Abnormal Liver Enzymes Whitepaper TI 07106Document6 pagesApproach To Abnormal Liver Enzymes Whitepaper TI 07106luceroNo ratings yet
- Activity 17 Clinical ChemistryDocument53 pagesActivity 17 Clinical ChemistryKendrix Aguiluz FlorendoNo ratings yet
- Buffalo Bulletin (September 2014) Vol.33 No.3Document113 pagesBuffalo Bulletin (September 2014) Vol.33 No.3AngelNo ratings yet
- Abnormal Liver Function TestsDocument6 pagesAbnormal Liver Function Testskronic12daniNo ratings yet
- Ontarget Results April 2008 FinalDocument20 pagesOntarget Results April 2008 Finalyona selvia ariesNo ratings yet
- Viral Hepatitis Case Semi FinalDocument73 pagesViral Hepatitis Case Semi FinalLOIS DANIELLE REYESNo ratings yet
- Issue03 41 20220Document8 pagesIssue03 41 20220NealNo ratings yet
- 9321 3357 - Basanti JenaDocument4 pages9321 3357 - Basanti JenaRodrigo Rodrigues S AlmeidaNo ratings yet
- Reference RangesDocument3 pagesReference RangesA.h.MuradNo ratings yet
- Reagents Brochure LT314 MAR20Document80 pagesReagents Brochure LT314 MAR20Yousra ZeidanNo ratings yet
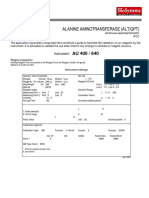
- Alanine Aminotransferase (Alt/Gpt) : InstrumentDocument1 pageAlanine Aminotransferase (Alt/Gpt) : InstrumentEnrique DuarteNo ratings yet
- Jaundice in The Adult PatientDocument11 pagesJaundice in The Adult PatientAdhytya Pratama AhmadiNo ratings yet
- Rhabdomyolysis: Dana BartlettDocument35 pagesRhabdomyolysis: Dana BartlettYousef JafarNo ratings yet
- LAB REPORT INSIGHTSDocument3 pagesLAB REPORT INSIGHTSHarshitNo ratings yet
- Mindray BS200E User ManualDocument6 pagesMindray BS200E User ManualMichael OkekeNo ratings yet
- Complete Urine Examination (CUE), Urine: MR.P V Rama RaoDocument19 pagesComplete Urine Examination (CUE), Urine: MR.P V Rama RaoGautam PendyalaNo ratings yet
- Animal Clinical ChemistryDocument231 pagesAnimal Clinical ChemistryAngel GarciaNo ratings yet
- LFT (Liver Function Test) : Biological Reference Results Units Test NameDocument4 pagesLFT (Liver Function Test) : Biological Reference Results Units Test Namemetepraju0210No ratings yet
- Pre EclampsiaDocument179 pagesPre EclampsiaAnton RossiniNo ratings yet
- Lyphochek Assayed Chemistry Control Levels 1 and 2: Erba XL SeriesDocument2 pagesLyphochek Assayed Chemistry Control Levels 1 and 2: Erba XL SeriesMDD EngineeringNo ratings yet