You might also like
- PDF 17267541 1585740752603Document7 pagesPDF 17267541 1585740752603Lucky TraderNo ratings yet
- PDF 17145960 1585132385521 PDFDocument7 pagesPDF 17145960 1585132385521 PDFLucky TraderNo ratings yet
- PDF 17057717 1584487025791 PDFDocument7 pagesPDF 17057717 1584487025791 PDFLucky TraderNo ratings yet
- HDFC ERGO General Insurance Company LimitedDocument5 pagesHDFC ERGO General Insurance Company LimitedChiranjib PatraNo ratings yet
- Intermediary Name:Direct Code: NIL Contact Number: NILDocument4 pagesIntermediary Name:Direct Code: NIL Contact Number: NILniren4u1567No ratings yet
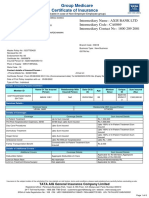
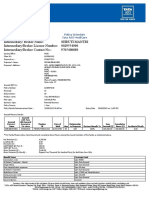
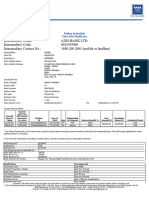
- Group Medicare Certificate of InsuranceDocument8 pagesGroup Medicare Certificate of InsuranceArindam senNo ratings yet
- PDF 17209503 1585132469545 PDFDocument7 pagesPDF 17209503 1585132469545 PDFLucky TraderNo ratings yet
- PDF 16916777 1584486465302 PDFDocument8 pagesPDF 16916777 1584486465302 PDFLucky TraderNo ratings yet
- PDF 16900547 1584487082104 PDFDocument7 pagesPDF 16900547 1584487082104 PDFLucky TraderNo ratings yet
- Schedule of BenefitsDocument1 pageSchedule of BenefitsParthiban RNo ratings yet
- MediclaimDocument3 pagesMediclaimPrajwal ShettyNo ratings yet
- PolicyDocument55 pagesPolicyBaneNo ratings yet
- My Insurance PolicyDocument7 pagesMy Insurance PolicyMuntaj BegumNo ratings yet
- Intermediary/ Broker Name: Intermediary/Broker License Number: Intermediary/Broker Contact No.: Shruti Mantri 0029554000 9765408680Document12 pagesIntermediary/ Broker Name: Intermediary/Broker License Number: Intermediary/Broker Contact No.: Shruti Mantri 0029554000 9765408680dipesh goudNo ratings yet
- 3 HanaDocument1 page3 HanaHimalayan MandererNo ratings yet
- Certificate of Insurance (COI) - Health PlusDocument5 pagesCertificate of Insurance (COI) - Health PlusSawan PaulNo ratings yet
- L L L L L: Customer AppDocument8 pagesL L L L L: Customer App879manjunath879No ratings yet
- 19172243Document7 pages19172243khushi yadavNo ratings yet
- Certificate PDFDocument3 pagesCertificate PDFSudeep MeshramNo ratings yet
- Mani HealthDocument7 pagesMani HealthManish Tewari50% (2)
- Policy 75532363 02122023Document8 pagesPolicy 75532363 02122023kpandya21No ratings yet
- Group Health Insurance Plans in India - SANADocument5 pagesGroup Health Insurance Plans in India - SANArohan kumarNo ratings yet
- JitendraDocument5 pagesJitendrachirag shahNo ratings yet
- PDF 70294786 1694423867565Document8 pagesPDF 70294786 1694423867565Niteshwar Nath [Sales]No ratings yet
- Reliance Healthwise Policy ScheduleDocument2 pagesReliance Healthwise Policy ScheduleueraviNo ratings yet
- GFB 62 23 2925667 000Document5 pagesGFB 62 23 2925667 000Haider BasuwalaNo ratings yet
- 02122020Document5 pages02122020Kumar FanishwarNo ratings yet
- Manipalcigna Prohealth Group Insurance PolicyDocument3 pagesManipalcigna Prohealth Group Insurance PolicykeviletuoNo ratings yet
- Coi 100100193984 03 00Document4 pagesCoi 100100193984 03 00Syam sundharNo ratings yet
- MR Krishna Dhulipala 1-9-485/15/5/ A Plot No: 104, Lalitha Nagar Near Ram Nagar Gundu Hyderabad Musheerabad Musheerabad 500044 Telangana 36Document6 pagesMR Krishna Dhulipala 1-9-485/15/5/ A Plot No: 104, Lalitha Nagar Near Ram Nagar Gundu Hyderabad Musheerabad Musheerabad 500044 Telangana 36dhulipalakrishnakantNo ratings yet
