You might also like
- Tooth Movement Rate and Anchorage Lost During Canine Retraction: A Maxillary and Mandibular ComparisonDocument7 pagesTooth Movement Rate and Anchorage Lost During Canine Retraction: A Maxillary and Mandibular ComparisonTuanNo ratings yet
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- Stress Distribution in The Abutment and Retention Screw of A Single Implant Supporting A Prosthesis With Platform SwitchingDocument10 pagesStress Distribution in The Abutment and Retention Screw of A Single Implant Supporting A Prosthesis With Platform SwitchingMarlene Kasumi Gantier TakanoNo ratings yet
- Artìculo BaseDocument8 pagesArtìculo BaseYeny Valdivia AlbornozNo ratings yet
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFrom EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiNo ratings yet
- PIIS0889540618306887Document10 pagesPIIS0889540618306887TuanNo ratings yet
- M Ny 5 WP L8 FC BQ 5 Nyhxqt WLNNDocument7 pagesM Ny 5 WP L8 FC BQ 5 Nyhxqt WLNNSyed Mohammad Osama AhsanNo ratings yet
- Short Dental Implants Literature ReviewDocument8 pagesShort Dental Implants Literature Reviewttdqgsbnd100% (1)
- Do Self Ligating Bracket Systems Produce Actual Alveolar Bone Expansion?Document10 pagesDo Self Ligating Bracket Systems Produce Actual Alveolar Bone Expansion?vighanesh kadamNo ratings yet
- Al Thomali 2017Document6 pagesAl Thomali 2017Alejandra CastroNo ratings yet
- Systematic Review of Self-Ligating Brackets. ALVARO CHACONDocument18 pagesSystematic Review of Self-Ligating Brackets. ALVARO CHACONAlvaro ChacónNo ratings yet
- Braquetes Autoligados Ele Promovem o Que PrometemDocument3 pagesBraquetes Autoligados Ele Promovem o Que PrometemMAurcioNo ratings yet
- Effect of Different Incisor Movements On The Soft Tissue Profile (2016)Document9 pagesEffect of Different Incisor Movements On The Soft Tissue Profile (2016)Nicolas ValenzuelaNo ratings yet
- 1 s2.0 S088954061001005X MainDocument6 pages1 s2.0 S088954061001005X MainPanaite TinelaNo ratings yet
- Effects of Third-Order Torque On Frictional Force of Self-Ligating BracketsDocument8 pagesEffects of Third-Order Torque On Frictional Force of Self-Ligating Bracketsmanuela castroNo ratings yet
- Lemos Evaluation of Cement-Retained Versus Screw-Retained Implant-Supported Restorations For Marginal Bone Loss: A Systematic Review and Meta-AnalysisDocument9 pagesLemos Evaluation of Cement-Retained Versus Screw-Retained Implant-Supported Restorations For Marginal Bone Loss: A Systematic Review and Meta-AnalysiseutaNo ratings yet
- The Use of Short Dental Implants in Clinical Practice Literature ReviewDocument7 pagesThe Use of Short Dental Implants in Clinical Practice Literature Reviewd1jim0pynan2No ratings yet
- Occlusal Contacts RetentionDocument9 pagesOcclusal Contacts RetentionRockey ShrivastavaNo ratings yet
- CLR 33 353Document9 pagesCLR 33 353Paul PalomequeNo ratings yet
- 2 Retenedores MandibularesDocument7 pages2 Retenedores MandibularesNeiba RomeroNo ratings yet
- AJODO 07 AutoligadoDocument7 pagesAJODO 07 AutoligadoAngela VillotaNo ratings yet
- 784 2022 Article 4781Document11 pages784 2022 Article 4781Thibaut BossuytNo ratings yet
- Bond Failure of GingivallyDocument5 pagesBond Failure of GingivallyMaria SilvaNo ratings yet
- Fracture Resistance of Endodontically Treated Teeth Without Ferrule Using A Novel H-Shaped Short PostDocument13 pagesFracture Resistance of Endodontically Treated Teeth Without Ferrule Using A Novel H-Shaped Short PostTiago CostaNo ratings yet
- Root Cementum Part 27Document11 pagesRoot Cementum Part 27Sumedha MalshetwarNo ratings yet
- Anterior Tooth Wear and Retention Type Until 5 Years After Orthodontic TreatmentDocument8 pagesAnterior Tooth Wear and Retention Type Until 5 Years After Orthodontic TreatmentRenan VeigaNo ratings yet
- AJODO-98 Clinical Comparison and PerformanceDocument8 pagesAJODO-98 Clinical Comparison and PerformancevaleriaNo ratings yet
- Sys Rev 2013 2Document9 pagesSys Rev 2013 2Hicham AL KHAYARNo ratings yet
- Vohra 2015Document9 pagesVohra 2015Rik ChatterjeeNo ratings yet
- Deguchi, 2011Document9 pagesDeguchi, 2011Laiana LarussaNo ratings yet
- Sobre Dent A Duras 1Document6 pagesSobre Dent A Duras 1LahurentAndresMejíaNo ratings yet
- BDJ 2008 152 PDFDocument5 pagesBDJ 2008 152 PDFlupusebastianNo ratings yet
- Chapter 8Document50 pagesChapter 8Komal TalrejaNo ratings yet
- Bowman 2016Document46 pagesBowman 2016Mirza GlusacNo ratings yet
- Pressure Transmission and Distribution Under Denture Bases Using Denture Teeth With Different Materials and Cuspal AngulationsDocument10 pagesPressure Transmission and Distribution Under Denture Bases Using Denture Teeth With Different Materials and Cuspal AngulationsRaul MirandaNo ratings yet
- Barrett Nordstrom Toshihiro Shoji W. Cameron Anderson Henry W. Fields Jr. F. Michael Beck Do-Gyoon Kim Teruko Takano-Yamamoto Toru DeguchiDocument7 pagesBarrett Nordstrom Toshihiro Shoji W. Cameron Anderson Henry W. Fields Jr. F. Michael Beck Do-Gyoon Kim Teruko Takano-Yamamoto Toru DeguchirigaNo ratings yet
- Bone Augmentation of The Edentulous Maxilla For Implant Placement: A Systematic ReviewDocument12 pagesBone Augmentation of The Edentulous Maxilla For Implant Placement: A Systematic ReviewJarvin Miguel Buitrago GalindezNo ratings yet
- 15 Years Rand Cobtrolled Trial 2011Document7 pages15 Years Rand Cobtrolled Trial 2011Hicham AL KHAYARNo ratings yet
- Analysis of Lingual en Masse Retraction CombiningDocument9 pagesAnalysis of Lingual en Masse Retraction Combiningandres belloNo ratings yet
- Fracture of Dental Implants Literature Review and Report of A CaseDocument6 pagesFracture of Dental Implants Literature Review and Report of A Casec5sdvcgdNo ratings yet
- Lemos 2016Document32 pagesLemos 2016wendyjemmy8gmailcomNo ratings yet
- Is Ridge Preservation Effective in The Extraction Sockets of Periodontally Compromised Teeth? A Randomized Controlled TrialDocument32 pagesIs Ridge Preservation Effective in The Extraction Sockets of Periodontally Compromised Teeth? A Randomized Controlled TrialmmputraNo ratings yet
- Eross 2015Document9 pagesEross 2015serahNo ratings yet
- 2021 In-Vitro Fatigue Performance Connection PRAMADocument7 pages2021 In-Vitro Fatigue Performance Connection PRAMASahasraNo ratings yet
- Self-Ligating Brackets Present and FutureDocument8 pagesSelf-Ligating Brackets Present and FutureVijay Prabu GNo ratings yet
- Kortam Sahira IbrahimDocument77 pagesKortam Sahira Ibrahimjuanita_luna_7No ratings yet
- 2016 ClinOraInvest Moninietal LowercanineretractionandlossofanchorageDocument8 pages2016 ClinOraInvest Moninietal LowercanineretractionandlossofanchorageabocoliNo ratings yet
- Influência Das Forças Rotacionais Na Estabilidade Pode Ser Minimizada Por Jateamento - KIMDocument9 pagesInfluência Das Forças Rotacionais Na Estabilidade Pode Ser Minimizada Por Jateamento - KIMUrsula Pantigozo MoránNo ratings yet
- PROTOCOLO de Carga de Coronas Sobre ImplanteDocument17 pagesPROTOCOLO de Carga de Coronas Sobre ImplanteJohnny CHNo ratings yet
- Complications Associated With The Ball, Bar and Locator Attachments For Implant-Supported OverdenturesDocument7 pagesComplications Associated With The Ball, Bar and Locator Attachments For Implant-Supported OverdenturesDr FarhatNo ratings yet
- Importance of Attachments in Treatment With Clear Aligners: A Narrative ReviewDocument7 pagesImportance of Attachments in Treatment With Clear Aligners: A Narrative ReviewAya ElsayedNo ratings yet
- Biomechanical Analysis of Miniscrew-Assisted MolarDocument9 pagesBiomechanical Analysis of Miniscrew-Assisted Molarmobinali19901No ratings yet
- IJOMI 2015 Thematic Extract - C I RatioDocument3 pagesIJOMI 2015 Thematic Extract - C I RatioZhiyi LinNo ratings yet