- 5e5a414c4ad34a1297701fba File PDFDocument30 pages5e5a414c4ad34a1297701fba File PDFVishal BothraNo ratings yet
- 5e5a414c4ad34a1297701fba File PDFDocument30 pages5e5a414c4ad34a1297701fba File PDFVishal BothraNo ratings yet
- Policy 73607229 31102023Document8 pagesPolicy 73607229 31102023mohdtanveer550No ratings yet
- CareHealth Policy 2020-21 Nihit FamilyDocument5 pagesCareHealth Policy 2020-21 Nihit FamilyJacob PruittNo ratings yet
- PolicySoftCopy 156477674Document7 pagesPolicySoftCopy 156477674aniket goyalNo ratings yet
- 0287764082 (1)Document8 pages0287764082 (1)rmohanNo ratings yet
- Advantage: A Health Cover For at The Cost of Your Monthly Internet BillDocument4 pagesAdvantage: A Health Cover For at The Cost of Your Monthly Internet BillAmitabh WaghmareNo ratings yet
- FPPack PDFDocument34 pagesFPPack PDFmeet1996No ratings yet
- Policy Mr. Ullas PalDocument11 pagesPolicy Mr. Ullas Palullaspal30No ratings yet
- Insurance SKU158638468362N9SWDocument5 pagesInsurance SKU158638468362N9SWEr Dnyaneshwar PatilNo ratings yet
- Self Health Insurance 80 DDocument3 pagesSelf Health Insurance 80 Dinstatest3580No ratings yet
- PDF 16932270 1584486557515 PDFDocument7 pagesPDF 16932270 1584486557515 PDFLucky TraderNo ratings yet
- 80 D Religare Health Insurace Premium Receipt Rs.21347Document7 pages80 D Religare Health Insurace Premium Receipt Rs.21347Shree Sai Enterprise100% (1)
- Mediclaim - SelfDocument5 pagesMediclaim - SelfParag Parwal0% (1)
- 16648941Document7 pages16648941Manideep AnanthulaNo ratings yet
- Diamond Brochure PDFDocument3 pagesDiamond Brochure PDFSumit SinghNo ratings yet
- PolicySoftCopy 201910201120390513 5dabf5af537a7b2e32033e06 PDFDocument35 pagesPolicySoftCopy 201910201120390513 5dabf5af537a7b2e32033e06 PDFNaveen KrishnaNo ratings yet
- Health Companion UIN: IRDAI/HLT/MBHI/P-H/V.III/2/2017-18Document53 pagesHealth Companion UIN: IRDAI/HLT/MBHI/P-H/V.III/2/2017-18Anil KumarNo ratings yet
- Intermediary Details Name Code Contact Number Shriram City Union Finance LTD 20182494 044-25341413Document4 pagesIntermediary Details Name Code Contact Number Shriram City Union Finance LTD 20182494 044-25341413Gadepilly MaheshNo ratings yet
- PDF 16045523 1571921316928Document5 pagesPDF 16045523 1571921316928Rohit TamuliNo ratings yet
- PDF 16898860 1584486320858 PDFDocument8 pagesPDF 16898860 1584486320858 PDFLucky TraderNo ratings yet
- Insurance Top Up SelfDocument45 pagesInsurance Top Up SelfAbhinav SinhaNo ratings yet
- Screenshot 2024-03-22 at 12.59.42 PMDocument40 pagesScreenshot 2024-03-22 at 12.59.42 PMYash ChaudharyNo ratings yet
- Religare - 80D - Policy - Sukhadeo VibhuteDocument5 pagesReligare - 80D - Policy - Sukhadeo VibhuteArvind kumarNo ratings yet
- Group Medicare Policy ScheduleDocument7 pagesGroup Medicare Policy Scheduleparas INSURANCENo ratings yet
- 23 19 0029367 04Document7 pages23 19 0029367 04josephNo ratings yet
- Policy 30180908 18022021Document7 pagesPolicy 30180908 18022021Lallu KalluNo ratings yet
- NivaBupa 2023Document83 pagesNivaBupa 2023Aniket Yadav100% (1)
- Policy 19718504 22012021Document7 pagesPolicy 19718504 22012021Lallu KalluNo ratings yet
- Personal Protective Equipment (PPE) : By: Erick Chester MagpileDocument33 pagesPersonal Protective Equipment (PPE) : By: Erick Chester MagpileMeghanNo ratings yet
- CT NZ Solutions 2010Document16 pagesCT NZ Solutions 2010Dave MudfordNo ratings yet
- Sales Coaching A Practical Guide For Sales ManagersDocument18 pagesSales Coaching A Practical Guide For Sales ManagersAgnes Yu100% (1)