- Fixed Versus Removable Orthodontic Appliances To Correct Anterior Crossbite in The Mixed Dentition-A Randomized Controlled Trial PDFDocument6 pagesFixed Versus Removable Orthodontic Appliances To Correct Anterior Crossbite in The Mixed Dentition-A Randomized Controlled Trial PDFJejeNo ratings yet
- Predictability of Short Dental Implants A Literature ReviewDocument7 pagesPredictability of Short Dental Implants A Literature Reviewea428adhNo ratings yet
- Caninos RetenidosDocument9 pagesCaninos RetenidosNayely MiguelNo ratings yet
- Extraction Socket Presenvation Using A Collagen Plug Combined With Platelet Rich Plasma (PRP) RADIOGRAPIHICDocument7 pagesExtraction Socket Presenvation Using A Collagen Plug Combined With Platelet Rich Plasma (PRP) RADIOGRAPIHICrachmadyNo ratings yet
- The Size of Occlusal Rest Seats PreparedDocument7 pagesThe Size of Occlusal Rest Seats PreparedPatra PrimadanaNo ratings yet
- A Look at Forensic Dentistry - Part 1: The Role of Teeth in The Determination of Human IdentityDocument8 pagesA Look at Forensic Dentistry - Part 1: The Role of Teeth in The Determination of Human IdentityJEAN BAILEY RAMOS ROXASNo ratings yet
- Ijomi 15 415Document4 pagesIjomi 15 415Bagis Emre GulNo ratings yet
- The Effect of A Lucia Jig For 30 MinutesDocument6 pagesThe Effect of A Lucia Jig For 30 Minutesd.diazNo ratings yet
- Step by Step Root Canal TreatmentDocument157 pagesStep by Step Root Canal TreatmentKaaroma Tamoaieta100% (1)
- 06200119-R6 Manuale-Isykone EngDocument48 pages06200119-R6 Manuale-Isykone EngsfaquiraNo ratings yet
- Health Teaching About Hygiene For TeensDocument8 pagesHealth Teaching About Hygiene For TeensAyna Salic PangarunganNo ratings yet
- Analysis of Ions in The ToothpasteDocument10 pagesAnalysis of Ions in The ToothpasteKalika SinghNo ratings yet
- Dentsply GAC - CatalogDocument336 pagesDentsply GAC - Catalogsorc50% (2)
- Ricketts Cephalometric Syntesis PDFDocument27 pagesRicketts Cephalometric Syntesis PDFAleeJanyArroNo ratings yet
- MBT Versatile Bracket Placement Guide Ifu PDFDocument1 pageMBT Versatile Bracket Placement Guide Ifu PDFmonwarul azizNo ratings yet
- Essential Hospital Bag Checklist: General Necessities For Your Baby ClothingDocument2 pagesEssential Hospital Bag Checklist: General Necessities For Your Baby ClothingSilvestre תזשק WolfNo ratings yet
- College of Dentistry BAMDCDocument14 pagesCollege of Dentistry BAMDCTazeem KhanNo ratings yet
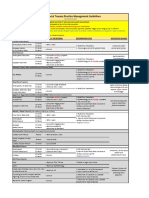
- VUMC Facial Trauma Practice Management GuidelinesDocument1 pageVUMC Facial Trauma Practice Management GuidelinesIndra D KristionoNo ratings yet
- Radiographic Features of RL LesionsDocument7 pagesRadiographic Features of RL Lesionszyad ahmedNo ratings yet
- Dentists Decisions Regarding The Need For Cuspal PDFDocument10 pagesDentists Decisions Regarding The Need For Cuspal PDFRohma DwiNo ratings yet
- 2the Effective of Photobiomodulation Therapy On Accelerating Orthodontic MovementDocument22 pages2the Effective of Photobiomodulation Therapy On Accelerating Orthodontic MovementPratNo ratings yet
- .Arnett AnalysisDocument6 pages.Arnett AnalysisMariyam100% (2)
- Adding New Teeth in DentureDocument2 pagesAdding New Teeth in DenturebabukanchaNo ratings yet
- Regeneration in Immature Permanent TeethDocument7 pagesRegeneration in Immature Permanent Teethmounica kadaliNo ratings yet
- Policy On Early Childhood Caries (ECC) - Classifications, Consequences, and Preventive StrategiesDocument4 pagesPolicy On Early Childhood Caries (ECC) - Classifications, Consequences, and Preventive StrategiesJeje100% (1)
- Cysts of The JawsDocument25 pagesCysts of The Jawsluna zeidNo ratings yet
- 1 eNDODONTICS To PrintDocument19 pages1 eNDODONTICS To PrintDENTAL REVIEWER ONLYNo ratings yet
- Community Directory (May 2023)Document32 pagesCommunity Directory (May 2023)The Livingston County NewsNo ratings yet
- Chapter 2: Operative Dentistry and Prosthodontics: AnswersDocument13 pagesChapter 2: Operative Dentistry and Prosthodontics: AnswersBinayak UpadhyayaNo ratings yet
- Kuk 253Document28 pagesKuk 253Kuk-Punjabi SamacharNo ratings yet
- Austin Journal of DentistryDocument8 pagesAustin Journal of DentistryAustin Publishing GroupNo ratings yet
- Dental Important Implant-BrochureDocument5 pagesDental Important Implant-BrochureKothapalli ChiranjeeviNo ratings yet
- CD Bernard LevinDocument172 pagesCD Bernard LevinIndrani Das50% (2)
- What Is Root Canal Treatment?Document2 pagesWhat Is Root Canal Treatment?Vishakha SabooNo ratings yet
- Patient Examination and Assessment: Subir Banerji and Shamir MehtaDocument45 pagesPatient Examination and Assessment: Subir Banerji and Shamir MehtaAdriana RibeiroNo ratings yet
- Cable Supported Bridges: Concept and DesignFrom EverandCable Supported Bridges: Concept and DesignRating: 5 out of 5 stars5/5 (1)
- The Great Bridge: The Epic Story of the Building of the Brooklyn BridgeFrom EverandThe Great Bridge: The Epic Story of the Building of the Brooklyn BridgeRating: 4.5 out of 5 stars4.5/5 (59)
- The Things We Make: The Unknown History of Invention from Cathedrals to Soda Cans (Father's Day Gift for Science and Engineering Curious Dads)From EverandThe Things We Make: The Unknown History of Invention from Cathedrals to Soda Cans (Father's Day Gift for Science and Engineering Curious Dads)No ratings yet
- Crossings: How Road Ecology Is Shaping the Future of Our PlanetFrom EverandCrossings: How Road Ecology Is Shaping the Future of Our PlanetRating: 4.5 out of 5 stars4.5/5 (10)
- The Things We Make: The Unknown History of Invention from Cathedrals to Soda CansFrom EverandThe Things We Make: The Unknown History of Invention from Cathedrals to Soda CansRating: 4.5 out of 5 stars4.5/5 (22)
- Structural Health MonitoringFrom EverandStructural Health MonitoringDaniel BalageasNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Connections in Steel Structures III: Behaviour, Strength and DesignFrom EverandConnections in Steel Structures III: Behaviour, Strength and DesignRating: 4 out of 5 stars4/5 (6)
- Shallow Foundations: Discussions and Problem SolvingFrom EverandShallow Foundations: Discussions and Problem SolvingRating: 5 out of 5 stars5/5 (1)
- Geotechnical Engineering Calculations and Rules of ThumbFrom EverandGeotechnical Engineering Calculations and Rules of ThumbRating: 4 out of 5 stars4/5 (17)
- The Big Roads: The Untold Story of the Engineers, Visionaries, and Trailblazers Who Created the American SuperhighwaysFrom EverandThe Big Roads: The Untold Story of the Engineers, Visionaries, and Trailblazers Who Created the American SuperhighwaysRating: 4 out of 5 stars4/5 (19)
- Operations in the Time of Industry 4.0: A guide to managing the clash of digitalization and real time operationsFrom EverandOperations in the Time of Industry 4.0: A guide to managing the clash of digitalization and real time operationsNo ratings yet
- To Engineer Is Human: The Role of Failure in Successful DesignFrom EverandTo Engineer Is Human: The Role of Failure in Successful DesignRating: 4 out of 5 stars4/5 (138)
- Principles of Forensic Engineering Applied to Industrial AccidentsFrom EverandPrinciples of Forensic Engineering Applied to Industrial AccidentsNo ratings yet
- Safety and Intelligent Transport Systems Development in the People’s Republic of ChinaFrom EverandSafety and Intelligent Transport Systems Development in the People’s Republic of ChinaNo ratings yet
- Environmental Impact Assessment: Theory and PracticeFrom EverandEnvironmental Impact Assessment: Theory and PracticeRating: 5 out of 5 stars5/5 (5)
- Bridge Engineering: Classifications, Design Loading, and Analysis MethodsFrom EverandBridge Engineering: Classifications, Design Loading, and Analysis MethodsRating: 4 out of 5 stars4/5 (16)
- The Finite Element Method: Linear Static and Dynamic Finite Element AnalysisFrom EverandThe Finite Element Method: Linear Static and Dynamic Finite Element AnalysisRating: 5 out of 5 stars5/5 (3)