- University of Dhaka: Google and The Government of China: Cross-Cultural NegotiationDocument8 pagesUniversity of Dhaka: Google and The Government of China: Cross-Cultural NegotiationAsora Yasmin snehaNo ratings yet
- Simple Yes/No Flowchart: What Is The Question To Answer?Document8 pagesSimple Yes/No Flowchart: What Is The Question To Answer?อ้อมใจ ไทรเมฆNo ratings yet
- Fundamentals of Investing: Fourteenth Edition, Global EditionDocument50 pagesFundamentals of Investing: Fourteenth Edition, Global EditionFreed DragsNo ratings yet
- ContinueDocument3 pagesContinueHannah Denise BatallangNo ratings yet
- Basic Jornal Accounting Pratice 1Document20 pagesBasic Jornal Accounting Pratice 1Lakshya AgrawalNo ratings yet
- Sample BudgetDocument109 pagesSample BudgetAnjannette SantosNo ratings yet
- 10 1016@j Iref 2020 06 026Document47 pages10 1016@j Iref 2020 06 026Graphix GurujiNo ratings yet
- Financial Management (Repaired)Document353 pagesFinancial Management (Repaired)Parth PatelNo ratings yet
- CRTF Manual 1.0 PDFDocument8 pagesCRTF Manual 1.0 PDFMuhammad MumtazNo ratings yet
- Cambridge International General Certificate of Secondary EducationDocument12 pagesCambridge International General Certificate of Secondary EducationMike Serge RazafiNo ratings yet
- Buku Teks Part 2Document88 pagesBuku Teks Part 2MAGDALINA BINTI ARIFFIN MoeNo ratings yet
- Big Bazaar Industry Analysis Report NewDocument12 pagesBig Bazaar Industry Analysis Report Newantima shardaNo ratings yet
- ACCCOB2 Introduction To Financial Accounting PPT T1AY2223-1Document25 pagesACCCOB2 Introduction To Financial Accounting PPT T1AY2223-1Clement ChuaNo ratings yet
- 2.EI - CarePlus - Premium Table - e (Jan 20) PDFDocument1 page2.EI - CarePlus - Premium Table - e (Jan 20) PDFYeshma JugdawaNo ratings yet
- Imc Of: Coca ColaDocument31 pagesImc Of: Coca ColaJaanvi GoyalNo ratings yet
- Directory of International Sales AgentsDocument25 pagesDirectory of International Sales AgentsAna De NevadoNo ratings yet
- Capital Budgeting MasDocument6 pagesCapital Budgeting MasHainiel ReforzadoNo ratings yet
- 4 5978943734182578179 PDFDocument3 pages4 5978943734182578179 PDFʚïɞ Fi Fi ʚïɞNo ratings yet
- E02754802 PESA 2022 ElayDocument256 pagesE02754802 PESA 2022 ElayAziel MeloNo ratings yet
- Policy Guidelines For Development of Wayside Amenities Along NHs and ExpresswaysDocument12 pagesPolicy Guidelines For Development of Wayside Amenities Along NHs and Expresswaysrawal_jNo ratings yet
- Industry 4.0 RealDocument8 pagesIndustry 4.0 Realmohan sarasNo ratings yet
- Analisis Lingkungan Bisnis Dalam Meningkatkan Keunggulan Bersaing Café KopilabsDocument9 pagesAnalisis Lingkungan Bisnis Dalam Meningkatkan Keunggulan Bersaing Café KopilabsFitrina SaidNo ratings yet
- Loyola College (Autonomous), Chennai 600034 Department of Commerce (Shift - Ii) Uco1501 Financial Accounting (MC) - Dynamic Question BankDocument12 pagesLoyola College (Autonomous), Chennai 600034 Department of Commerce (Shift - Ii) Uco1501 Financial Accounting (MC) - Dynamic Question BankSam MathewNo ratings yet
- Term Plan ChecklistDocument1 pageTerm Plan ChecklistKumardasNsNo ratings yet
- DAFMDocument337 pagesDAFMShivam GuptaNo ratings yet
- Operations Management Chapter OneDocument24 pagesOperations Management Chapter OneEyob FekaduNo ratings yet
- 1593252702.349 Dsa Empanelment - Form (Reworked)Document5 pages1593252702.349 Dsa Empanelment - Form (Reworked)dhanrajNo ratings yet